Krishna Foundation`s Jaywant Institute of Pharmacy, Wathar, Karad, Maharashtra 415539
Polycystic ovary syndrome (PCOS) impacts 4-20% of women globally, featuring irregular periods, infertility, hirsutism, obesity, and cystic ovaries, while driving insulin resistance and risks like diabetes, cardiovascular issues, hypertension, dyslipidemia, and cancers due to unclear pathophysiology involving hypothalamic-pituitary-ovarian axis dysregulation. First- line management focuses on lifestyle shifts, including low-calorie, low-GI, high-fiber, omega- 3-rich, ketogenic, Mediterranean, antioxidant, and anti-inflammatory diets to enhance insulin sensitivity, hormonal balance, and weight. Ayurveda provides personalized, side-effect-free relief by targeting root causes—regularizing cycles, controlling blood sugar and weight, boosting fertility, and reducing stress—making nutrition strategies, neuroendocrine control, lifestyle changes, and Ayurvedic interventions key for effective PCOS symptom management.
Polycystic Ovary Syndrome (PCOS) is a common endocrine disorder in women of reproductive age, characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovaries. It is not only a reproductive disorder but also a metabolic and neuroendocrine condition, associated with insulin resistance, obesity, and HPO-axis imbalance.
PCOD is a milder form where ovulation occurs irregularly, while PCOS involves chronic anovulation, high androgens, and greater metabolic risk.
HISTORICAL BACKGROUND
Ancient References (400 BCE – 1700s):
Ancient medical texts (like Hippocrates, ~400 BCE) described women with “masculine traits” such as infertility, irregular periods, and excessive hair growth. While not called PCOS then, these were likely early descriptions. In the 18th century, physicians began noticing enlarged ovaries during autopsies of women with menstrual and fertility problems.
The 19th Century: First Medical Observations
1844 – Dr. Chereau (France) described sclerocystic ovaries in women who had irregular menstruation and infertility.
1895 – Rokitansky noted the association between ovarian enlargement and abnormal menstrual cycles.These reports laid the groundwork for linking ovarian changes with reproductive disorders.
1935 – The Stein-Leventhal Syndrome:
Dr. Irving F. Stein Sr. and Dr. Michael L. Leventhal (Chicago, USA) published their landmark paper.They described seven women with Enlarged polycystic ovaries, Irregular or absent menstruation, Infertility & Hirsutism (excess hair growth). After performing bilateral ovarian wedge resections, 5 of the 7 women regained normal menstruation and some conceived.This condition became known as the Stein-Leventhal Syndrome.
Mid–20th Century (1940s–1970s): Endocrine Understanding
Doctors discovered that women with the syndrome often had high levels of luteinizing hormone (LH) and androgens (male hormones).The link with insulin resistance began to emerge by the late 1960s and 70s.By this point, PCOS was recognized not only as a reproductive disorder but also as a metabolic condition.
Late 20th Century (1980s–1990s): Modernization of Diagnosis
Ultrasound imaging made it possible to directly see “polycystic ovaries.” In 1990 (NIH Conference, USA),PCOS was defined as chronic anovulation + hyperandrogenism, after excluding other causes.
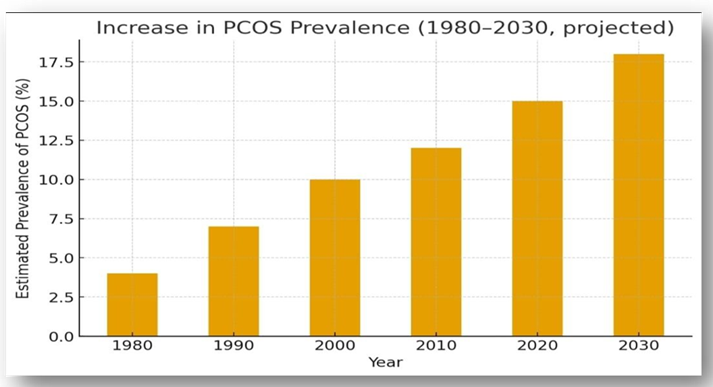
Fig 1.1 : Historical Background of PCOS
2003 (Rotterdam Criteria, Europe):
Diagnosis required two of three: Irregular ovulation/periods, High androgen levels (clinical or biochemical) or Polycystic ovaries on ultrasound
21st Century: Beyond Reproduction
PCOS is now recognized as a lifelong syndrome affecting not just fertility, but also metabolic health, mental health, and long-term risks (e.g., diabetes, cardiovascular disease).Research continues into genetics, insulin resistance, inflammation, and environmental triggers (like endocrine-disrupting chemicals).
TYPES OF PCOS
Based on Rotterdam criteria, PCOS is classified into four phenotypes:
Table 1.1 Types Of PCOS
|
|
Phenotype A |
Phenotype B |
Phenotype C |
Phenotype D |
|
Hyperandrogenism & Hirsutisum |
ü |
ü |
ü |
û |
|
Ovulatory dysfunction |
ü |
ü |
ü |
û |
|
POMS |
ü |
û |
û |
û |
PATHOPHYSIOLOGY
Abnormal GnRH secretion increases LH over FSH, stimulating ovarian androgen production. High androgens impair follicle development, causing anovulation, cyst formation, acne, and hirsutism.
Insulin resistance worsens androgen excess and leads to metabolic and reproductive dysfunction.
CAUSES
Polycystic Ovary Syndrome (PCOS) is a common hormonal disorder that affects people with ovaries, typically during their reproductive years. The exact cause of PCOS is not fully understood, but several interrelated factors are believed to contribute to its development such as Hormonal imbalance (high androgens, low progesterone), Insulin resistance, Genetic predisposition, Inflammation, Lifestyle factors (diet, inactivity, stress), Obesity, thyroid disorders, adrenal dysfunction, vitamin D deficiency etc.
SYMPTOMS
PCOS include symptoms like Irregular or absent periods, Infertility, Hirsutism, acne, hair loss, Weight gain, insulin resistance, Anxiety and depression
HORMONAL CHANGES
Table 1.2: Hormonal Changes
|
Sr. No. |
Hormone Change |
Effect |
Clinical Feature |
|
1. |
↑ Luteinizing Hormone (LH) |
Stimulate Androgen Production |
Hyperandrogenism |
|
2. |
↓ Follicle Stimulating Hormone (FSH) |
Impair Follicle Maturation |
Anovulation, Irregular Menstrution |
|
3. |
↑ Androgens |
Excess Androgens |
Hirsutism, Acne, Hair Loss |
|
4. |
↓ Sex Hormone- Binding Globulin |
More Free Androgens |
Exacerbated Hyperandrogenic Symptoms |
|
5. |
↑ Estrogens |
Chronic Low-level Estrogen Secretion |
Risk Of Endometrial Hyperplasia |
|
6. |
↑ Insulin |
Worsens Hyperandrogenisum |
Metabolic Issues |
ROLE OF NUTRITION
A PCOS-friendly diet for example Low-GI, high-fiber carbohydrates ,Adequate protein and omega-3 fats ,Micronutrients like Vitamin D, B12, magnesium, zinc, chromium, selenium , also Mediterranean and plant-based diets improve insulin resistance and ovulation.
LIFESTYLE MANAGEMENT
Lifestyle modification is considered the first-line therapy for PCOS by international guidelines because it improves metabolic, hormonal, and reproductive outcomes. It includes 5–10% weight loss ,Regular exercise ,Healthy low-GI diet ,Adequate sleep (7–9 hours) ,Stress management (yoga, meditation)
AYURVEDIC MANAGEMENT
PCOS is related to Kapha and Vata imbalance in Ayurveda.Important herbs like Shatavari, Ashwagandha, Guduchi, Triphala, Fenugreek, Guggulu. These help in hormone balance, insulin sensitivity, weight control, and ovarian function. Panchakarma therapies detoxify and restore balance.
AYURVEDA vs ALLOPATHY
Ayurveda treats the root cause, improves lifestyle, and balances hormones naturally while Allopathy provides quick symptom control using drugs and hormones. Both systems are useful, but Ayurveda is especially beneficial for long-term PCOS management.
OBJECTIVE
DISCUSSION
The study confirms that Polycystic Ovary Syndrome (PCOS) is a metabolic–endocrine disorder involving hormonal, metabolic, and ovarian abnormalities.
These findings confirm PCOS as a chronic endocrine–metabolic disorder, not just a reproductive problem.
PCOS develops due to neuroendocrine and metabolic imbalance. Excess GnRH → high LH → increased ovarian androgens, while insulin resistance further raises androgen levels and suppresses SHBG, leading to ovulation failure.
Lifestyle factors such as poor diet, obesity, and stress worsen hormonal imbalance. Even 5– 10% weight loss significantly improves ovulation and insulin sensitivity.
Role of Ayurvedic Herbs
Ayurveda views PCOS as Kapha–Vata imbalance with metabolic blockage. Herbs correct the root cause by improving metabolism, hormones, and ovarian function.
Table 1.3: Herbs and Actions
|
Herb |
Main Role in PCOS |
|
Shatavari |
Regulates female hormones, improves ovulation |
|
Ashwagandha |
Reduces stress, balances cortisol and LH/FSH |
|
Guduchi |
Improves insulin sensitivity, reduces inflammation |
|
Triphala |
Detoxifies, improves metabolism and gut health |
|
Fenugreek |
Lowers insulin resistance and androgens |
|
Kanchanar |
Reduces cysts, supports thyroid and fat metabolism |
|
Licorice |
Lowers testosterone, improves acne & hirsutism |
|
Gokshura |
Supports ovarian and hormonal balance |
PCOS is a multifactorial disorder involving hormonal imbalance, insulin resistance, ovarian dysfunction, and psychological stress.
Modern medicine controls symptoms, while Ayurvedic herbs correct metabolism, reduce androgens, improve ovulation, and support long-term hormonal balance.
An integrated approach of diet, exercise, stress control, modern therapy, and Ayurveda provides the best and most sustainable management of PCOS.
CONCLUSION
Polycystic Ovary Syndrome (PCOS) is a hormonal and metabolic disorder influenced by genetic and environmental factors. It disrupts the hypothalamic–pituitary–ovarian (HPO) axis, leading to high androgen levels, irregular ovulation, and insulin resistance. Therefore, PCOS management should focus on correcting these metabolic and neuroendocrine imbalances.
A balanced diet rich in low-glycemic foods, fiber, lean proteins, and omega-3 fatty acids helps improve insulin sensitivity, control weight, and regulate menstruation. Avoiding processed foods and sugars reduces inflammation and hormonal imbalance.
Stress management, proper sleep, yoga, and meditation help regulate hormones such as GnRH, LH, and FSH, supporting reproductive health. Regular physical activity further enhances insulin sensitivity and prevents long-term complications.
Ayurveda considers PCOS a disorder of Kapha and Vata imbalance. Treatments such as Panchakarma, herbal medicines like Shatavari, Ashwagandha, Guduchi, and Triphala, along with yoga and diet, help restore hormonal balance and ovarian function.
In conclusion, an integrated approach combining nutrition, lifestyle modification, and Ayurvedic therapy offers an effective natural strategy for managing PCOS and improving overall reproductive and metabolic health.
REFERENCES







Sayama Nadaf, Alfiya Mujawar, Om Niprul, Sanika Mote, Sanika Mali, Sushant Mohite, Suraj Jadhav, Dr. Bhagyesh Janugade, A Systemic Review: Nutrition Strategy, Neuroendocrine Control & Lifestyle in Polycystic Ovary Syndrome, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 583-590. https://doi.org/10.5281/zenodo.18894086
 10.5281/zenodo.18894086
10.5281/zenodo.18894086
