Malla Reddy Pharmacy College.
PURPOSE: The main aim of the study was to evaluate the antibiotics usage trends in a tertiary care setting through drug utilization evaluation technique. METHODOLOGY: It is a hospital based prospective observational study conducted in inpatients of 5 different departments. The duration of study was 6 months. A total of 207 patients were enrolled in the study as per the inclusion criteria. The data was collected from the patient case reports/case sheets, and a questionnaire was performed. The data collected was recorded, analyzed and results were extracted. RESULTS: According to our study, most of the patients receiving antibiotics were in the age group of 31-40 years. Most of the antibiotics are used in the general surgery department. Most of the patients were prescribed one antibiotic, 93.2%of patients were prescribed antibiotics without any prior microbial culture test. Generic prescribing of antibiotics is only 13%. The most prescribed antibiotics were Monocef (ceftriaxone) followed by Amikacin, Augmentin etc. CONCLUSION: Our study concluded that most of the antibiotics were prescribed in brand names. Irrational prescribing of antibiotics, like the prescribing of antibiotics without culture sensitivity tests and prescribing of parenteral antibiotics for longer durations was observed.
Antibiotics are among the most often given medications worldwide and are very important in the fight against bacterial diseases including urinary tract infections and respiratory tract infections (whooping cough, pneumonia). Their extensive usage has, however, brought various difficulties including antibiotic resistance, side effects from medications, and rising healthcare costs. [1] Promoting the prudent use of antibiotics is a major focus of global health projects as inappropriate prescription practices may aggravate resistance problems and compromise patient outcomes. Antimicrobial drugs form the foundation of contemporary medical practice. However, the development and proliferation of pathogens resistant to these medications pose a significant threat to our capacity to manage common infections and conduct crucial medical procedures. There are four ways of action behind bacterial resistance. Antibiotic inactivation or modification: bacteria create enzymes that degrade and inactivate antibiotics (e.g., beta-lactamase an enzyme created by bacteria against penicillin and cephalosporin). Change in target or binding site (e.g., methicillin-resistant staphylococcus aureus.). Overcoming metabolic inhibition: certain bacteria scavenge folic acid from the surroundings entirely, therefore bypassing the effect of sulfonamides.[2] By lowering the bacterial membrane's permeability and thereby preventing the antibiotic accumulation. The World Health Organization describes drug utilization evaluation, as a continuous, systematic process for quality enhancement that aims to ensure medications are used effectively and appropriately. [3] This process is designed to examine patterns of drug use and prescription, disseminate findings to medical professionals and other pertinent groups, establish criteria and benchmarks for optimal medication use, encourage proper drug usage through educational initiatives and other measures. DUE may greatly help to clarify the knowledge, interpretation, and improvement of pharmaceutical prescription, administration, and use procedures of the healthcare system.
Drug Profile:
A) Amoxicillin
Amoxicillin is FDA approved drug that is a widely utilized beta-lactam antibiotic.
Indications:
FDA approved: When administered as directed, it may alleviate illnesses brought on by some types of bacteria that are sensitive to it, but do not produce beta-lactamase in the cases described below. Acute bacterial sinusitis, UTI, Helicobacter pylori eradication, LRTI
Off-label uses used to treat Lyne disease if there are contraindications for doxycycline.
Mode of action:
Majority of the bacteria contain an unyielding cell wall that contribute to structural integrity. This wall consists of peptidoglycan, composed of interconnected glycan (polysaccharide) chains. The glycan chains contain repeating units of N-acetylmuramic acid (NAcM) and N-acetylglucosamine (NAcG). Pentapeptide side chains attached to Cell wall synthesis inhibitors interfere with PBP-mediated processes. This results in defective cell wall development, leading to osmotic imbalance and eventual bacterial cell rupture. Penicillin is thus bactericidal, targeting cell wall synthesis and causing bacterial lysis. Their effectiveness against Gram-positive bacteria is higher than that against Gram-negative bacteria.
Pharmacokinetic parameters:
Absorption: Rapid oral absorption occurs with an average Cmax within one to two hours, and it remains stable when exposed to stomach acid.
Adverse drug reaction:
Although amoxicillin is usually well-tolerated, it does have the potential to cause the usual gastrointestinal side effects such nausea, vomiting, and diarrhea on rare occasions. Hematological symptoms (hemolytic anemia, thrombocytopenia, and leukopenia), nephrotoxicity, hypersensitivity responses, and hepatotoxicity are further adverse drug reactions (ADRs) linked to amoxicillin.[4]
B) Ceftriaxone:
Ceftriaxone is a 3rd generation cephalosporin antibiotic with magnificent activity against gram-negative bacteria. It is effective in the cure of complicated and uncomplicated UTI, LRTI, etc.
Indications:
FDA-approved: acute bacterial otitis media, pelvic inflammatory disease, meningitis, acute uncomplicated pyelonephritis, surgical prophylaxis, and gonococcal infections. Off-label uses septic shock, acute epididymitis, acute bacterial rhino sinusitis.
Mode of action: Although it works better against resistant species, this third-generation cephalosporin antibiotic, which is broad-spectrum and gram-negative, has limited effectiveness against gram-positive bacteria. By attaching to one or more PBPs, which impede the fusing of peptidoglycans—a main and crucial component of the bacterial cell wall—this inhibits the formation of the cell wall. This leads to the death of bacteria in the long run.
Pharmacokinetic parameters:
Absorption: It is well absorbed through the IM route of administration. Cmax 2-3 hours.
Distribution: 85-95% is bound to plasma proteins
Metabolism: metabolized in the liver
Elimination: half-life of elimination 5–9 hours in healthy kidneys and livers, 12–16 hours in moderate to severe kidney disease. Urine excretes 33–67 percent of the medication in its unaltered form.
Adult dose: 1g/50ml/IM
Adverse drug reactions:
Oliguria, Steven Johnson syndrome, stomatitis, pancreatitis, dermatitis, seizures, acute renal failure
Note: lidocaine contraindicates if lidocaine solution is used as a solvent with ceftriaxone for IM injection.[5]
C) Tetracycline:
Broad-spectrum antibiotics that inhibit protein synthesis, tetracyclines are used to treat and control a variety of bacterial illnesses.
Indications:
Applied in the cure of actinomycosis, syphilis, gonorrhea, uncomplicated urethral endocervical or rectal infections, moderate to severe acne, chronic bronchitis, and acute exacerbations.
Mode of action:
These drugs act by reversibly binding to 30s ribosomal subunits and passively diffusing through porin channels in the bacterial membrane, tetracyclines inhibit tRNAs' ability to attach to mRNA ribosomal complex, hence impeding protein synthesis.
Pharmacokinetic parameters:
Adverse drug reactions: epigastric distress, esophagitis, inflammatory lesions in the Ano genital area, enamel hypoplasia, hepatotoxicity, liver failure, hemolytic anemia, pericarditis, hypersensitivity reactions, and renal toxicity. [6]
D) Azithromycin:
Azithromycin is an anti-microbial agent included in the class of macrolides which is utilized in the treatment and control bacterial infections such as STDs and community-acquired pneumonia.
Indications:
FDA approved: Community-acquired pneumonia, pharyngitis, COPD, micro bacterial infections, genital ulcer disease.
Off-label uses: Covid 19, Cat scratch disease, and endocarditis.
Mechanism of action:
Azithromycin reversibly binds to the ribosomal 50s subunit of the bacteria and hinder the translation of mRNA and thereby inhibits bacterial protein assimilation.
Adverse effects:
Rashes, fever, eosinophilia, skin eruptions, cholestatic hepatitis, epigastric pain, thrombophlebitis etc.
Pharmacokinetic parameters:
Adverse drug reaction:
Generally, azithromycin is a safer antibiotic and has fewer cardiac effects when compared to other macrolides. Very few of the patients discontinue Azithromycin due to ADRs as follows: QTc prolongation, polymorphic ventricular tachycardia, rarely hepatotoxicity (with elevated transaminase concentration, cholestatic jaundice). [7]
E) Trimethoprim-Sulfamethoxazole:
This is also known as co-trimoxazole. It is an antimicrobial agent that is used to treat and prevent bacterial infection. Trimethoprim Sulfamethoxazole is abbreviated as TMP-SMZ. This composition is particularly impactful against numerous aerobic enteric bacteria excluding “pseudomonas aeruginosa”.
Indications
FDA approved: UTI, acute exacerbation of chronic bronchitis, traveler's diarrhea treatment and prophylaxis, shigellosis, toxoplasmosis (treatment and prophylaxis), otitis media (only in pediatrics).
Off label uses acne vulgaris, TB, listeria, pertussis, malaria, In HIV patients, community-acquired pneumonia.
Mode of action:
This drug mainly acts by inhibiting the folic acid synthesis inside the bacteria. Sulfamethoxazole acts as a direct competitor for PABA and Trimethoprim acts as a direct competitor for an enzyme dihydrofolate reductase causing the inhibition of tetrahydrofolate’s production to its active form which is fundamental for the formation of the genetic material of bacteria. Thereby it results in inhibition of bacterial growth
Pharmacokinetic parameters:
E) Ciprofloxacin
Second-generation fluoroquinolone antibiotic ciprofloxacin treats many bacterial illnesses including pneumonia and urinary tract infections.
FDA-approved indications: ciprofloxacin can be applied in the treatment of UTIs, gonorrhea, chancroid, prostatitis, typhoid fever, GI infections, LRTIs, anthrax, plague, corneal ulcers, conjunctivitis, etc.
Mode of action:
Ciprofloxacin is a bactericidal drug that pertain to the class called fluoroquinolone antibiotic. It acts by blocking the actions of bacterial DNA gyrase and DNA topoisomerase enzymes which are needed for bacterial DNA replication and separation of bacterial daughter cells separation respectively.
Pharmacokinetic parameters:
Adverse drug reactions: the major side effects of ciprofloxacin include, joint, muscle, and tendon pain associated with swelling or stiffness, allergic reactions, heart rhythm changes, mood, and behavioral changes, etc. [10]
F) Rifampicin
Derived from rifamycin, rifampicin is the first-line antitubercular medication.
FDA-approved indications: Neisseria meningitidis carrier may be treated with rifampicin, as can TB.
Off-label indications: include leprosy, Haemophiles Influenzae Type B infection.
Strength and form of dosage: The capsule weights 150 mg, 300 mg. 600 mg injectable powder.
Mode of action:
Rifampicin acts bactericidally. It suppresses RNA synthesis by binding to bacterial DNA-dependent RNA polymerase, therefore blocking RNA transcription, a strong enzyme inducer.
Pharmacokinetic parameters:
Adverse effects: The main adverse effects of ciprofloxacin include hepatotoxicity, headache, muscular and joint pain, flushing, and GI problems including nausea, vomiting, and stomachache.[11]
Aim And Objectives:
Aim: To evaluate the drug use evaluation of antibiotics in a tertiary care hospital.
Objectives: Assess usage patterns: analyze the current patterns of antibiotic use within a specific setting to determine adherence to guidelines and identify trends. Identify inappropriate prescribing: analyze data to uncover instances where antibiotics are not prescribed appropriately, such as for viral infections or without a clear indication. Assess the most prescribed antibiotics. Develop recommendations: formulate evidence-based recommendations for improving antibiotic utilization practice based on findings.
Inclusion Criteria: Inpatients of all age groups from General Medicine, General Surgery, Orthopedics, Pediatrics, and Pulmonology departments. Inpatients prescriptions containing at least one antibiotic. Prescription containing at least one antibiotic prescribed for main therapy or prophylactic treatment. Oral and I.V. antibiotics. Patients with other comorbid conditions.
Exclusion Criteria: Outpatients of General Medicine, General Surgery, Orthopedics, Pediatrics and Pulmonology departments. Inpatients and Outpatients of other departments which are not included in the inclusion criteria. Patients with chronic infections requiring long-term therapy. Patients with incomplete data and medical charts without antibiotics were excluded.
Study Site: The study was conducted in the Malla Reddy Hospital
Study Design: Prospective observational study
Study Period: The study was carried out for 6 months
Sample Size: 207
RESULTS
Table 1: Distribution of patients based on gender
|
Gender |
No. of Subjects |
Percentage |
|
Male |
126 |
60.9% |
|
Female |
81 |
39.1% |
|
Total |
207 |
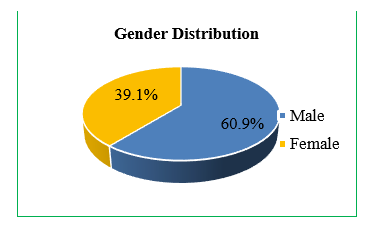
Fig 1. Graphical presentation of gender
Table 2: Distribution of patients based on age
|
Age (Years) |
No. of Subjects |
Percentage |
|
0 – 10 |
15 |
7.2% |
|
11 – 20 |
17 |
8.2% |
|
21 – 30 |
23 |
11.1% |
|
31 – 40 |
45 |
21.7% |
|
41 – 50 |
28 |
13.5% |
|
51 – 60 |
32 |
15.5% |
|
61 – 70 |
31 |
15.0% |
|
71 & above |
16 |
7.7% |
|
Total |
207 |
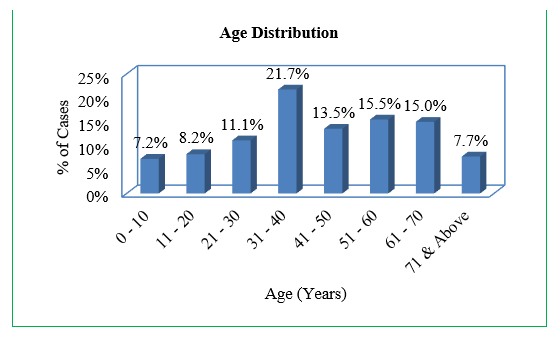
Figure 2: Graphical presentation of age group
Table 3: Distribution of patients according to department
|
Department |
No. of Subjects |
Percentage |
|
GS |
91 |
44.0% |
|
GM |
42 |
20.3% |
|
Orthopedics |
35 |
16.9% |
|
Pediatrics |
23 |
11.1% |
|
Respiratory |
16 |
7.7% |
|
Total |
207 |
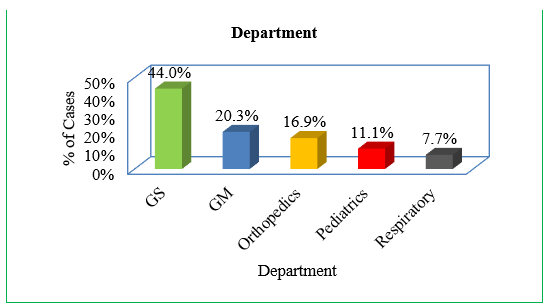
Figure 3: Graphical presentation of department
Table 4: Distribution of patients according to type of therapy received
|
Type of Therapy |
No. of Subjects |
Percentage |
|
Mono Therapy |
97 |
46.9% |
|
Bi Therapy |
72 |
34.8% |
|
Triple Therapy |
32 |
15.5% |
|
Quadruple Therapy |
6 |
2.9% |
|
Total |
207 |
|
|
|
|
|
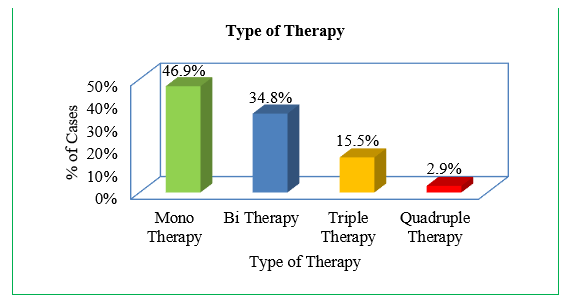
Fig 4. Graphical presentation of type of therapy received
Table 5: Distribution of patients based on culture sensitivity test performed
|
Culture Sensitivity |
No. of Subjects |
Percentage |
|
None |
193 |
93.2% |
|
E.coli |
3 |
1.4% |
|
Mantoux test |
5 |
2.4% |
|
Sputum test |
2 |
1.0% |
|
Pseudomonas |
1 |
0.5% |
|
Smear for MP |
1 |
0.5% |
|
Culture APB |
1 |
0.5% |
|
Gram positive bacilli and cocci |
1 |
0.5% |
|
Total |
207 |
|
|
|
|
|
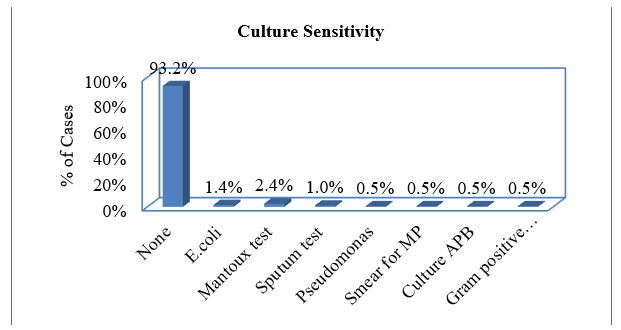
Fig 5: Graphical presentation of culture sensitivity test performed
Prescribing Pattern
Table 6: Distribution of patients based on antibiotics prescribing pattern
|
Type of Antibiotic Used |
No. of Subjects |
Percentage |
|
Only Generic |
27 |
13.0% |
|
Only Brand |
118 |
57.0% |
|
Combination |
62 |
30.0% |
|
Total |
207 |
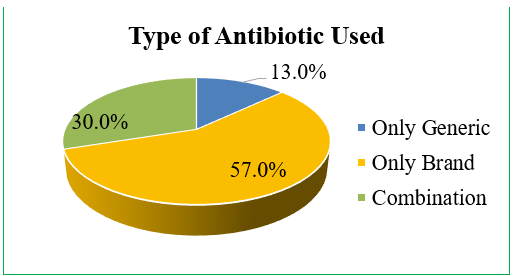
Fig 6. Graphical presentation of antibiotics prescribing patterns
Table 7: Distribution of patients based on antibiotics route of administration
|
Route of Administration |
No. of Subjects |
Percentage |
|
Only IV |
145 |
70.0% |
|
Only Oral |
24 |
11.6% |
|
IV + Oral |
38 |
18.4% |
|
Total |
207 |
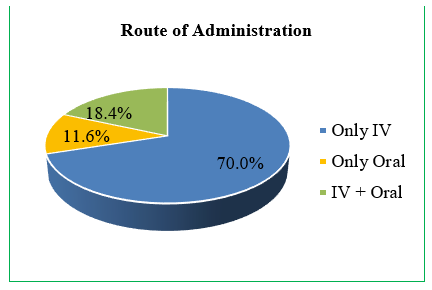
Fig 7: Graphical presentation of antibiotics route of administration
Table 8: Distribution of patients based on antibiotics duration of therapy
|
Duration of Antibiotic Therapy (Days) |
No. of Subjects |
Percentage |
|
<= 15 |
187 |
90.3% |
|
16 - 30 |
18 |
8.7% |
|
31 & Above |
2 |
1.0% |
|
Total |
207 |
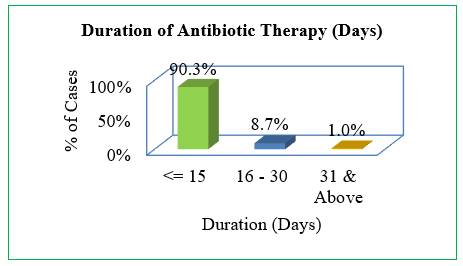
Fig 8: Graphical presentation of antibiotics duration of therapy
Table 9: Distribution of prescribed antibiotics
|
Antibiotic |
No. of antibotics |
|
Ceftriaxone |
124 |
|
Metronidazole |
58 |
|
Amikacin |
38 |
|
Amoxicillin Clavulanate |
37 |
|
Magnex forte |
15 |
|
Cefotaxime |
17 |
|
Azithromycin |
16 |
|
Doxycycline |
8 |
|
Piptaz(piperacillin+tazobactum) |
7 |
|
Ciprofloxacin |
12 |
|
Clindamycin |
5 |
|
Meropenem |
5 |
|
Cefixime |
4 |
|
Gentamycin |
2 |
|
Ofloxacin |
2 |
|
Penicillin |
2 |
|
Ampicillin |
1 |
|
Cefpodoxime |
1 |
|
Levofloxacin |
1 |
|
Midazolam |
1 |
|
Niftas(nitrofurantoin) |
1 |
|
Rifaximin |
1 |
|
Cefbact T(ceftriaxone+tazobactum) |
1 |
DISCUSSION
According to our study, most patients were males (60.9%) and females were (39.9%) which is found to be greater compared to the study conducted by S. Anandhkumar et al (2019) (male 54.63%, female 45.36%).[12] According to our inclusion criteria, majority of patients receiving antibiotics were seen in the general surgery department (44%) which was found to be greater than the study conducted by Ogbonna B.O et al (2022) (18.3%).[13] Many of the patients, that is, 97 patients (46.9%) out of 207, were prescribed one antibiotic which was found to be lesser than the study conducted by Sesham, Pushpalatha et al (2020) (59%).[14] For a total of 207 patients receiving antibiotics, a culture sensitivity test or microbial culture test was performed only in 14 patients. 93.2% of patients were prescribed antibiotics without performing any prior culture test which was found to be more than the study conducted by the S. Anandhkumar et al (2019) (50.73%).[15] 57.0% (118) of patients were prescribed antibiotics in brand names only. 13.0% (27) patients were prescribed antibiotics in generic names only which was found to be greater than the study conducted by Sesham, Pushpalatha et al (2020) (9.85%).[16] Many patients were prescribed with the intravenous route (70%) which was found to be less than the study conducted by Sesham Pushpalatha et al (2020) (92.5%).[17] The most prescribed antibiotic observed in our study was Monocef, with the generic name Ceftriaxone, in about 124 patients.
CONCLUSION
Evaluation of antibiotic usage in hospital setting is essential to know the prescribing pattern of antibiotics. One reason to be aware of the antibiotic treatment pattern towards patients is the rise in antibiotic resistance. Antibiotic prescription practices did not adhere to standards. Irrational antibiotic prescription is prevalent because most antibiotics are provided without first doing a culture test to isolate bacteria. The fact that most patients who were given antibiotics for infectious or disease-related illnesses were able to recover shows that the medicine was successful. Over the course of our research, Monocef (ceftriaxone) was given more often than any other antibiotic. Metronidazole, amikacin, (amoxicillin + clavulanate), (cefoperazone + Sulbactam), cefotaxime, and azithromycin were the next most frequent. It would be better for hospitals to prescribe generic antibiotics instead than brand-name ones. Prior to administering antibiotics, medical providers should be prompted to do microbial culture testing and laboratory tests. The current study presents the following World Health Organization (WHO) indicators: an average of 1.73 antibiotics per prescription, 70% injection encounters, 100% essential drug list drugs, and 46.9% patients prescribed at least one antibiotic.
REFERENCES

Gattipalli Vaishale, Huma Fareha, Rendla Rakesh, Jadur Shruthi, Dr. Priyanka Anil*, A Study on Antibiotics Usage Trends: Insights from Drug Utilization Evaluation, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 3060-3073 https://doi.org/10.5281/zenodo.17004019
 10.5281/zenodo.17004019
10.5281/zenodo.17004019
