Department of Pharmacology, Dadasaheb Balpande college of Pharmacy.
Non-alcoholic fatty liver disease (NAFLD) is a leading cause of chronic liver disease worldwide, affecting a significant proportion of the population due to the rising prevalence of obesity and metabolic syndrome. NAFLD encompasses a spectrum of conditions, ranging from simple hepatic steatosis to non-alcoholic steatohepatitis (NASH), which can lead to fibrosis, cirrhosis, and hepatocellular carcinoma. The disease is closely linked to insulin resistance, dyslipidemia, and type 2 diabetes, making it a critical component of metabolic dysfunction. The pathogenesis of NAFLD involves complex interactions between genetic predisposition, dietary habits, lipid metabolism abnormalities, oxidative stress, and gut microbiota dysbiosis. While non-invasive diagnostic tools such as imaging modalities and serum biomarkers have improved early detection, challenges remain in accurately assessing disease severity and progression. Currently, lifestyle modifications, including weight loss, exercise, and dietary interventions, are the cornerstone of treatment. However, novel therapeutic targets focusing on metabolic regulation, inflammation control, and fibrosis inhibition are under investigation to provide effective pharmacological options. Given the significant impact of NAFLD on liver-related and cardiovascular morbidity, early detection and comprehensive management strategies are essential. Future research should prioritize personalized medicine approaches, improved biomarkers, and targeted therapies to prevent disease progression and reduce the global burden of NAFLD.
The condition termed NAFLD is characterized by fat accumulation liver. It affects people who consume no or less alcohol. This condition is characterized by inflammation and excessive fat accumulation. It is significantly correlated with obesity and metabolic disorder. People at risk for NAFLD may develop cirrhosis, liver carcinoma, and heart problems. The incidence of NAFLD is shown to be between 20% and 30%, with a higher prevalence in elderly populations, and there are approximately 2 new cases per 100 patients each year. (1) . Macro vesicular steatosis presence in ≥5% of hepatocytes in individuals that consume less/no alcohol described as NAFLD. Classification of NAFLD (non-alcoholic fatty liver), which also called as simple steatosis, NON-ALCOHOLIC STEATOHEPATITIS is an advance form of NAFLD which can further develop into cirrhosis of the liver, hepatocellular carcinoma (2). Individuals with NAFLD often experience obesity or diabetes, with insulin resistance contributing as significant pathogenic factor. There are four distinct phenotypes identified among patients with NAFLD,
Microbiota, environmental factor and genetic factors. Factors like microbiome and genetic factor have important role in progression of NAFLD. NAFLD encompasses a spectrum of liver diseases characterized by various degrees of injury and fibrosis. Out of these, non-alcoholic steatohepatitis (NASH) represents a more severe form associated with an inflammatory state as well as injury to liver cells (steatohepatitis); it is usually associated with peri-cellular fibrosis, which may lead to cirrhosis. NAFL is hepatic steatosis, or fat of the liver. NAFLD generally occurs in patients with obesity and obesity-related conditions (e.g., type 2 diabetes)
Causes For NAFLD
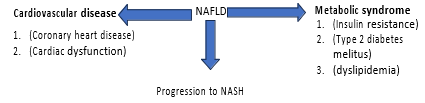
Fig.1 interrelation between NAFLD cardiovascular disease and metabolic syndrome.
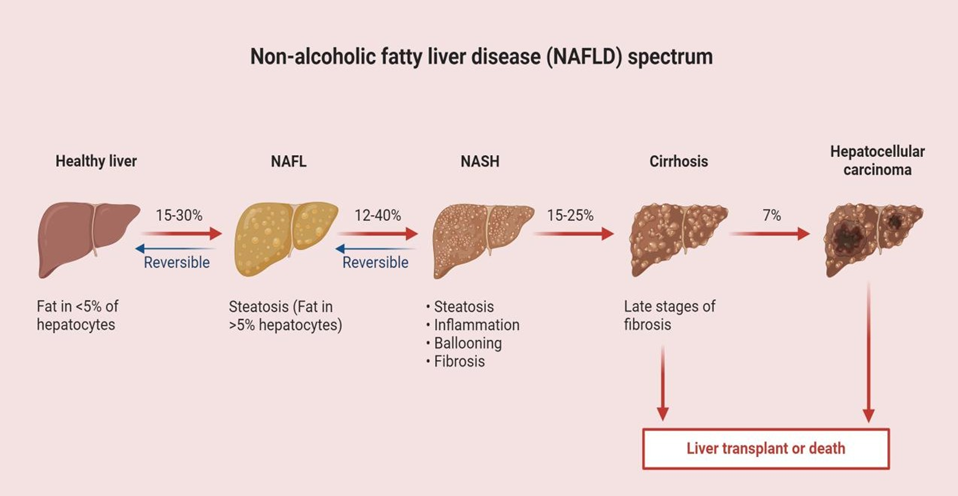
Fig.2 Spectrum of Non-alcoholic fatty liver disease
Factor Influencing NAFLD / Risk Factor Of NAFLD
Genetic factor
NAFLD is strongly related to genomic factors & Research into the genetics of NAFLD has encompassed heritability studies, candidate gene investigations, familial accumulation analyses and genome-wide association studies.
PNPLA3 (Patatin-Like Phospholipase Domain Containing Protein 3):
The PNPLA 3 protein is a that cause breakdown of retinyl ester and triglycerides .isoleucine to methionine change at amino acid position 148 is due to rs738409 C>G genetic variant which further result in reduce release of retinyl ester and decrease of hydrolase activity . All these alteration leads to buildup of fat in hepatic cells which also include stellate cells ultimately leads to hepatic inflammation.
TM6SF2 (Transmembrane 6 Superfamily Member 2):
A TM6SF2 has a significant role in synthesis of triglyceride rich protein mediated by VLDL and is situated in endoplasmic reticulum and Golgi apparatus. The C to T change at nucleotide 499 result in glutamate to lysine substitution at codon 167 (E167K) is caused by rs58542926 variant. This variant causes a decrease in TM6SF2 that cause buildup of lipid in liver
MBOAT7 (Membrane-Bound O-Acyltransferase Domain Containing 7):
Hepatic stellate cell, hepatic sinusoidal cell and hepatic cells are responsible to initiate expression of MBOAT7. Research indicates that the T allele of rs641738 in MBOAT7 (chr19:54173068) is linked to a heightened risk of developing the full range of NAFLD.(7) Alterations in the expression levels or polymorphisms of these three genes/proteins have been identified as contributing factors to the development of NAFLD
Metabolic Syndrome
Polycystic ovary syndrome (PCOS)
NAFLD is strongly associated with Polycystic ovary syndrome (PCOS)PCOS is characterized by insulin resistance and alteration in hormonal level mainly estrogen and progesterone and increase in androgen level with irregular ovulation and is linked to CVS disorders type 2 DM and obesity. It is a common endocrine disorder which affects premenopausal women, with occurrence rate ranging from 5% to 18%, depending on the criteria used for diagnosis. In addition to its reproductive implications, It is observed that women with PCOS show higher incidence of nafld particularly with high androgen level, insulin resistance and obesity. . (8)
Dyslipidemia:
Dyslipidaemia refers to abnormal level of lipids in blood circulation. This condition is characterized by an increase in levels of lipids in body which mainly includes low-density lipoprotein (LDL) cholesterol, with decreased levels of high-density lipoprotein (HDL) cholesterol and triglycerides. It has been noted that this increased level of triglyceride, LDL,and reduced level of HDL are major cause for manifestation of CVD. Athersclerosis is a disease in which fat,cholesterol,get deposited in artery wall is observed in patients with NAFLD. this condition increases the occurrence of atherosclerosis. Chronic dyslipidaemia can cause an increase in SREBP 1 that affects production of lipids in liver which leads to increase in LDL and triglyceride. All these factor described above can cause damage to hepatocytes and further cause its necrosis. (9)
Factor Influencing NAFLD / Risk Factor of NAFLD
Genetic factor
NAFLD is strongly related to genomic factors & Research into the genetics of NAFLD has encompassed heritability studies, candidate gene investigations, familial accumulation analyses and genome-wide association studies.
PNPLA3 (Patatin-Like Phospholipase Domain Containing Protein 3):
The PNPLA 3 protein is a that cause breakdown of retinyl ester and triglycerides .isoleucine to methionine change at amino acid position 148 is due to rs738409 C>G genetic variant which further result in reduce release of retinyl ester and decrease of hydrolase activity . All these alteration leads to buildup of fat in hepatic cells which also include stellate cells ultimately leads to hepatic inflammation.
TM6SF2 (Transmembrane 6 Superfamily Member 2):
A TM6SF2 has a significant role in synthesis of triglyceride rich protein mediated by VLDL and is situated in endoplasmic reticulum and Golgi apparatus. The C to T change at nucleotide 499 result in glutamate to lysine substitution at codon 167 (E167K) is caused by rs58542926 variant. This variant causes a decrease in TM6SF2 that cause buildup of lipid in liver
MBOAT7 (Membrane-Bound O-Acyltransferase Domain Containing 7):
Hepatic stellate cell, hepatic sinusoidal cell and hepatic cells are responsible to initiate expression of MBOAT7. Research indicates that the T allele of rs641738 in MBOAT7 (chr19:54173068) is linked to a heightened risk of developing the full range of NAFLD.(7) Alterations in the expression levels or polymorphisms of these three genes/proteins have been identified as contributing factors to the development of NAFLD
Metabolic Syndrome
Polycystic ovary syndrome (PCOS)
NAFLD is strongly associated with Polycystic ovary syndrome (PCOS)PCOS is characterized by insulin resistance and alteration in hormonal level mainly estrogen and progesterone and increase in androgen level with irregular ovulation and is linked to CVS disorders type 2 DM and obesity. It is a common endocrine disorder which affects premenopausal women, with occurrence rate ranging from 5% to 18%, depending on the criteria used for diagnosis. In addition to its reproductive implications, It is observed that women with PCOS show higher incidence of nafld particularly with high androgen level, insulin resistance and obesity. . (8)
Dyslipidemia:
Dyslipidaemia refers to abnormal level of lipids in blood circulation. This condition is characterized by an increase in levels of lipids in body which mainly includes low-density lipoprotein (LDL) cholesterol, with decreased levels of high-density lipoprotein (HDL) cholesterol and triglycerides. It has been noted that this increased level of triglyceride, LDL,and reduced level of HDL are major cause for manifestation of CVD. Athersclerosis is a disease in which fat,cholesterol,get deposited in artery wall is observed in patients with NAFLD. this condition increases the occurrence of atherosclerosis. Chronic dyslipidaemia can cause an increase in SREBP 1 that affects production of lipids in liver which leads to increase in LDL and triglyceride. All these factor described above can cause damage to hepatocytes and further cause its necrosis.(9)
Type 2 Diabetes Melitus And Insulin Resistance
TYPE 2 DM is a metabolic disorder which is charecterized by increased level of blood glucose and decreased secretion of insulin and involves destruction of b cell of langerghans of pancreas. TYPE 2 DM leads to various complication such as CVD like stroke atherosclerosis angina and also give rise to insulin resistance and pcos which ultiimately increases the prevalence of nafld in individual. currently in many meta analysis observational studies it has been proved that nafld is dierctly associated and increases the risk of devoloping TYPE 2 DM regardless of obesity and other metabolic risk factors. In many large hospital studies like valpolicella heart diabetes study it was found that patient with TYPE 2DM shows increased prevalance of nafld ranging from 45 to 75 percentage . It is also being suggested that people with TYPE 2 DM are at elevated risk of devoloping nash which is a more severe form of nafld.
It has been suggested that the mechaniism by which TYPE 2 DM cause or induces nafld is said to be insulin resistance and hepatic lipid accumulation which further cause inflammation of liver In many meta analysis studies performed in sri lanka china japan taiwan sweden and spain which included atleast 5001022participants of average age ranging 47 years it is found that people exhibiyting TYPE 2 DM SHOWS an 2-4 folds increased risk for devoloping nafld . Over 28000 new cases of TYPE 2 DM are identified every 5 years associated with nafld.
Cardiovascular Disease
Many studies provides proof that NAFLD is directly linked to cardiovascular disease.The mechanism for their interelation is suggested that triglyceride rich lipoprotein that contain apolipoprotein C3 are of greater importance .Toll like receptors 2 and 4 are activated by lipoprotein by dimerization that leads to stimulation of NOD like receptor family , pyrin domain containing protein 3(NLRP3) inflammasome .This follows mainly two pattern which are damage associated molecular pattern (DAMPs) and pathogen associated molecular pattern (PAMPs) or atherosclerosis linked stimuli for activation of NLRP3 .The interleukin
1β t CONVERTING ENZYME also known as capase 1 activity is regulated by NLRP3 inflammaosome.
The activation of caspase-1 through the NLRP3 inflammasome results in the proteolytic activation of proinflammatory cytokines from the IL-1β family, leading to the activation of the inflammatory cascade from IL-1 to IL-6 to C-reactive protein (CRP). This pathway plays a crucial role in the onset of vascular inflammation and the progression of atherosclerotic cardiovascular disease.. (10)All evidence described above suggest that individuals suffering from NAFLD may devolop disease like hypertension ,cardiac arrythmia , cardiac artery disease (10) .
NAFLD and arterial hypertension:
Arterial hypertension is defined as the force excerted by blood on arterial wall. In individual with NAFLD the prevalance rate for developing hyperytension is high. according to estimate the stastical data provided by WHO the arterial hypertension is considerd as an risk factor for the cardiovascular disease. the current data from WHO shows that 54% of all strokes and 47% of ischemic heart disese contributes to hypertension. the incidence of arterial hypertension is in-between 40% to 70% in NAFLD patients. the research shows that strong link between NAFLD and inrcease chances for developing prehypertension & hypertension(10).
NAFLD and cardiac arrhythmias:
Emerging research indicates that non-alcoholic fatty liver disease (NAFLD) is linked to a heightened risk of cardiac arrhythmias, including atrial fibrillation and ventricular arrhythmias. NAFLD is marked by chronic low-grade inflammation and an elevated production of pro-inflammatory substances, including cytokines that may originate from the systemic circulation or be produced locally in the pericardial adipose tissue. This condition can influence the myocardium by altering specific ion channels, which leads to an extended action potential duration, consequently increasing the QTc interval. Furthermore, insulin resistance, a fundamental aspect of metabolic syndrome, may result in lower potassium levels, which can contribute to the prolongation of ventricular repolarization
Gut Microbiota
A (unhealthy gut microbiota) Gut dysbiosis associates with the pathogenesis of obesity- related disorders that involve metabolic syndrome and nonalcoholic fatty liver disease (NAFLD). A dysbiotic gut can increase the liver's exposure to bacteria, bacterial products, and harmful dietary ingredients that contribute to NAFLD pathophysiology. Study conducted on adults with NAFLD revealed a highly significant association between steato-hepatitis lower proportion of Bacteroidetes, and a higher proportion of C. coccoides (phylum Firmicutes). (11) Many research shows that non dietary ethanol may be the causative factor in growth of nonalcoholic steaohepatitis(NASH). Dysbiosis could lead to increased intestinal ethanol production, for instance, in anaerobic conditions under 1g of E. coli producing 0.8g of ethanol per hour. Furthermore, substantially increasing patients with NASH was found in Proteobacteria ( mainly E. coli and other Enterobacteriaceae), which produce alcohol.
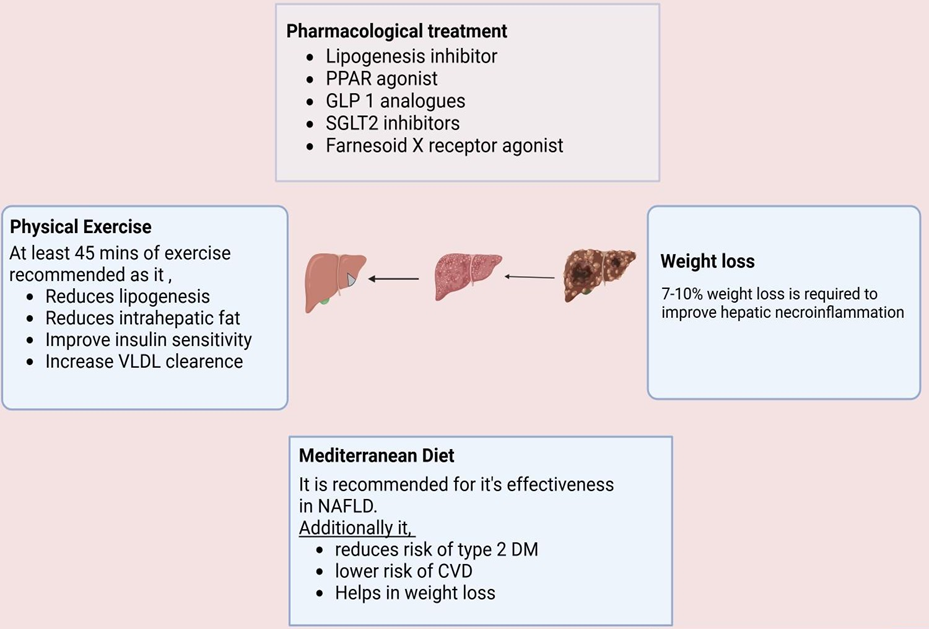
Fig 3: Current Treatment Approaches for NAFLD
Current Treatment Options
(1) Natural compounds Honokiol
Honokiol (HNK) is recognized as an anti-fibrotic agent that influences autophagy. Natural compounds and their derivatives are also considered promising candidates for the development of new medications for non-alcoholic fatty liver disease (NAFLD). HNK, a bioactive substance derived from the Magnolia grandiflora plant, has been widely utilized in herbal medicine. Research has demonstrated that HNK can reduce liver fibrosis in rat models, although the specific mechanisms behind its action have not been thoroughly investigated in mouse models. In studies focused on renal fibrosis, HNK was found to inhibit the TGF-1/SMAD signaling pathway in hepatic stellate cells (HSCs), suggesting a key role in its antifibrotic properties.(14)
Quercetin
Natural polyphenols are a diverse group of polyphenolic compounds that are used to treat metabolic disorders and have been shown to have hepatoprotective properties [15]. The main causes of this protective effect are decreased fibrotic lipolysis and increased lipid breakdown in the liver, which reduce oxidative stress and subsequent hepatocellular damage. Naturally occurring polyphenolic flavonoid, quercetin (QUE) has antioxidant, anti-inflammatory, immunoprotective and anti-apoptotic properties. Although its hepatoprotective role has already been proven by a number of research, the pathophysiological processes behind its impact on NAFLD remain unclear. Process of autophagy plays a crucial role in maintaining liver homeostasis, and is important to inhibit intracellular degeneration. It promotion has hepatoprotective role as well as it regulates intracellular lipid stores and hepatocellular lipid metabolism. Many studies have shown that in established of NAFLD is inhibited by hepatic autophagy.
Curcumin
Turmeric is dried as well as fresh rhizome obtained from the plant Curcuma longa, which belongs to family Zingiberaceae. the active ingredients are curcumin, demethoxycurcumin, bisdemethoxycurcumin, and curlone. Among these curcumin has a more potent effect. Various research has proven that turmeric exhibits potent antioxidant, anti-inflammatory, antifibrotic effect and also improves insulin sensitivity. due to all of this activity turmeric has a potent role in NAFLD.
Resveratrol
Reservetrol is a stillbenoid derivative and a polyphenolic compound which occurs naturally It has anti-inflammatory as well as anti oxidant properties .The mechanism of action includes stimulation of AMP activated protein kinase (AMPK) and Silent information regulation homologue 1 (SIRT)(16)
Silymarin
Silymarin is a herbal plant which is currently used for the treatment of liver and gallbladder disorder .Silymarin is known to posses antinflammatory , immunomudulatory antioxidant and liver regernating effects . The biological source of silymarin is Silynum marianum L.and belongs to family asteraceae and the chief chemical constituents includes silybinin, isosilybinin A and B, silychristin. Silymarin is shown to have liverprotective, liver cleansing and reducing inflammation in individuals suffering from nafld. It has also been noted that it modulates the level of ALT AST triglyceride and also decreases the expression of IL 6 ,caspase 3 ,MAPK1 and enhance expression of AKT1 . .(17)
Oleanolic acid
Oleanolic acid is a pentacyclic triterpenoid found in numerous plant species and is used clinically in China for its liver-protective properties. Research indicates that this compound can reduce triglyceride buildup in rats subjected to fructose. The effects of oleanolic acid are linked to the suppression of mRNA levels of SREBP-1c, along with a decrease in its nuclear protein expression, which plays a crucial role in the synthesis of new lipids.(18)
Limitations :
Liver Toxicity: Although OA is recognized for its protective benefits on the liver, excessive dosages and prolonged usage may result in liver damage (19).
Gastrointestinal Issues: Frequent side effects noted in clinical studies of OA derivatives, including bardoxolone methyl, are fatigue, nausea, and loss of appetite. (19)
(2) Pharmacological drug
Aramchol (arachidyl amido cholanoic acid) symbolizes a novel synthetic compound. It is the product of the conjugation of two substances: arachidic acid (saturated fatty acid) and cholic acid (bile acid). It reduces the storage of fat in the liver by increasing fat oxidation.According to numerous studies, Aramchol improved insulin resistance, decreased the atherogenic effect, and dramatically decreased the liver's fat content in animals fed a high-fat diet. Numerous human investigations have examined its effectiveness and safety in reducing liver fat since its effect on animals was discovered. In a clinical study of individuals with non-alcoholic fatty liver disease (NAFLD), a particular dosage of Aramchol (300 mg) for three months decreased the liver's fat content by over 12.5% when compared to a placebo, with no significant adverse medication reactions. (22)
Obeticholic acid (OCA)
Agonist of FXR oca proves to be a beneficial option for the treatment of NAFLD. It belongs to semi synthetic derivative of chenodeoxycholic acid. It causes activation of FXR and also additionally regulates the secretion of FGF 19 that have significant role in bile synthesis in liver. In primary biliary cholangitis patient this medication is used as a treatment option. .(23)
Limitation:
•The Food and Drug Administration issued a new warning restricting the use of OCA in patients with advanced cirrhosis (24)
Pioglitazone
Pioglitazone belongs to a class of thiazolidinediones that works by enhancing insulin sensitivity. Pioglitazone's main mechanism involves activation of PPARy, which further enhances glucose uptake by cells. Studies have shown that it causes positive changes in the ALT and AST levels of rats. THEREFORE it can also be employed in treatment of NAFLD.(25)
Limitation:
Peripheral oedema: Rise renal sodium re-absorption
Peripheral vasodilation: Rise VEGF production, Congestive heart failure.
Reduced aromatase activity with altered oestrogen production and Rise bone resorption.
Weight gain: Rise adipogenesis, Rise lipogenesis(mainly in subcutaneous fat.(25) Elafibranor acts as an agonist of PPAR-α and PPAR-δ and is currently under development for the treatment of NAFLD (27)
Semaglutide
Semaglutide is classified as a glucagon-like peptide-1 receptor agonist (GLP-1 RA) that, upon binding to its receptor, triggers various intracellular signaling pathways with diverse effects. (28). Additionally, it curbs energy consumption by modulating appetite and slows down gastric emptying, leading to weight reduction. Furthermore, semaglutide exhibits antioxidative properties and mitigates mitochondrial damage, a factor that is believed to be crucial in the development and advancement of NAFLD.(29)
Limitation:
It is a novel liver targeted inhibitor of acetyl CoA carboxylase Rationale for ACC inhibition as treatment for NAFLD Reason for using ACC inhibition to treat NAFLD. Although ACC1/ACC2 plays a key role in stimulating DNL and impairing fatty acid β-oxidation, pharmacologically inhibiting ACC enzymes offers an attractive treatment option for NAFLD/NASH by reducing hepatic lipid synthesis and enhancing fatty acid oxidation concurrently.(32)
Limitation:
An imbalance between the biological system's capacity for rapid detoxify reactive intermediates and the systemic manifestation of reactive oxygen species is reflected in oxidative stress. Vitamin E (Vit. E), also known as alpha tocopherol, is one of the essential vitamins and micronutrients. Hydroxyl group in the thetocochromanol ring that donates or releases the hydrogen ion to neutralise free radicals and reactive oxygen species is the main reason for the antioxidant property of Vit E. It fat-soluble vitamin and consists of four isoforms α-, β-, δ , and γ, which possess their unique properties. Cell proliferation, cellular signaling, and the modulation of inflammatory response genes are all impacted by these isoforms. 2 2 2 Through modifying the activity of several enzymes involved in signal transduction, including protein kinas (PKC), cyclooxygenase-2 (COX 2), 5 lipooxygenase, protein phosphate, monocyte chemoattractant protein-1, and various factors in the mitogen- activated protein (MAPK) signal transduction pathway, Vit. E acts both directly and indirectly.
Vitamin E in NAFLD
in several experimental models of NAFLD. Vitamin E has been evaluated. α-tocopherol supplementation attenuated LPS-induced liver damage and prevented oxidative stress, including steatosis and necroinflammation, and inflammation-related diseases in mice with NASH induced by a methionine-choline-deficient (MCD) diet. (31). Additionally, vitamin E reduced ROS-induced TGF-β production, that has been associated to development of liver fibrosis.(36)
Structure of Vitamin E
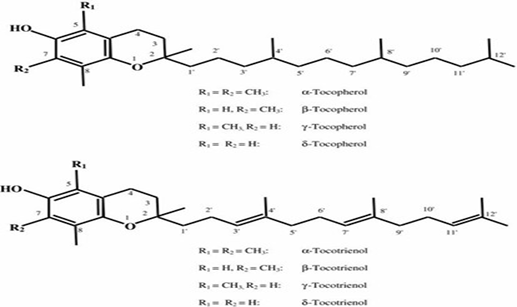
Fig. Structure of vitamin E
Major Proteins Involved in Non- Alcoholic Fatty Liver Disease:
Sterol Regulatory Element-Binding Protein (SREBPs) Sterol Regulatory Element-Binding Protein (SREBPs)
Sterol regulatory element-binding proteins (SREBPs) are membrane-bound transcription factors that control the expression of genes involved in lipid synthesis. SREBP-1c boosts the expression of genes that encode lipogenic enzymes, including ACC and FAS. Insulin is a well-known stimulator of lipogenesis. It activates the liver's expression of SREBP-1c. Insulin receptor substrate (IRS) proteins are a group of docking molecules that link insulin receptor activation to important downstream pathways. The two main isoforms, IRS-1 and IRS-2, are found in high amounts in the liver. Besides positively regulating SREBP-1c expression, IRS proteins also reduce fatty acid oxidation by inhibiting a transcription factor called forkhead box protein A2 (Foxa2).
ROLE OF SREBP-1C IN NAFLD
AMP-activated protein kinase (AMPK) acts as an energy sensor. It regulates cellular metabolism, including lipid metabolism. AMPK activates when cellular AMP levels rise, signaling changes in energy stores. When it is active, AMPK promotes ATP-producing pathways like fatty acid oxidation while inhibiting ATP-consuming processes such as lipogenesis. This means AMPK activation lowers the expression of ACC and FAS by down-regulating SREBP-1c. We have not fully studied the mechanisms involved in the development of NAFLD, especially in humans. Additionally, we know little about how fatty acid synthesis is regulated in NAFLD. In this study, we looked at the expression of lipogenesis regulator genes.
Niemann-Pick C1-Like 1 (NPC1L1)
Niemann-Pick C1-Like 1 (NPC1L1) is a multi-spanning transmembrane protein found in the apical membrane of enterocytes and the canalicular membrane of hepatocytes. It acts as a sterol transporter to assist in intestinal cholesterol absorption and balances out cholesterol excretion from the liver and bile. NPC1L1 is the main target of ezetimibe, a strong cholesterol absorption inhibitor commonly used to treat high cholesterol. Recent research shows that a lack of NPC1L1 or treatment with ezetimibe can also prevent diet-induced liver fat accumulation and obesity in addition to lowering blood cholesterol. Future studies should examine the molecular mechanisms behind NPC1L1-dependent cholesterol transport and clarify how this cholesterol transporter affects the development of metabolic diseases. dependent cholesterol transport and clarify how this cholesterol transporter affects the development of metabolic diseases.
Hydroxysteroid 17-Beta Dehydrogenase 13
Hydroxysteroid 17-beta dehydrogenase 13 (HSD17B13) is an enzyme that plays a role in the metabolism of steroids, particularly in the conversion of androstenedione to testosterone and estrone to estradiol. It is primarily found in the liver, but it is also expressed in other tissues, including the brain and reproductive organs. HSD17B13 has gained attention due to its potential involvement in liver diseases, especially non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD). Genetic studies have identified variants of the HSD17B13 gene that may influence an individual's risk of liver damage. Some variants are associated with a reduced risk of liver disease, while others may predispose individuals to liver injury. Research is ongoing to understand the full implications of HSD17B13 in liver health and to explore its potential as a therapeutic target for treating liver diseases.
Serine/Threonine Kinase Stk25
Serine/threonine kinase STK25(also known as Serine/threonine-protein kinase 25) is an enzyme that is involved in various cellular processes, including regulating cell growth, metabolism, and signalling pathways. It is a member of the larger family of serine/threonine kinases, which play important roles in phosphorylation, a process that can activate or deactivate many proteins involved in cellular functions.
1. Metabolic Regulation: STK25 is involved in regulating metabolic processes, particularly those related to glucose and lipid metabolism. It plays a role in energy homeostasis and has been studied in the context of obesity and insulin resistance.
2. Mitochondrial Function: STK25 has been implicated in regulating mitochondrial dynamics and function, which is critical for cellular energy production. Disruptions in STK25 activity could potentially lead to mitochondrial dysfunction, contributing to metabolic diseases.
3. Inflammation and Disease: Studies have also suggested that STK25 may be involved in inflammatory processes, particularly in the context of obesity- related diseases such as non-alcoholic fatty liver disease (NAFLD) and type 2 diabetes.
4. Signalling Pathways: STK25 participates in various signaling pathways, influencing processes like cell survival, proliferation, and stress response. It can impact insulin signaling and various pathways that regulate cell metabolism and growth.
STK25 and Disease Associations:
Obesity and Metabolic Disorders: Variations in the STK25 gene have been linked to obesity and insulin resistance, which are central to conditions like type 2 diabetes and metabolic syndrome.
Liver Disease: There is growing evidence that STK25 may play a role in liver health, particularly in the development of fatty liver disease and other liver- related metabolic conditions.
Vitamin E Docking Result
Table1: vitamin E docking with NPC1L1, SREBP, Hydroxysteroid 17-beta-dehydrogenase 13, Serine-Threonine kinase STK 25
|
Name of protein |
Ligand (PDB ID) |
Binding Affinity |
|
NPC1L1 |
3QNT |
-5.1 |
|
SREBP |
1AM9 |
-6.5 |
|
Hydroxysteroid 17-beta- dehydrogenase 13 |
8G89 |
-7.7 |
|
Serine-Threonine kinase STK 25 |
7Z4V |
-7.7 |
Firsocostat docking result
Table2: firsocostat docking with NPC1L1, SREBP, Hydroxysteroid 17-beta-dehydrogenase 13, Serine-Threonine kinase STK 25
|
Name |
Ligand (PDB ID) |
Binding affinity |
|
NPC1L1 |
3QNT |
-6.5 |
|
SREBP |
1AM9 |
-6.5 |
|
Hydroxysteroid 17-beta- dehydrogenase 13 |
8G89 |
-8.8 |
|
Serine-Threonine kinase STK 25 |
7Z4V |
-8.7 |
Structure Of Interaction of Different Protein with Vitamin E
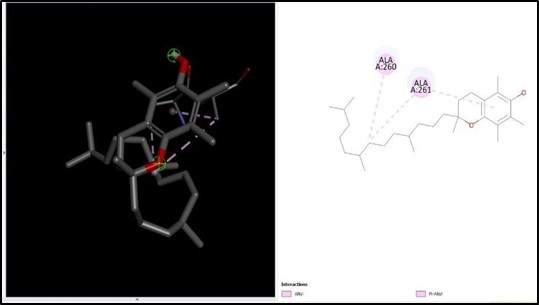
Fig. 2D, 3D Structure of 3QNT
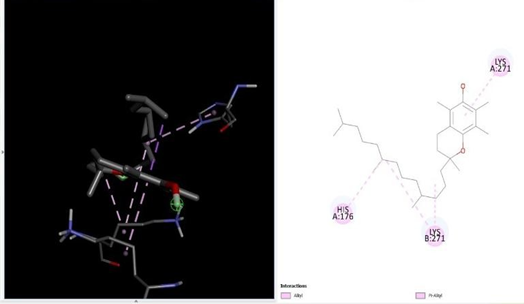
Fig. 3D,2D Structure of 8G89

Fig. 3D,2D Structure of 7z4v
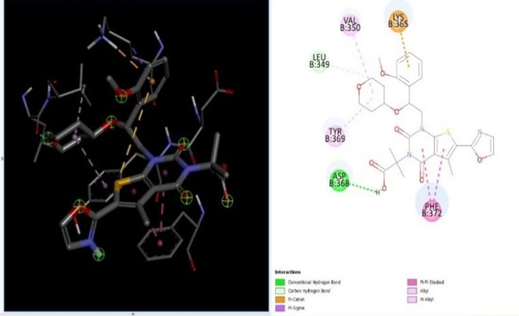
Fig. 3D,2D Structure of 1AM9
Structure Of Different Protein with Firsocostat
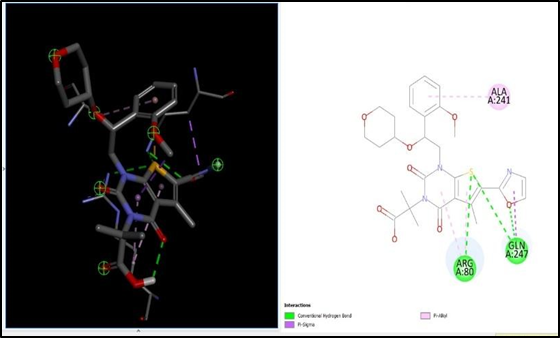
Fig. 2D, 3D Structure of 3QNT
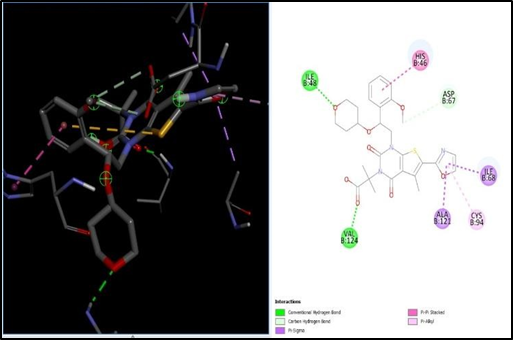
Fig. 3D,2D Structure of 8G89
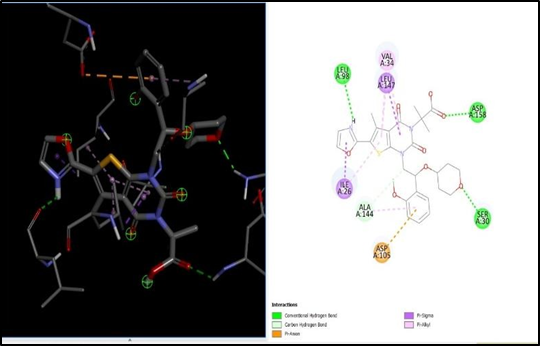
Fig. 3D,2D Structure of 7z4v
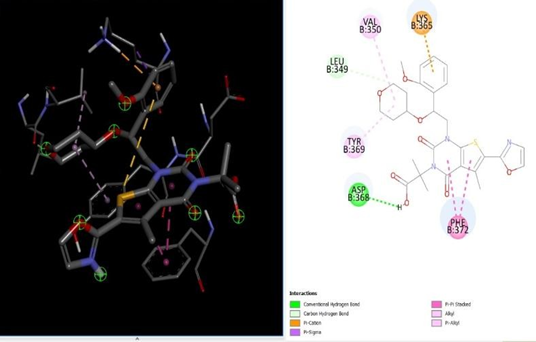
Fig. 3D,2D Structure of 1AM9
REFERENCE


Yash Bhoyar*, Vrushab Awachat, Disha Kemekar, Anuja Jikar, Sachin More, Identifying and Validating Target for NAFLD Through in Silico Study, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 580-598 https://doi.org/10.5281/zenodo.17283401
 10.5281/zenodo.17283401
10.5281/zenodo.17283401
