Rungta Institute of Pharmaceutical Sciences and Research, Kohka, Bhilai.
Psoriasis is a chronic autoimmune skin condition characterized by rapid skin cell proliferation, inflammation, and scaling. Safer alternatives need to be looked into because of the possible negative effects of traditional therapies such immune suppressants and corticosteroids. Because of their potential efficacy and minimal side effects, herbal formulations have attracted attention.
Persistent inflammation is a hallmark of psoriasis, a common and persistent inflammatory skin disorder. Globally, it affects 2–5% of people, depending on cultural demography, age, gender, and location. Notably, psoriasis is more common in Europeans than in other ethnic groups. Red, inflammatory skin plaques and macules are the condition's outward manifestation. Poor differentiation and excessive proliferation of the keratin-producing epidermal cells are the causes of these symptoms. Silver scales are often seen with these plaques. Due to impaired immunological signaling, the keratin-producing cells' mitotic rate increases tenfold in these lesions, resulting in increased inflammation. Certain chemical traits, such the emergence of erythematous and scaly skin lesions, set it apart. Usually, the scalp, lower back, and the area surrounding knees and elbows are where these lesions show up. Eventually, they might extend to the forehead, back of the neck, arms, chest, and behind the ears. Prominent features of psoriatic skin, as shown by histopathological analysis, include elevated angiogenesis, notable inflammatory infiltrates, and epidermal hyperplasia with significant keratinocyte differentiation.
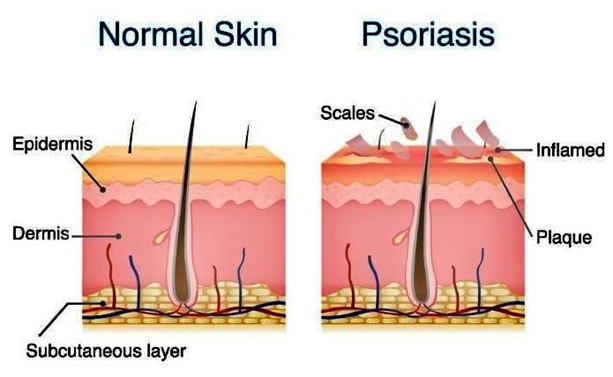
Fig 1 Psoriasis
Numerous underlying variables contribute to this disorder, including a combination of genetic (family history) and environmental (alcohol, infections, medications, stress) factors. Together, these factors result in the immune -histological changes observed in the skin. Since psoriasis is a chronic condition, management and treatment approaches vary according to the severity of the issue. Topical medicine is the initial line of treatment for mild to moderate psoriasis. These kinds of psoriasis respond favorably to this treatment. However, for more serious conditions, such as high severity circumstances, systemic medicines or phototherapy are recommended treatments. In the realm of managing psoriasis, treatment options are informed by a comprehensive understanding of the severity of the problem. Topical medicines, which are crucial for symptom alleviation, are the main therapeutic strategy for mild to severe cases. Natural product development has recently showed promise as an adjunct to conventional techniques. Notably, certain natural remedies have properties that could lessen psoriasis symptoms. Aloe Vera, which is well-known for its anti-inflammatory qualities, hydrates and calms skin, while fish oil supplements, which are rich in omega-3 fatty acids, aid in reducing inflammation and promoting skin health.While tea tree oil, colloidal oatmeal, and Dead Sea salt show promise in terms of moisturizing, exfoliating, and reducing itching, turmeric's curcumin molecule has anti-inflammatory and antioxidant qualities [9–11]. Additionally, apple cider vinegar for pH balancing and limited sun exposure for increased vitamin D generation appear to be complementary strategies. Working with medical professionals is still necessary to provide a seamless transition with traditional medications and optimize the holistic care of psoriasis, even though adding these natural things offers a major approach.
2 History
2.1 Psoriasis in The Old Age
The medicine came from Mesopotamia, which was home to Babylon, Assir, and Sumer. The earliest written documents on their medicine are clay tablets from 3000-5000 years ago (Radbill, 1975). Although priests and seers were usually the ones who cured skin disorders, Mesopotamian physicians, known as asu, were aware of them. Psoriasis is absolutely not present.
According to Herodotus, in pharaonic Egypt, there was a physician for every organ. A range of drugs were used, along with enchantments and magical ceremonies (Herodotus, 1989). But they don't mention psoriasis in their medical papyruses. The longest writing, the Ebers papyrus, which was written in the 15th century BC and found near Luxor in 1873, contained descriptions of numerous skin disorders (paragraphs 90–95 and 104–118). The phrase "šuf.t" meaning scale was found, but psoriasis could not be identified (Ebbel, 1937). The religious medicine known as Ayurveda has its roots in ancient India. It was based on magic-religious rituals using particular plants. One of the most important medical books of the time was the Charaka Samitha. Both this document and the Bower manuscript mentioned in passing the illness called Khusta. It was probably leprosy, but Paul Richter believed it to be psoriasis (Menon & Haberman, 1969; Richter, 1928).
2.2 Psoriasis in the Middle Age
After the Roman Empire fell because of the Goths, there was a period of stagnation known as the Dark Ages, which hindered scientific progress (Porter, 1999). In a medical system full of superstition, ignorance, and mysticism, skin diseases received little care, and the literate males were confined to convent cloisters. Hebra asserts that authors spent their time making meaningless comments on the great authors of antiquity, whether or not they were physicians, even when the cause of the ailments was unknown (Bechet, 1936). The majority of people were treated by often illiterate barbers and quacks. Arabian doctors may have been the first to distinguish psoriasis from other skin disorders in the seventh century A.D., and it seems that they used psychotherapy to treat it (Shafii&Shafii, 1979). Constantine the African founded the first medical school in Western Europe in Salerno by translating old medical literature from Greek and Arabic to Latin. By the 13th century, Latin had become the dominant language of the educated, with most manuscripts translated into it.
2.3 Psoriasis in the Renaissance
The Renaissance was a cultural movement that roughly spanned the 14th through the 17th centuries, beginning in Florence in the Late Middle Ages and later spreading to the rest of Europe. Lepra and psora were mentioned in the writings of some authors of the era.In his "Epistolaemedicinales," Ferrara native Johannes Manardi (1462-1536) mentioned the disease called "psora," but he didn't write anything more about it (Manardi,1542). The most important book on skin illness was written by Hieronymus Mercurialis, a medical professor at the universities of Padua and Bologna (1530–1606). "De morbiscutaneis et omnibus corporis humaniexcrementis," a treatise produced by his pupil Acardius, was based on his teachings. This book was "the first systematic text book on diseases of the skin," Garrison said. Like Galen's "a capite ad pedes," Mercurialis categorized skin diseases into those that affected the scalp and then the entire body. Variations in bulk, color, and structure were used to further categorize these diseases. He referred to psoriasis as "lepra grecorum" and other disorders as "psora" (Mercurialis, 1572) In his 1700 publication "De morbisartificumdiatriba," B. Ramazzini (1633–1714) enumerated a number of illnesses, including skin conditions, that were caused by engaging in specific occupations. Ramazzini discovered many new causes of illness, in opposition to Hippocrates' theory of a dyscrasia of humors (Ramazzini, 1700).
2.4 Psoriasis in 18th Century
In the 18th century, a few physicians and surgeons made an effort to concentrate solely on the study of skin conditions. Among them was Daniel Turner (1667–1740), who started out as a surgeon before graduating from Yale University in America with an honorary degree in medicine. The 1714 publication of his treatise, "De morbiscutaneis a treatment of diseases incident to the skin," began. It was swiftly translated into a number of languages and saw multiple editions (Turner, 1726). His description of the psoriasis he called "leprosy of the Greek" was inaccurate, but our leprosy was called "leprosy of the Arabian." He was aware that ointments and drugs were transported internally when they were applied topically. In the second part of the 18th century, the famous Swedish scientist and physician Carl Linnaeus (1707–1787) created the binomial language and made the first comprehensible classifications of plants. His book "Systema naturae" was published in 1735, and in his "Genera morborum," he even proposed a system of classification for human illnesses (Linnaeus, 1763). Francois Boissier de Sauvages classified diseases into ten classes with almost 2400 species in his work "Nosologiamethodica" (Grmek, 1996) on the same topic. Such classifications were quickly used to classify skin diseases.
2.5 Psoriasis in the 19th Century
In the 19th century, dermatologists continued to disagree on how to classify skin problems. Dermatology and psoriasis grew and evolved with the introduction of pathohistological classifications (F. Hebra, Auspitz). In reference to psoriasis, it is worth noting that Besnier coined the name arthritis psoriatica in 1822 following Alibert's observation that the ailment was associated with abnormalities of the joints (Alibert, 1818). The association between psoriasis and rheumatic and gout disorders was first described by Erasmus Wilson and then further developed by Charles Bourdillon (Bourdillon, 1888). Barber-Königsbeck subsequently described psoriasis palmo-plantaris, while Leo von Zumbusch (1884–1940) initially described the forms of psoriasis in 1910 with psoriasis pustulosa generalisata (von Zumbusch, 1910). The identification of the condition was made easier by the symptoms several authors reported. The isomorphous effect of irritation, also referred to as the Köbner phenomenon—the development of a psoriatic lesion at the site of a physical or other harm—was described in 1872 by Heinrich Köbner, a dermatology professor at Breslau from 1838 to 1904 (Köbner,1877). This phenomenon was later used to experimentally study the early changes in the disease.
2.6 Psoriasis in the 20th Century
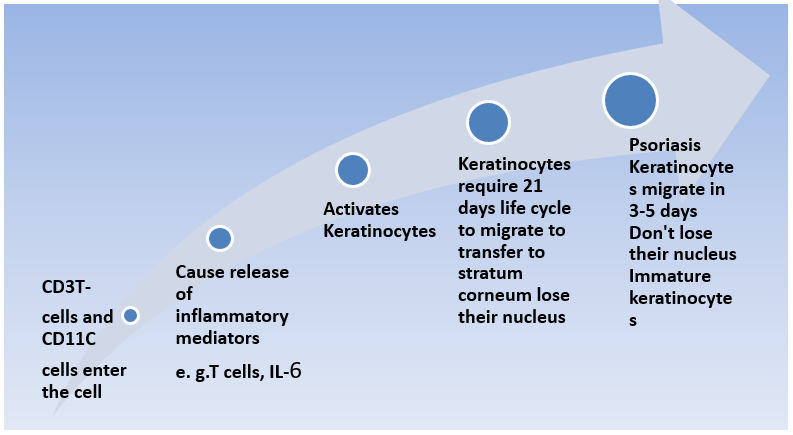
In the early 1900s, the Woronoff ring was observed surrounding the psoriatic plaque (1926), notably following antrarobin treatment (Woronoff, 1926; Kogoj, 1927). The Zagreb-based physician Franjo Kogoj (1894–1981) was the first to describe the spongiform pustule in pustular psoriasis in 1927. Through an ultramicroscopic study, Mladen Rupec enhanced this description (Kogoj,1927; Rupec, 1970). The epidermis of psoriatic people has 25 times as many mitoses per unit as that of healthy people, according to research conducted in the second half of the 20th century. The turnover time of the epidermis is dramatically reduced from 27 days to 4 days (Weinstein, 1968), and the cell cycle of keratinocytes in psoriatic patients is significantly shortened from around 311 hours in a normal individual to 36 hours (van Scott, 1963). Ekel and van Scott demonstrated this. Throughout the 20th century, many researchers studied genetic change, and there is now indisputable evidence that the disease is multifactorial—that is, caused by multiple genes. There are several "susceptible" genes (PSOR1–PSOR10) on different chromosomes. The syndrome may be brought on by a variety of environmental factors (Sanchez, 2007; Bowcock & Barker, 2003).
2.7 PsoriasisTherapy throughout History
Psoriasis instances treated with boiled viper broth or an ointment containing ammoniated mercury (Hydrargyriamidochlorati) are accurately described by D. Turner in his book (Turner, 1726). Such treatment-related facts are fascinating, but they are not relevant to our article. We shall talk about how psoriasis was treated beginning in the early 19th century because the diagnosis was somewhat contentious prior to that time and the therapy was usually challenging and inventive.The treatment was topical and/or internal, of course, but for a long time the doctors concentrated more on the latter since they believed that externally administering drugs to the skin could cause the lesions to press inward and cause "metastases" to the internal organs. Hebra asserted that this was only speculation.
2.8 Psoriasis Treatment inthe 19th Century
One of the earliest drugs taken internally to treat psoriasis was arsenic. Thomas Girdlestone was the first to use potassium arsenite as a Fowleri solution in 1806, after moderate use, usually 6 drops three times a day (Girdlestone, 1806). This solution was introduced into medicine in 1780 by the English physician and pharmacist Fowler (Fowler, 1786). The drug was easily absorbed and dispersed throughout the body, especially in the skin and hair, by inhibiting specific enzymes. Many years later, F. Hebra, M. Kapsi, and E. Wilson also proposed the use of solutioFowleri (before a meal in water or a bland tea) and Pilulaeasiaticae (a concoction of arsenic, black pepper, acacia, and water) to cure psoriasis (Bechet, 1936).Psoriasis guttata seems to have benefited the most from arsenic compounds, however other forms of the condition have also occasionally improved.
2.9 In the 20th Century, Psoriasis Treatment
Around the turn of the century, new drugs to treat diseases were developed thanks to developments in chemistry and technology, especially in Germany and England. Dithranol, also referred to as citrolin, was developed in 1916 by chemist Galewsky, making psoriasis easier to treat. It was initially used by PC Unna and the Galewsky brothers (Galewsky, 1916). It was initially applied as a paste or ointment (0.1%) for the short-term treatment of psoriasis, and then as a stick.
2.10 The 21st Century Is The Future.
Decades of studies have shown the importance of immunological pathways in the reappearance of psoriasis. In our opinion, the application of biological agents to treat psoriasis and further knowledge of the pathophysiology of the condition (Tutrone et al., 2004) will encourage the future use of drugs that target specific receptors (IL-2), cytokines, chemokines, or other lymphocyte molecules (Mrowietz, 2003). Humanized or recombinant monoclonal antibodies and fusion proteins will be utilized to treat psoriasis because of their ability to interact with molecules on the surface of antigen-presenting cells or lymphocytes, such as CD4 and CD2.Others may prevent some proinflammatory cytokines that change the TH1 to TH2 immune response, like interleukins or tumor necrosis factor α. It is critical to monitor for infections and autoimmune responses.
3 Disease
Because of the rapid buildup of skin cells, psoriasis is a chronic autoimmune disease that causes inflammation and scaling. This results in red, itchy, and often painful patches of skin, typically on the scalp, elbows, knees, and lower back. The exact cause is unknown, although it is believed to be connected to an overactive immune system where T-cells unintentionally attack healthy skin cells.
3.1 Etiology of Psoriasis
3.1.1 Immunological Factors:
When autoimmunity is present, the body attacks itself. Psoriasis is one kind of autoimmune disease. WBCs induce scrap infection by invading and eliminating invasive bacteria. In psoriasis, T lymphocytes target the skin cells. It is possible that this onslaught will speed up the production of skin cells. The increased production of skin cells leads to an overabundance of new skin cells. The hyperproliferated skin cells migrate toward the skin's outer layer wherever they gather.
3.1.2 Genetic Factors:
One of the causes of psoriasis is its hereditary component, which is exacerbated by familial aggregation. First and second generations of afflicted people are more likely to have emergent psoriasis. The odds are two to three times higher for monozygotic twins and two to three times higher for dizygotic twins. Thus far, comprehensive linkage investigations of families affected by psoriasis have identified at least 60 chromosomal loci linked to psoriatic susceptibility. PSORS1 is found inside the major histocompatibility complex7,8 on chromosome 6P21. PSORS1 is exposed to more than 50 single-nucleotide polymorphisms (SNPs), which are risk factors for psoriasis.
3.1.3 Environmental Factors:
Environmental factors such as UV radiation, mechanical damage, a variety of disorders, chemical damage, prescription drugs, and smoking can all cause psoriasis. Psychological stress is another factor contributing to psoriasis.
Table No.1
|
Environmental Factors |
Immunological Factors |
Genetic Factors |
|
|
|
3 Types of Psoriasis
3.1 Plaque psoriasis;
Is the most common kind of psoriasis, accounting for 80–90% of cases. This chronic autoimmune condition results in thick, puffy patches of skin with silvery-white scales because skin cells undergo rapid changes. These plaques are not only disagreeable and itchy, but they can also occasionally bleed or shatter.

Fig 2 Plaque psoriasis
3.2 Guttate psoriasis;
The sudden appearance of small, drop-shaped red or pink skin patches, often coated in microscopic, silvery scales, is a characteristic of this kind of psoriasis. It is most commonly seen in children and young adults, but it can afflict people of any age. After plaque psoriasis, it is the second most common form of psoriasis. Compared to the thick, raised plaques of plaque psoriasis, the spots of guttate psoriasis are typically smaller and more widely distributed over the body.

Fig 3 Guttate Psoriasis
3.3 Inverse psoriasis;
Is a kind of psoriasis that mostly affects the skin folds under the breasts, in the armpits, groin, and around the genitalia and buttocks. Unlike the more common forms of psoriasis, which show up as thick, scaly plaques, inverse psoriasis is characterized by smooth, bright red patches of skin that are often glossy and may appear inflamed. Since inverse psoriasis typically lacks the thick, silvery scales found in other types of psoriasis, it can occasionally be more difficult to diagnose.

Fig 4 Inverse Psoriasis
3.4 Pustular psoriasis;
A severe form of psoriasis is characterized by white, pus-filled blisters (pustules) surrounded by red, swollen skin. These pustules are not contagious since they contain neither bacteria nor fungus. Localized pustular psoriasis can affect only specific areas of the body, such as the hands and feet, or it can affect large regions of the body.

Fig 5 Pustular Psoriasis
3.5 Erythrodermic psoriasis;
Is a severe and rare form of psoriasis that affects the entire body, resulting in widespread redness and irritation as well as the shedding of massive, continuous sheets of skin. This type of psoriasis is characterized by severe redness, swelling, and the disintegration of the skin's protective layer. It can result in skin that is extremely dry and cracked. In some cases, it may also result in severe pain, itchiness, or even a burning sensation.

Fig 6 Erythrodermic Psoriasis
3.6 Nail psoriasis;
Is a condition when psoriasis, an inflammatory disease that accelerates the growth of skin cells, affects the nails. In addition to the typical red, scaly skin areas, psoriasis can cause a variety of structural and cosmetic issues when it affects the nails. These changes include discoloration, thickness, cracking, pitting (small indentations), and even the nail moving away from the nail bed.

Fig 7 Nail Psoriasis
3.7 Psoriatic arthritis;
Some people with psoriatic arthritis (PsA), an inflammatory form of arthritis, also have psoriasis, a skin condition characterized by red, scaly areas. PsA is a disorder where the immune system mistakenly attacks healthy joint tissue, resulting in inflammation, pain, and stiffness in the joints. The fingers, toes, wrists, knees, and lower back are the most commonly affected joints, though it can affect every joint in the body.

Fig 8 Psoriatic Psoriasis
4.Dosage form-
Table No 2
|
S No. |
API Drug |
Brand Name |
Dose Form |
Quantity |
|
01 |
Apremilast |
Otezla |
Tablet |
30mg |
|
02 |
Calcipotriene |
Dovonex |
Ointment |
20g |
|
03 |
Tazarotene |
Tazorac |
Cream |
30g |
|
04 |
Acitretin |
Soriatane |
Capsule |
25mg |
|
05 |
Adalimumab |
Humira |
Injection |
40mg/0.4ml |
|
06 |
Etanercept |
Enbrel |
Injection |
25gm/0.5ml |
|
07 |
Infliximab |
Remicade |
Powder for Injection |
100mg |
|
08 |
Ustekinumab |
Stelara |
Injection |
45mg/0.5ml |
|
09 |
Secukinumab |
Cosentyx |
Powder for Injection |
150mg/ml |
|
10 |
Ixekizumab |
Taltz |
Injection |
80mg/ml |
|
11 |
Methotrexate |
Rheumatrex |
Injection |
250mg/10ml |
|
12 |
Cyclosporine |
Sandimmne, Neoral |
Capsule |
100mg |
5New Drugs-
6 Patent-
Table No. 3
|
S. No. |
Authors |
Title |
Patent no. |
Submission |
Publication |
|
01 |
Dingjiang Liuat all |
Method of treating psoriasis using an il-17 receptor antibody formulation |
US20180346583A1 |
2018-08-02 |
2018-12-06 |
|
02 |
Sumon K. PAL |
Systems and methods for applying electrical energy to treat psoriasis |
US20200297999A1 |
2020-04-07 |
2020-09-24 |
|
03 |
James W. Edingerat.all |
Treatment of psoriasis using placental stem cells |
US8753883B2 |
2011-05-13 |
2011-11-17 |
|
04 |
Achim Guettnerat.all |
Methods of treating psoriasis using IL-17 antagonists |
US11534490B2 |
2019-12-19 |
2020-06-04 |
|
05 |
Gordon J. Dowat.all |
Topical compositions and methods for treating psoriasis |
US11648256B2 |
2022-11-23 |
2023-03-23 |
|
06 |
Ann Begovichat.all |
Genetic polymorphisms associated with psoriasis, methods of detection and uses thereof |
US10920276B2 |
2018-05-29 |
2019-01-24 |
|
07 |
Michael E. Silver |
Method For Treating Psoriasis |
US11517552 B2 |
2020-09-03 |
2021-02-04 |
|
08 |
Birkir SVEINSSON |
Use of CGRP antagonist compounds for treatment of psoriasis |
US10668132B2 |
2016-11-18 |
2017-03-09 |
|
09 |
Rebecca S. Hoffman at. All |
Use of TNFa inhibitor for treatment of psoriasis |
US9090689B1 |
2015-04-08 |
2015-07-28 |
|
10 |
Evan Anderson at. all |
Phototherapy dressing for treating psoriasis |
US10058711B2 |
2016-06-20 |
2016-10-06 |
7 CONCLUSION-
Pharmaceutical gels are increasingly being used because they provide controlled release and are more stable than other semisolid dose forms. By improving the skin's capacity to absorb medications, the topical gel raises bioavailability. A topical administration method's main advantage is that it avoids first-pass metabolism. Additionally, it has a high rate of patient acceptability.When the bioavailability of another medication administration method is lower, topical distribution is usually selected. Topical gel is a safe and effective therapy choice for skin-related disorders, according to clinical data.
REFERENCES

Sanjay Kumar*, Pawan Kumar, Tulsi Ram, Anjli Sahu, Review on Poly Herbal Gel for Treatment of Psoriasis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 2645-2657 https://doi.org/10.5281/zenodo.15095037
 10.5281/zenodo.15095037
10.5281/zenodo.15095037
