Department of Pharmacy Practice, School of Pharmaceutical Sciences, Vels Institute of Science, Technology and Advanced Studies (VISTAS), Chennai-600117, Tamilnadu, India
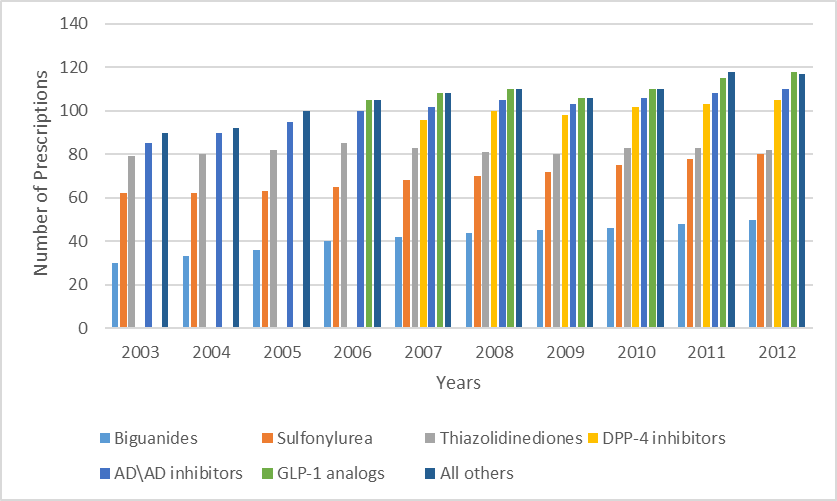
Over 0.4 billion individuals worldwide are affected from diabetes mellitus (DM), which could lead to serious side effects like heart disease, stroke, kidney damage, blindness, and nerve damage. High blood sugar content, which are generated by inappropriate insulin activity, are a hallmark of diabetes mellitus. Type 2 diabetes is brought on by impairment to the pancreatic Beta cells, whereas type 1 diabetes is an autoimmune condition. Serious consequences can arise from tiny blood vessel damage caused by elevated blood glucose levels. Elevated plasma glucose levels or HbA1c testing are used to identify diabetes. For diagnosis, the WHO suggests a HbA1c cutoff of 48 mmol/mol (6.5%). This study’s goal is to gain access type II diabetes patients' prescription use habits by utilising WHO's primary drug prescribing indicators to In order to encourage appropriate medication use and give medical practitioners useful information, the study under discussion attempts to assess the drug consumption habits of individuals with type II diabetes using WHO's core drug prescribing indicators. This study current bias in the use of antidiabetic medications in US retail pharmacies from 2003 to 2012. With 18.8 million users by 2012, it reported a 42.9% increase in patients filing prescriptions for antidiabetic drugs, which closely matched CDC projections for cases of confirmed diabetes. With 62.7% of patients using it, metformin was the most recommended medication. Newer drugs like Dipeptidyl peptidase-4 inhibitors and Glucagon-like peptide-1 receptor agonist became more popular, sulfonylureas were used less frequently. Many patients used these more recent medications without taking metformin, despite advice to the contrary. The study emphasises how important it is to comprehend medication usage trends in order to improve diabetes treatment and adherence.
Over 0.4 billion people worldwide affected from diabetes mellitus (DM), a criti public health concern. This metabolic condition will lead to life threatening conditions such as persistent microvascular, macrovascular and neuropathic effects (1). Diabetes mellitus (DM) is cluster of metabolic illnesses distinguished by constant increase in blood sugar concentration. Blood glucose levels rise as a result of the pancreas' inability to release enough insulin from β-cells or when insulin is unable to connect to its receptors (2). Type 1 diabetes is an autoimmune illness which damages pancreatic cells and reduces or limits the generation of insulin, whereas type 2 diabetes is brought on by loss to the beta cells in the pancreas that limits a person's capacity to utilise insulin (1). Insulin deficiency causes wasting by increasing protein breakdown and inhibiting protein synthesis. Diabetic ketoacidosis are considered as a minor emergency. During the absence of insulin there is a rapid conversion of fat to acetyl-CoA and this leads to the lack of aerobic carbohydrate metabolism resulting in the synthesis of acetoacetate and β hydroxybutyrate which leads to the acidosis, along with acetone (a ketone). As the cells are unable to absorb the glucose that has accumulated in your blood. Increased blood glucose content will harm the small blood vessels of the kidneys, heart, eyes, and nervous system. And this is the reason that when diabetes-notably if not unaddressed can possibly lead heart disease, stroke, kidney disease, blindness, and neurological harm to foots nerve (3). A unusual plasma glucose level (either fasting ≥7 mmol/L or arbitrarily ≥ 11.1 mmol/L) combined with the occurrence of symptoms linked to diabetes. Diabetes can be diagnosed based on symptoms such as water retention, urinary retention, repeated infections, weight loss, exhaustion, and stupor. Glycated haemoglobin, also known as HbA1c is currently advised by the World Health Organization (WHO) as a diabetes diagnostic test. To diagnose diabetes, a normal HbA1c level should be 48 moles per mol (6.5%). However, a value below 48 moles per mol did not imply that the patient does not have diabetes, which has been identified with glucose testing in the past (3). Therefore, it is crucial to conduct drug consumption studies of anti-diabetic medications in order to encourage diabetics to use medications sensibly and to provide the medical staff with useful information. This study examined the drug use patterns of patients with type II diabetes and examined prescriptions using the WHO core drug prescribing indicators.
Types of Diabetes Mellitus:
Type-1 Diabeties:
Type 1 diabetes syndrome (T1DM), that is responsible for 5–10% of all forms of diabetes, can be detected by the immune-mediated breakdown of the beta cells in the pancreatic islets which create insulin. As an outcome, insulin is totally nonexistent. In spite of a family history, plenty of environmental issues, such as substances, infectious viruses, and particular dietary ingredients, are believed to be connected to autoimmune conditions. T1DM tends to appear in young people, although it may occur at any stage in life.
Type 2 Diabetes:
Type 2 diabetes is a worldwide situation that dramatically increases in socially changing cultures, newly industrialized nations, and emerging nations, particularly among the elderly. Insulin is incapable under this state, and to maintain the equilibrium of glucose, the rise in of insulin production occurs. However, type 2 diabetes arises as insulin production declines gradually. Individuals aged 45 and older make up a majority of those suffering type 2 diabetes. However, it is growing more common in children, teens, and young adults owing to spike in obesity, lack of exercise, and foods high calories.
Gestational Diabetes:
Pregnancy-related diabetes mellitus is an operative classification, not a pathophysiologic ailment, that is utilized to women who acquire diabetes mellitus while maternity. Women who establish Type 1 diabetes disorder while pregnant along with those who have undetected silent Type 2 diabetes mellitus which is addressed at the time of maternity is jointly referred to as getting gestational diabetes mellitus (GDM). GDM normally begins to appear in pregnant women within the middle trimester of pregnancy.
Maturity Onset Diabetes of Young:
"Aside from Specific Types" is a category encompassing diabetes mellitus categories with an assortment of identified origins. The majority with inherited deficiencies of function of beta cells (originally referred to as MODY syndrome or maturity-onset diabetes in youth), flaws in the release of hormone, intrinsic pancreatic illnesses like pancreas inflammation or cystic fibrosis, as well as malfunction correlated with multiple conditions (like acromegaly), and pancreatic malfunction triggered by medications, substances, or illnesses reflect under ten percent of episodes of diabetes mellitus.
Physiopathology of Type 1 Diabetes:
The immune system's breakdown of islet cells, escorts to a lack in production of hormones that reduces the blood sugar level which causes the dysfunctional metabolism linked to the illness. In attention to the drop in hormone production, the role of islet α-cells is moreover dysfunctional and there is extravagant glucagon production in individuals with type 1 illness. Typically, diabetes aims to decreased glucagon creation, however, for patients with type 1 illness, glucagon release is by no mean inhibited when blood sugar level is been elevated. The resulting extremely high levels of glucagon increase the metabolic illness due to lack of insulin. The most noticeable hallmark of this metabolic illness is When insulin is not administered, diabetic ketoacidosis occurs rapidly in patients with the condition. Even though a lack of hormone is the major diabetes defect, and also a flaw in the supervision in insulin. Lack of insulin hinders the metabolism of glucose in peripheral tissues, including skeletal muscle, by generating inappropriate lipolysis also with elevated plasma level of free fatty acids. This impairs the accuracy of glucose application, and low levels of insulin further reduces the expression of many genes that enable target tissues to adapt to insulin in an appropriate way, including this enzyme in the liver and the Glucose transporter type 4 category of glucose transporters in the fat cells.
Effect on Glycolysis:
Raised hepatic blood sugar secretion leads to the result of unrestrained Type 1 diabetes illness. Hepatic stored glycogen must first be released before glucose can be produced by hepatic gluconeogenesis. A lack of insulin also affects how glucose is used by non-hepatic tissues. Insulin promotes the uptake of glucose, especially in skeletal muscle as well as adipose tissue. Insulin-mediated trafficking of glucose transporter proteins to these tissues' plasma membranes enables this. Peripheral tissues absorb less glucose, which lowers the rate at which glucose is metabolized. Furthermore, insulin controls the amount of hepatic glucokinase. Thus, higher transport to the blood results from a lower rate of glucose phosphorylation in hepatocytes. Further enzymes associated in the aggressive physiological cycle of sugar are influenced on hormone.
Effect on Lipid Metabolism:
The main purpose of the hormone insulin is to encourage the preservation of nutrients in the manner of carbs by skeletal muscle and hepatocytes following a meal. Moreover, insulin activates hepatocellular which creates as well as maintain triglycerides in adipose tissue. In unmanageable IDDM, triglycerides are quickly energized, raising the quantity of plasma basic fatty acids. With the sole exception of the cerebral cortex, a variety of tissues absorb the free fatty acids then convert them into energy. Absent insulin, fatty acyl-COA transit into the mitochondria occurs and malonyl COA levels decline. Fatty acids undergo oxidization in the mitochondria and produce acetyl COA, that may then undergo additional oxidation in TCA cycle. The majority of acetyl COA in hepatocytes instead metabolized into ketone compounds acetoacetate and b-hydroxybutyrate by the cycle of TCA, as opposed to being oxidized. These ketone molecules are used by heart, brain, and skeletal muscle for manufacturing energy. In IDDM, the raised accessibility of ketone bodies and free fatty acids aggravate the decreased utilization of glucose, leading to hyperglycemia. When the body manufactures more ketone bodies than it can rely on, ketoacidosis occurs. Acetoacetate automatically breaks down to form acetone, which is substance the lungs manufacture and gives breath its characteristic scent. Normally, plasma triglycerides is broken down by lipoprotein lipase (LPL), so they need insulin.
Physiopathology of Type 2 Diabetes:
Despite having the greatest plasma insulin levels, those with prediabetic allowance exhibit increased sugar level, which suggests, they are opposing to the effects of hormone. Insulin levels drop when prediabetic allowance develops into diabetes illness, suggesting that individuals with type 2 diabetes illness secrete less hormone. The typical NIDDM patient has both insulin resistance and insulin insufficiency. NIDDM is primarily caused by insulin resistance, however some researchers argue that insulin shortage is the fundamental cause as well because NIDDM cannot be caused by mild insulin resistance alone. Both abnormalities are present in the majority of individuals with the normal pattern of type 2 diabetes illness. A member of the fission estrogen receptor extremely complex of enzymes is being linked in the origins of diabetes type 2 based upon recent findings. Thiazolidinedione drugs are fairly new types of pharmaceuticals meant to render the body better susceptible to insulin. These chemicals adhere to the peroxisome proliferators-activated receptor g and change the way it functions. In furtherance of being a transcription factor, proliferators-activated receptor g interacts to the retinoid x receptor (RXR) when it is activated. A particular group of genes become activated when these two proteins complex. Fibroblasts alongside other undifferentiated cells are capable of being made into mature fat cell types by proliferators-activated receptor g, an essential supervisor of adipocyte conversion.
Complications in Diabetes Mellitus:
Retinal vascular disease:
One of the main causes of blindness and visual loss in diabetics is diabetic retinal degeneration, a capillary condition that can affect the macula, peripheral retina, or both. Retinal objectivity or vitreous hemorrhage can cause entire or substantial loss of vision. In the previous arrangement, it can be separated into two categories: "expanding diabetic retina" (PDR) and "benign diabetic retina" (NPDR). Capillary divider insufficiency, increased microaneurysm and liquid leakage, and more pronounced leukocyte and monocyte endothelial attachment are the main characteristics of NPDR. Endothelial cell and pericyte retinal capillary degeneration brought on by the prevalence of ischemia and microaneurysm is a defining feature of diabetic retinopathy.
Neuropathy:
In the industrialized world, diabetic polyneuropathy is the most prevalent type of neuropathy and one of the most frequent long-term consequences of diabetes. It includes several neuropathic disorders, the most prevalent of which being diabetic peripheral neuropathy (DPN), also referred to as chronic distal symmetrical polyneuropathy. DPN is linked to cardiovascular disease and a higher risk of death. It also causes significant morbidity, such as neuropathic pain, foot ulcers, and amputations. Poor glucose regulation and indicators of macrovascular disease, like hypertension, are risk factors for DPN. There is now substantial evidence that the cause is nerve ischemia. 15–26% of diabetics have painful DPN, which can cause significant impairment. The diagnosis and treatment of painful DPN remain extremely difficult. Diabetic autonomic neuropathy is linked to a higher risk of death and causes significant morbidity and a decline in quality of life. Thermoregulatory, sudomotor, pupillomotor, urogenital, gastrointestinal, and cardiovascular functions may all be affected. The most severely affected individuals will need pharmacological interventions, even if other people may be effectively managed with counseling and non-pharmacological interventions.
Nephropathy:
Diabetic nephropathy, the most frequent results in kidney deterioration among individuals initiating renal replacement therapy, impacts roughly forty percent of adults with both type one and second-generation diabetes. It enhances the chance of death, mostly arises out of cardiovascular causes, and is described by high urine albumin discharge under the lack of other renal diseases. Diabetic nephropathy occurs in two stages: microalbuminuria (UAE >20 μg/min and ≤199 μg/min) and macroalbuminuria (UAE ≥200 μg/min). The primary risk factors for the development of diabetic nephropathy include genetic predisposition, high blood pressure, and hyperglycemia. High blood cholesterol, smoking, and the quantity and kind of protein consumed appear to be risk factors as well. Five years after getting diagnosed with type 1 diabetes, or earlier if puberty occurred previously, annual the condition screening must begin. Smoking habits, high blood lipids, and the quantity as well as root of protein in the diet also seem to be risk factors. Approximately five years after being diagnosed with type 1 diabetes, or earlier if puberty or poor metabolic control are evident, annual the condition monitoring should start. People with type 2 diabetes should be screened once they are first diagnosed and then frequently thereafter. It is vital to assess patients with both micro- and macroalbuminuria for the presence of associated disorders, notably retinopathy and macrovascular disease.
Cerebrovascular diseases:
The primary factor of diabetes-related illness and death is cerebrovascular illness. Patients with diabetes are at least twice as likely to have a stroke, have symptoms earlier, and have lower functional results than people without the disease. Stroke is one of the main causes of death for diabetes individuals, accounting for about 20% of their deaths. Research cohorts comprising people with and without diabetes have produced effective primary and secondary stroke prevention measures. However, there are several particular factors to take into account when preventing diabetes. In order to help with the diagnosis and treatment of stroke in diabetes individuals, we have compiled the evidence in this publication. Like other patients with cerebrovascular disease, we suggest that diabetic stroke patients should have a thorough risk assessment to guide therapies.
Who Prrscribing Indication
Indication 1
To evaluate the level of polypharmacy, it shows the typical number of medications prescribed. Average, determined by fractioning the whole number of prescriptions surveyed by the amount of medicinal goods directed. Whether, patient actually received the medications is important.
Indication 2
This represents the proportion of medications prescribed under generic names and gauges the propensity to do so. The average is estimated by fractioning the amount of prescriptions for generic medications by the entire number of prescriptions, then increasing the aftermath by 100
Indication 3
The ratio of prescriptions that contain an antibiotic is indicated by this indicator. Measuring the entire amount of antibiotic abuse is the goal. The percentage is determined by fractioning the amount of prescriptions that contained antibiotics with the entire number of prescriptions that were reviewed, then increasing the aftermath by 100
Indication 4
The ratio of prescriptions that include an injection is displayed by this pointer. It assessed the overall prevalence of injectable medication therapy, which is an expensive and overused modality. The average is estimated by fractioning the amount of scripts that included injections by the entire number of prescriptions that were inspected, then increasing the aftermath by 100.
Indication 5
This calculated the proportion of medications prescribed from formularies or essential drug lists. Assessing how closely prescribing procedures adhere to the Fifth Edition of the Ethiopian National Medicine List is useful. The ratio is determined by partitioning the entire digit of prescription medications by the number of medications that are on the local formulary or essential pharmaceuticals list, then multiplying the result by 100.
Pharmacological Agents:
|
Classification Of Anti-Diabetic Drugs |
Agents |
Route Of Adminis- Tration |
Mechanism of Action |
Adverse Effects |
|
Biguanide |
Metformin |
Oral |
Sensitizer to insulin
|
Anemia and neuropathy can result from a vitamin B12 deficiency (risk in elderly) Very safe medication; nevertheless, if a person's Men's and women's creatinine concentrations vary more than 1.5 and 1.4 mg/dL, accordingly. discontinue taking metformin. |
|
Dipeptidyl peptidase 4 [DPP-IV] inhibitor |
Sitagliptin Saxagliptin Vidagliptin Alogliptin Linagliptin |
Oral |
Prevention of GLP mortification
|
URTI, Pancreatits. |
|
Sodium glucose Cotransporter [SGLT2] inhibitor |
Canagliflozin Dapagliflozin Empagliflozin |
Oral |
Presence of glucose level in urine brought on by renal PCT's 90% blockage of glucose reabsorption; insulin-independent mode of action |
Ketoacidosis, Bone fractures, Genital mycosis. |
|
Insulin |
Humulin R Novolin R Levemir Tresiba Lispro Aspart Apidra |
Parental |
Insulin receptor activation and subsequent signaling in several delicate tissues
|
Lipohypertrophy and lipoatrophy at locations of injection Intolerance to injection ingredients for gestational diabetes mellitus, the Levemir Food and Drug Administration has granted approval. |
|
GLP 1 agonist |
Liraglutide Exenatide Dulaglutide |
Parental |
Turn on the GLP1 receptor |
Pancreatitis, nausea, vomiting, and thyroid C cell tumors (which are contraindicated in MEN type 2)
|
Analysis of Anti-Diabetic Drugs Prescribed:
|
Drug Class |
Total Prescr- Iption |
Prescription Share in Niad Or Insulin (%) |
Cases(N) |
Medications |
Prescriptions Shae In Class |
|
Noninsulin antidiabetic drug |
121055250 |
100 |
16316580 |
|
|
|
Biguanides |
60368335 |
49.9 |
11792980 |
Metformin
|
100.0 |
|
Sulfonylurea |
32341020 |
26.7 |
6121488 |
Glipizide Glimepiride Glyburide Chlorpropamide Tolbutamide Tolazamide Acetohexamide |
44.7 33.0 22.3 <0.1 <0.1 <0.1 <0.1 |
|
DPP-4 Inhibitor |
9703821 |
8.0 |
1870819 |
Sitagliptin Saxagliptin Linagliptin |
76.4 17.3 6.4 |
|
AD\AD combination |
8109413 |
6.7 |
1504542 |
Sitagliptin\Metformin Glyburide\Metformin Pioglitazone\Metformin Saxagliptin\Metformin Glipizide\metformin Pioglitazone\Glimepiride Linagliptin\Metformin Repaglinide\Metformin Rosiglitazone\Metformin Rosiglitazone\Glimepiride |
38.5 35.1 11.8 9.8 3.5 0.8 0.5 0.1 <0.1 <0.1 |
|
Thiazolidinediones |
5770131 |
4.8 |
1083193 |
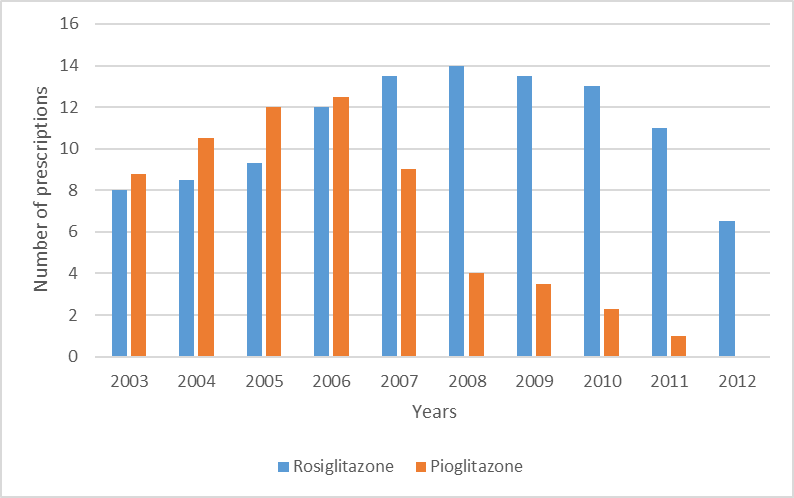
Pioglitazone Rosiglitazone |
100.0 <0.1 |
|
GLP-1 Analogs |
3136564 |
2.6 |
673367 |
Liraglutide Exenatide |
59.1 40.9 |
|
Alpha glucosidase inhibitor |
356852 |
0.3 |
80506 |
Acarbose Miglitol
|
92.0 8.0 |
|
Meglitinide |
1079356 |
0.9 |
226628 |
Repaglinide Nateglinide |
54.0 46.0 |
|
Analog human long acting |
17311225 |
51.8 |
3650111 |
Insulin Glargine Insulin detemir |
81.3 18.7 |
|
Analog human fast acting |
9056523
|
27.1 |
2172770 |
Insulin aspart Insulin lispro Insulin glulisine |
51.8 43.8 4.4 |
|
Miscellaneous |
53 |
<0.2 |
36 |
Animal Insulin, Persistent human insulin, Insulin zinc, Insulin Human (Isophane\Regular) |
100.0 |
Analysis of The Prescriptions:
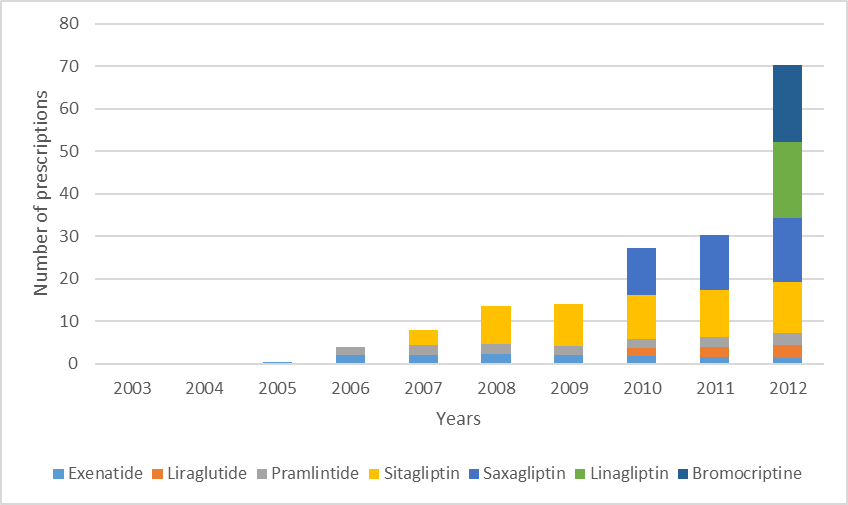
B. Between 2003 and 2012, scripts for newly permitted noninsulin diabetes medications were submitted in US clinics.
CONCLUSION:
This study expands on earlier research on the use of antidiabetic medications by examining both current and nationally projected data. The main findings include A consistent rise in the overall number of scripts and patient usage of antidiabetic medications in Retail drugstores in the US; the number of antidiabetic medication users (18.8 million) (22) closely matched the CDC's 2010 estimate for diagnosed diabetes cases, although not all diabetic patients use these medications; metformin was the most prescribed noninsulin antidiabetic drug, accounting for half of all prescriptions; it is now the first-line therapy advised by diabetes associations, with 62.7% of patients using it in 2012, primarily as monotherapy; sulfonylurea use decreased, while newer drugs such as Dipeptidyl peptidase-4 inhibitor and Glucagon-like peptide-1 analogs, such as liraglutide, increased their market share. A limitation of the study is that it only included prescriptions filled at retail pharmacies; data from mail-order pharmacies or nonretail settings were not included. The study also demonstrated a 42.9% increase in patients filling antidiabetic prescriptions from 2003 to 2012, with metformin remaining the most prescribed drug. Despite recommendations that metformin be used with other medications, a large percentage of patients used drugs such as sulfonylureas, Dipeptidyl peptidase-4 inhibitor and Glucagon-like peptide-1 analogs without metformin (24). The research stresses the relevance of recognizing these patterns, especially with reference to treatment adherence and the implications of pharmaceutical choices in diabetes control..
REFERENCES


K. Sowmya Sri*, J. Kabilan, Dr. K. Karthickeyan, Dr. P. Shanmugasundaram, A Review on the Prescription Pattern Analysis of the Diabetes Mellitus, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 2571-2581. https://doi.org/10.5281/zenodo.15429215
 10.5281/zenodo.15429215
10.5281/zenodo.15429215
