Department of Chemical Technology, Dr Babasaheb Ambedkar Marathwada University, Chhatrapati Sambhajinagar, Maharashtra, India 431004
Transdermal Drug Delivery Systems (TDDS) have emerged as a pivotal facet of modern pharmacotherapy, offering a non-invasive route for systemic drug administration while enhancing patient compliance. This paper provides a comprehensive review of the historical evolution of TDDS, detailing its generational advancements and mechanisms of action. Various types of transdermal patches are explored, alongside their technical sophistication, advantages, and disadvantages. Key desirable features for effective transdermal patches are discussed, as well as potential adverse events associated with their use. The paper delves into the intricacies of skin and percutaneous absorption, highlighting the role of penetration enhancers and the multiple factors influencing transdermal permeability, including physiological and formulation characteristics. Conditions favoring and opposing the use of TDDS are examined, with a focus on drug selection, formulation strategies, and preparation methods. Evaluation techniques for assessing TDDS effectiveness are outlined, followed by an exploration of contemporary development approaches and advanced techniques aimed at enhancing TDDS performance. Finally, future directions and challenges facing the field are identified, underscoring the ongoing need for innovation in transdermal delivery technologies.
A transdermal drug delivery system (TDDS) is a method of delivering medication through the skin for systemic effects. It typically involves the use of patches that contain a specific dose of the drug, which is absorbed into the bloodstream via the skin. This approach allows for the controlled release of the drug over time, improving patient compliance and minimizing side effects compared to other routes of administration. Transdermal drug delivery systems (TDDS) offer an alternative to oral administration, providing sustained release of therapeutic agents and improving patient compliance.[1] TDDS is especially useful for patients unable to take oral medication, such as those experiencing vomiting or unconsciousness, and bypasses first-pass metabolism, reducing side effects associated with oral drugs.[2] However, TDDS efficacy depends on factors such as skin permeability, which varies among individuals, and the physicochemical properties of the drug.[3] While the market for TDDS is growing, challenges like skin irritation, variability in drug absorption, and optimizing drug delivery rates remain.[4] Adverse Despite progress, there is a gap in understanding how to enhance permeation while reducing adverse reactions. This review aims to explore the present scenario of TDDS, identify its advantages and disadvantages, and propose innovative strategies to optimize drug delivery, ensuring safety and improving clinical outcomes.
The human skin, the largest organ of the body, acts as a protective barrier while enabling transdermal absorption of substances. It comprises three main layers epidermis, dermis, and hypodermis. Each with distinct roles that influence skin function and drug permeability.[5]
The skin regulates body temperature, contributes to sensory perception, and aids in vitamin D synthesis. The stratum corneum plays a crucial role as a barrier to penetration, yet drug absorption can effectively occur through two primary pathways (Figure-1):
The Trans epidermal pathway involves drug absorption through the skin's outermost layer, the stratum corneum, which acts as a complex multi-layered barrier.[11] This pathway can be further divided into two distinct routes:
The trans appendageal pathway allows drugs to pass through skin appendages, such as hair follicles and sweat glands. This route is akin to utilizing tiny tunnels within the skin, facilitating the movement of specific substances. [15], [16]
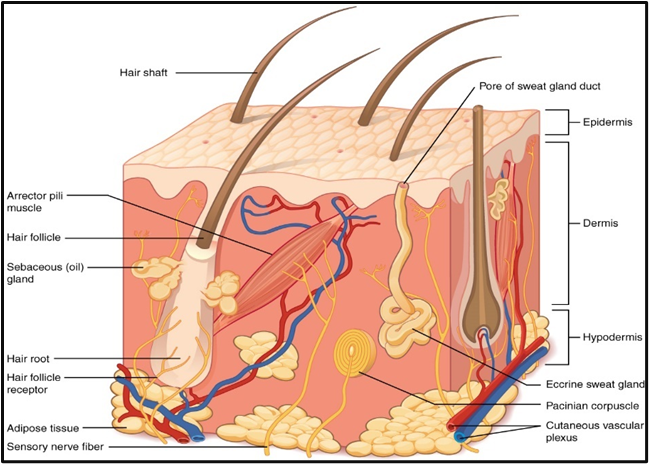
Figure 1: The Structure of human skin
The way of using the skin as a pathway for delivering medications spans thousands of years, with roots in ancient practices and evolving through modern science.
The first generation of transdermal delivery systems has laid the groundwork for the transdermal patches currently used in clinical practice. These patches are designed as reservoirs, encased with an impermeable backing on one side and an adhesive layer on the other, which contacts the skin.[23] The ideal candidates for first-generation systems are low-molecular-weight, lipophilic compounds that demonstrate efficacy at low doses.[24] Such candidates are preferred particularly when transdermal delivery offers advantages over oral routes, such as low bioavailability, less frequent dosing, and consistent delivery profiles. Despite the initial success and increasing public acceptance, the growth of this generation is anticipated to decline as the availability of suitable drugs diminishes (figure-2).
The second generation of TDDS recognizes the need for enhanced skin permeability to broaden the range of applicable drugs. This generation employs various methods to disrupt the stratum corneum, thus facilitating drug transport.[25] Techniques such as chemical enhancers, iontophoresis, and non-cavitation ultrasound have been developed, but they often struggle to balance increased permeation with the protection of deeper tissues. For example, chemical enhancers can disrupt the stratum corneum's lipid bilayer but may lead to skin irritation. Iontophoresis employs low-voltage electrical currents to aid drug transport, while ultrasound enhances permeation but risks thermal damage to deeper tissues. Overall, the second generation has primarily advanced the delivery of small molecules, with limited success in macromolecule transport.[26]
The third generation represents a significant leap in transdermal technology, focusing on targeted disruption of the stratum corneum while protecting underlying tissues.[27] This generation utilizes innovative techniques such as electroporation, cavitation ultrasound, microneedles, thermal ablation, and microdermabrasion to deliver macromolecules, including therapeutic proteins and vaccines, effectively through the skin.[28] By localizing the effects to the stratum corneum, these methods allow for more aggressive strategies that enhance drug delivery without compromising safety.
Microneedles are a noteworthy advancement in this generation. These micro-structured devices can painlessly penetrate the skin, enabling the delivery of a variety of compounds, from small molecules to proteins and vaccines. They have been shown to achieve therapeutic levels in clinical trials, demonstrating their potential for effective transdermal drug delivery.[29]
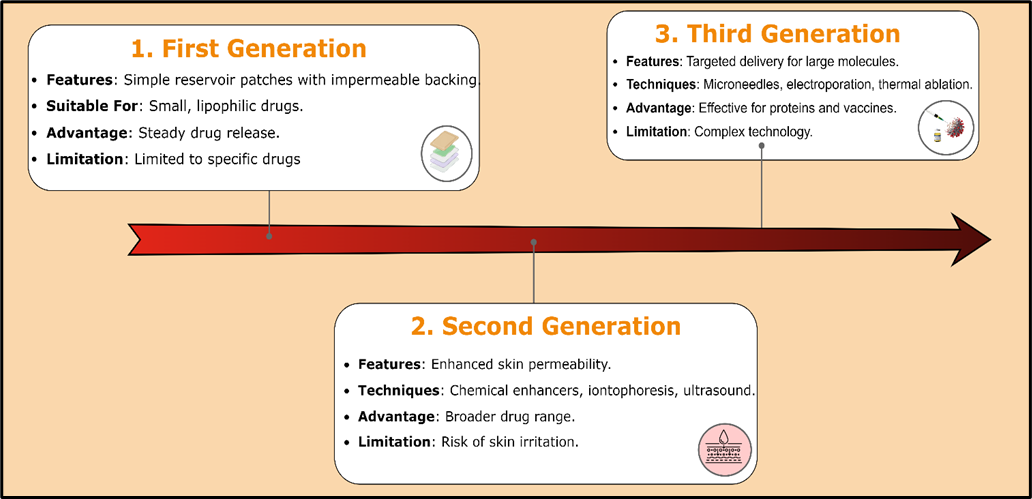
Figure 2: Generations of TDDS.
Transdermal drug delivery (TDD) has seen substantial growth in recent years, becoming a key focus in non-invasive drug administration. Currently, more than 35 TDD products are available in the U.S. market, and there are around 16 distinct active ingredients that have been officially approved for use in transdermal delivery systems worldwide.[30] This rise is fueled by the demand for convenient, effective alternatives to oral and injectable drugs, offering steady, controlled drug release directly through the skin. [31]
These patches cover a range of therapeutic areas, with products for pain management, hormone therapy, cardiovascular issues, and more. Each product is tailored for specific conditions, and marketed under familiar brand names that reflect the system’s purpose and benefits. As the popularity of TDD continues to grow, we can expect more innovations to address both existing and emerging therapeutic needs, demonstrating TDD's potential in modern medicine. [32], [33]
It refers to the movement of drug molecules into and within the biological environment, involving various processes of drug transport across cell membranes.
J= -D×dCdx
Were,

Drug permeation can occur through distinct pathways:
A. Lipid Pathway
B. Aqueous Pathway
In this configuration, the adhesive layer integrates the drug directly within it. The dual role of the adhesive is to ensure adherence to the skin and to control drug release. The rate of drug diffusion is influenced by various factors, including the skin's permeability and the adhesive's properties. This simple design is advantageous for ease of manufacturing and application (figure-3).[40]
Building on the single-layer model, the multi-layer drug-in-adhesive patch includes additional layers, which may consist of membranes or extra drug-containing adhesive layers. This complexity allows for differentiated drug release profiles, enabling both rapid and sustained release phases. Such designs enhance the versatility of dosing regimens and can improve patient compliance. [41]
The reservoir patch distinguishes itself by featuring a dedicated compartment for the drug and is generally available in a liquid or gel format. A semi-permeable membrane controls the drug's release rate, facilitating zero-order kinetics, where a constant amount of drug is delivered over time. This system's ability to maintain stable serum drug levels makes it ideal for chronic conditions, with examples including Duragesic® and Estraderm®. [42]
In matrix systems, the drug is evenly dispersed within a polymer matrix, allowing for controlled release. This category can be further divided into:
The adhesive layer incorporates the drug, providing both adhesion and a drug reservoir in a single formulation.
The active pharmaceutical ingredient is uniformly integrated with hydrophilic or hydrophobic polymers, forming a medicated disk mounted on an impermeable backing layer. The surrounding adhesive rim ensures the patch remains secure during use.[43]
Vapour patches are a novel innovation in transdermal delivery, designed to release essential oils for therapeutic effects, such as decongestion or sleep improvement. These patches not only adhere to the skin but also serve as a delivery mechanism for volatile compounds, making them suitable for users seeking alternative or adjunct therapies.[44]
Combining elements of both reservoir and matrix systems, the micro reservoir design consists of drug particles suspended in a polymer matrix. The resulting formulation creates unreachable, microscopic drug reservoirs, allowing for controlled release while enhancing the skin's absorption capabilities. This approach provides a promising solution for delivering a wide range of therapeutic agents.[45]
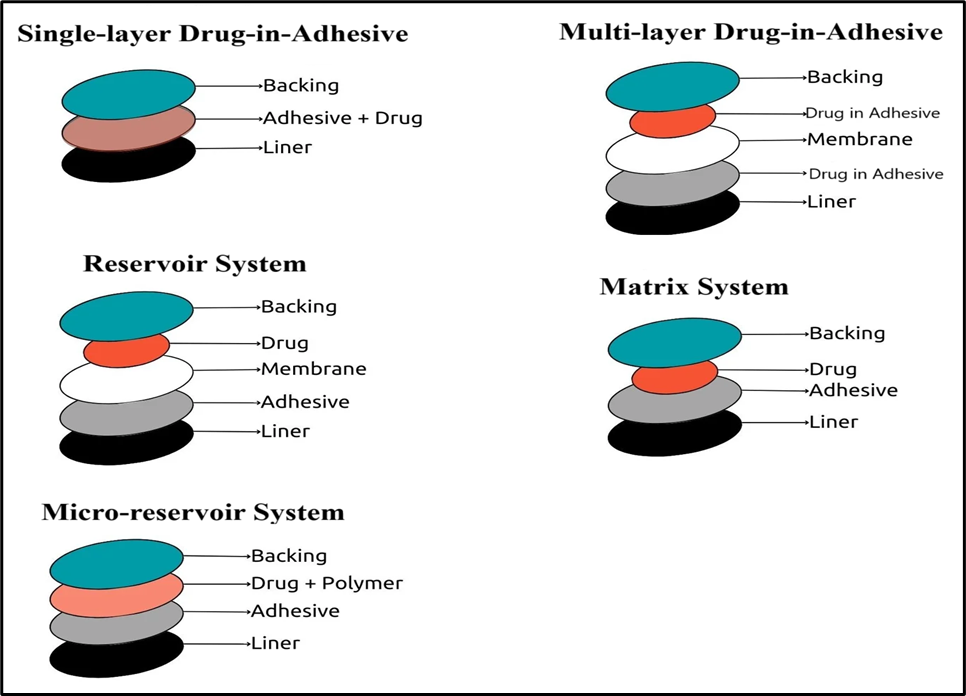
Figure 3: Types of Transdermal Patches.
Skin irritation is a common issue with TDDS, presenting symptoms such as redness, itching, and burning.
Allergic responses can occur due to components in the patch, including adhesives and active ingredients. Symptoms may range from localized rashes to more widespread hives, often requiring the patch to be removed.
The continuous delivery of medications, particularly potent opioids like fentanyl, raises concerns about systemic overdose. Signs of overdose can include nausea, vomiting, sedation, and serious respiratory issues.
Drug absorption through the skin varies due to factors like skin thickness, hydration, and temperature. This variability can lead to inconsistent therapeutic.
Table No. 1: List of Drugs Used in Transdermal Patches: Pharmacological Category, Formulation Type, and Clinical Applications
|
Sr. No. |
Drug |
Pharmacological Category |
Formulation Type |
Clinical Application |
|
1 |
Nicotine |
Smoking cessation agent |
Matrix Patch |
Smoking cessation |
|
2 |
Fentanyl |
Opioid analgesic |
Reservoir Patch |
Pain management |
|
3 |
Hormones (e.g., Estradiol) |
Hormone |
Matrix or Reservoir Patch |
Hormone replacement therapy |
|
4 |
Scopolamine |
Anticholinergic |
Matrix Patch |
Motion sickness |
|
5 |
Clonidine |
Alpha-2 adrenergic agonist |
Matrix Patch |
Hypertension treatment |
|
6 |
Nitroglycerin |
Nitrate vasodilator |
Reservoir Patch |
Angina pectoris |
|
7 |
Testosterone |
Androgen |
Matrix Patch |
Hormone replacement therapy |
|
8 |
Rivastigmine |
Acetylcholinesterase inhibitor |
Reservoir Patch |
Alzheimer's disease |
|
9 |
Capsaicin |
Analgesic (topical) |
Matrix Patch |
Pain relief (topical) |
|
10 |
Lidocaine |
Local anesthetic |
Matrix Patch |
Local anesthesia |
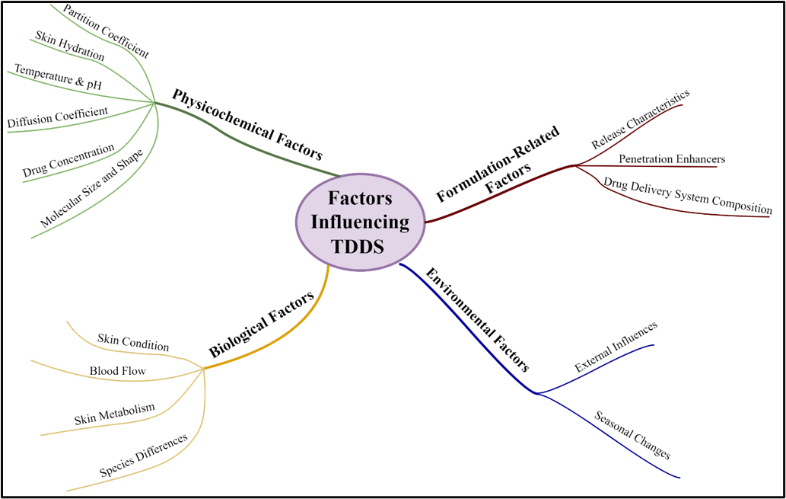
Figure 4: Factors Influencing TDDS.
The drug used in transdermal systems is often selected for its ability to bypass first-pass metabolism and its compatibility with transdermal delivery requirements. Ideal properties include a molecular weight of less than 500 Da, an affinity for both hydrophobic and hydrophilic phases, a low melting point, and non-irritating, and non-allergic characteristics. The drug's log partition coefficient should be between 1 and 4, with a solubility greater than 1 mg/mL within a pH range of 5.0 to 9.0.[65]
Pressure-sensitive adhesives (PSAs) are critical for maintaining close contact between the patch and the skin. They must be easily attachable and removable without causing irritation. The adhesive should not interfere with drug permeation and must be compatible with other components.[66]
The polymer matrix regulates drug release and can be prepared by dispersing the drug in a synthetic polymer. Polymers should be biocompatible, chemically compatible with the drug, and maintain consistent drug delivery throughout the shelf life. Common polymers include natural options (e.g., cellulose derivatives) and synthetic elastomers (e.g., polybutadiene). [67]
Backing films provide stability, protect the active layer, and regulate skin permeation. They must be chemically resistant and compatible with excipients to prevent leaching. Ideal materials include flexible, impermeable substances like vinyl, polyethylene, and polyester.[68]
This protective layer is removed before patch application. It must be chemically inert and allow permeation of the drug and enhancers while preventing moisture ingress.[71]
Penetration enhancers, or permeation enhancers, are substances that enhance the penetration of active compounds through the skin by temporarily altering the stratum corneum. This enhancement allows for improved delivery of topical medications into the bloodstream.[72]
Drug penetration through the skin involves several pathways, including:
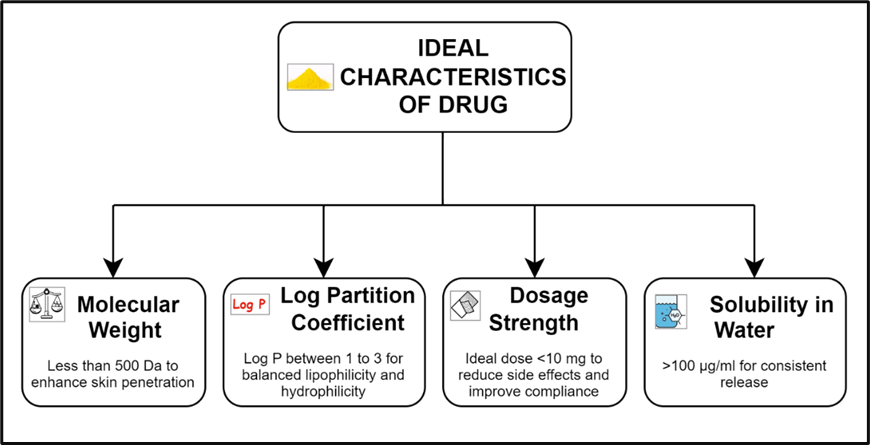
Figure 5: Ideal Characteristics of Drug
Table No. 2: Ideal Properties of Drug
|
Parameter |
Properties |
|
Dose |
Less than 20 mg/day |
|
Molecular weight |
Less than 1000 Dalton |
|
Melting point |
Less than 200°C |
|
Half-life |
Less than 10 hours |
|
Shelf life |
Up to 2 years |
|
Partition coefficient |
1 to 4 |
|
Aqueous solubility |
Greater than 1mg/mL |
|
pH of the aqueous saturated solution |
5-9 |
|
Skin permeability coefficient |
Greater than 0.5×10-3cm/h |
|
Skin reaction |
Non-irritating and non-sensitizing |
|
Oral bioavailability |
Low |
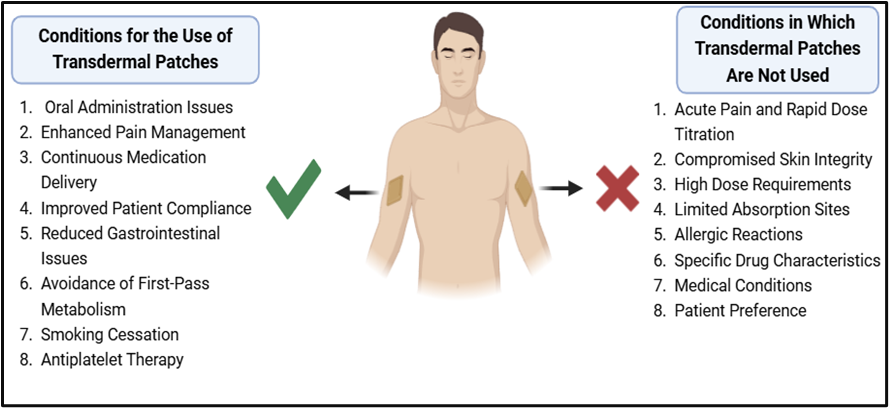
Figure 6: Clinical Conditions Supporting and Limiting Transdermal Patch Utilization
This method involves fabricating a prototype patch using a heat-sealable polyester film (type 1009, 3M) with a 1 cm diameter concave as the backing membrane. A drug sample is dispensed into this concave, covered with a TPX poly (4-methyl-1-pentene) asymmetric membrane, and sealed using an adhesive. The TPX membrane is prepared through a dry/wet inversion process, where TPX is dissolved in a solvent mixture at 60°C, followed by casting on a glass plate and coagulating in a bath maintained at 25°C.[78]
In this approach, polymer solutions in various ratios are dissolved in an organic solvent. A calculated amount of drug is dissolved in half of the solvent, while enhancers are dissolved in the other half. Di-N-butyl phthalate is added as a plasticizer to the drug-polymer solution. The combined mixture is stirred for 12 hours and then poured into a circular Teflon mold. These molds are placed on a leveled surface and covered with an inverted funnel to control solvent vaporization in a laminar flow hood at an air speed of 0.5 m/s. After allowing the solvent to evaporate for 24 hours, the dried films are stored in a desiccator containing silica gel for an additional 24 hours to eliminate aging effects. [79]
In this method, the drug is dissolved in a polymer solution that includes a plasticizer. This mixture is stirred for 10-15 minutes to achieve a homogeneous dispersion, which is then poured onto a levelled mercury surface. An inverted funnel is used to control solvent evaporation, allowing for efficient film formation.[80]
The drug is dispersed in a mixture of water and propylene glycol containing Carbomer 940 polymer and stirred for 12 hours using a magnetic stirrer. The dispersion is neutralized with triethanolamine to enhance viscosity. A buffer with a pH of 7.4 can be used to achieve a gel-like consistency, particularly when drug solubility in aqueous solutions is poor. This gel is subsequently incorporated into the IPM membrane.[81]
To create a transdermal therapeutic system, a 1% Carbopol reservoir gel, polyethylene (PE), and ethylene vinyl acetate copolymer (EVAC) membranes serve as rate control membranes. For drugs insoluble in water, propylene glycol is used to prepare the gel. The drug is dissolved in propylene glycol, mixed with Carbopol resin, and neutralized with a 5% w/w sodium hydroxide solution. The drug in gel form is then placed on a backing layer and covered with a rate-controlling membrane, with edges sealed by heat to form a leak-proof device. [82]
This method is particularly suitable for drugs with a loading dose greater than 10 mg, as it helps avoid unstable matrices. Chloroform is the solvent of choice, dissolving both the drug and adhesive. The drug is combined with the adhesive material in chloroform, and a custom-made aluminum former is lined with aluminum foil and sealed with cork blocks.
Proliposomes are prepared via the carrier method using a film deposition technique. An optimized ratio of drug and lecithin (0.1:2.0) is employed. Mannitol powder (5 mg) is placed in a round-bottom flask, heated to 60-70°C, and dried under vacuum for 30 minutes. The drug and lecithin are dissolved in an organic solvent mixture. Aliquots of this solution are introduced into the flask, and following complete drying, the proliposomes are lyophilized, stored in a desiccator, and sieved through a 100-mesh screen. [83]
This method involves casting a free film of cellulose acetate on a mercury surface. A 2% w/w polymer solution is prepared using chloroform, with plasticizers incorporated at 40% w/w of the polymer weight. The polymer solution is poured into a glass ring on the mercury surface, and the solvent evaporation is controlled by an inverted funnel. After complete evaporation, the dry film is separated and stored in a desiccator between sheets of wax paper. [84]
The preparation of TDDS is modified from earlier reported methods using a solvent casting approach. A polymer (e.g., PVP/HPMC) is mixed with a minimum quantity of solvent, followed by the addition of other polymers (e.g., PVA) and thorough stirring. A plasticizer is incorporated, and the drug is added with continuous agitation. The resultant films are cast onto a glass mold and dried in an oven at 40°C. After drying, the films are carefully removed, wrapped in butter paper, and stored in a cool, light-protected environment.
Each patch undergoes visual inspection for color, clarity, transparency, flexibility, and surface smoothness, all crucial for product uniformity and quality assurance.[85]
To ensure excipient compatibility with the drug, analytical methods like thermal analysis, Fourier-transform infrared (FT-IR) spectroscopy, UV spectroscopy, and chromatography are employed. These helps detect possible physical or chemical interactions, thus preserving the drug’s stability and bioavailability.[86]
Measured at multiple points using a micrometer, uniform patch thickness ensures consistent drug release and dosage. [87]
A strip of the patch is repeatedly folded up to 300 times until it breaks, measuring its flexibility a key property for body movement adaptability.[88]
After drying, patches are weighed to confirm uniform drug distribution. Variability should remain within acceptable limits, ensuring dose consistency. [89]
Moisture content and absorption are evaluated by exposing patches to controlled humidity levels. Moisture content is determined by placing patches in a desiccator, while uptake is assessed by re-weighing patches exposed to high humidity. [90]
%Moisture Content= Initial Weight-Final WeightInitial Weight×100

Patches are sealed over vials containing calcium chloride and kept at 63% relative humidity. Weight changes after 72 hours assess the patch’s permeability to moisture, essential for product stability.[91]
WVP= ?WA?t
Were,
To ensure accurate drug loading, patches are dissolved in solvents (e.g., methanol or phosphate buffer) and analyzed via UV or HPLC techniques.[92]
Polariscopic microscopy determines whether the drug remains crystalline or transforms to an amorphous form in the patch, impacting stability and release profile.[93]
Flatness is assessed by measuring strips from different patch areas. Zero constriction indicates uniform flatness, a quality essential for even adhesion to the skin. [94]
This test, often performed with a universal testing machine, measures the force required to break the patch, indicating its durability and mechanical strength. [95]
Measures the time a patch holds under a specific weight on a smooth surface, indicating adhesive strength.
The force to remove a patch from a steel surface at a 180-degree angle, testing adhesive durability.
Measures the distance a steel ball travels on the adhesive surface, indicating quick adhesion.
These tests measure the ease of separating a thumb or probe from the adhesive, providing tack values crucial for user application.
A probe contacts the adhesive surface; the force to separate the probe is recorded as tack, reflecting quick adherence. [96]
Using a USP dissolution apparatus, patches are tested in a buffer at body temperature, and drug release is measured over 24 hours. This ensures controlled and sustained drug delivery.
Patches are stored at high temperatures and humidity according to ICH guidelines, with periodic assessments over six months to verify long-term stability. [97]
In vitro permeation studies evaluate drug release and absorption through the skin, providing an initial indication of the formulation’s in vivo behavior.[98], [99]
Typically employing Franz or flow-through diffusion cells, these studies simulate the permeation environment with a donor compartment (holding the patch) and a receptor compartment (buffer solution) with constant stirring to ensure uniform drug distribution.
Skin from animals (e.g., rats or pigs) or synthetic membranes with properties mimicking human skin are commonly used, with the epidermal side facing the patch to simulate skin application.
The system is maintained at 32°C to replicate human skin temperature, with samples collected periodically from the receptor compartment over 24 hours for analysis.
Samples are analyzed via UV spectrophotometry or HPLC to determine cumulative drug release, permeation rate, and permeability coefficient. Flux is calculated from the steady-state slope of drug permeation versus time.[100]
In vivo studies assess the TDDS’s actual performance within a living system, considering absorption, metabolism, and excretion.
Before human trials, animal models (e.g., hairless mice, rats, or rabbits) provide initial pharmacokinetic and pharmacodynamic data. The TDDS is applied to the skin, and blood or tissue samples are collected at intervals to study bioavailability and absorption rates.[101]
In clinical trials, patches are applied to human subjects, measuring pharmacokinetics, safety, and efficacy. Plasma drug levels indicate how efficiently the drug enters systemic circulation, with side effects and compliance closely monitored.
Human studies provide unique insights into individual variations in drug absorption and metabolism. These results inform therapeutic effectiveness, dosing, and action duration.
Clinical trials validate that the TDDS can achieve therapeutic drug levels with minimized side effects, often using crossover studies to compare the transdermal route’s advantages over alternative administration forms.[102]
Table No. 3: Evaluation Methods with United States Pharmacopeia (USP) Limits for Patches.
|
Sr. No. |
Evaluation Method |
United States Pharmacopeia Limits |
|
|
Physical Appearance |
Clear, no discolouration; flexible, smooth |
|
|
Interaction Studies |
No detectable interaction impacting drug bioavailability |
|
|
Thickness Measurement |
±10% variation in thickness |
|
|
Folding Endurance |
Minimum 100 folds, ideal 300 |
|
|
Weight Uniformity |
±5% weight variation |
|
|
Moisture Content and Uptake |
Moisture content ≤5%, uptake ≤10% |
|
|
Water Vapor Permeation (WVP) Test |
WVP ≤0.05 g/24 hrs./cm² at 63% RH |
|
|
Drug Content Analysis |
90-110% of labelled drug content |
|
|
Polariscopic Examination |
No crystalline content if amorphous form is intended |
|
|
Flatness Test |
Maximum variation ≤1 mm |
|
|
Tensile Strength |
Tensile strength ≥5 N/cm² |
|
|
Adhesion and Tack Tests |
|
|
≥50 g/cm² |
|
|
≥100 g/cm² at 180° angle |
|
|
<2 cm |
|
|
Easy separation of tack |
|
|
Reflects quick adherence |
|
|
|
In Vitro Release Study |
≥80% release within 24 hours |
|
|
Stability Studies |
≤5% degradation at 40°C, 75% RH after 6 months |
|
|
In Vitro Permeation Studies |
≥50% drug release within 24 hours |
|
|
In Vivo Studies |
≥80% bioavailability within 24 hours |
Transdermal drug delivery systems (TDDS) have gained prominence due to their ability to facilitate effective medication administration while minimizing invasive procedures. Several innovative technologies have emerged, each with unique mechanisms and applications.
Thermal ablation, also known as thermophoresis, utilizes targeted heat to disrupt the stratum corneum, thereby creating microchannels that enhance drug permeability. Achieving temperatures above 100 °C is crucial for vaporizing keratin and altering the skin's structure.[103] This technique can be executed using various thermal energy sources, such as lasers and radiofrequency devices. By carefully adjusting parameters like wavelength and exposure duration, practitioners can control the depth and extent of skin ablation, significantly improving drug delivery efficiency.[104], [105]
Microneedle technology represents a groundbreaking method in transdermal delivery, employing micron-sized needles to penetrate the skin's outer layer. These needles, typically measuring 25 to 2000 μm in height, allow for the direct administration of medications into the dermal capillaries, thus enhancing absorption while reducing pain. The success of this approach hinges on optimizing the geometry of microneedles to ensure they reach the target without contacting nerve endings. They are generally arranged in arrays to maximize skin contact and drug delivery.[106], [107], [108]
Needle-free jet injectors propel liquid formulations through narrow nozzles, ranging from 50 to 360 μm in diameter.[109] This method eliminates concerns associated with needle disposal and injury, although risks of cross-contamination from the nozzle remain. Solid jet injectors utilize compressed gas to deliver powdered medications, creating Micro perforation in the skin that facilitate drug absorption. Key factors influencing drug distribution include particle size and impact velocity, which are critical for achieving effective delivery of specific therapeutics.[51], [110]
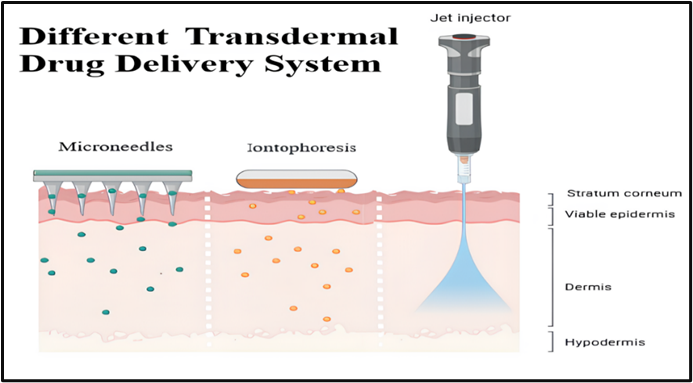
Figure 7: Different Transdermal Drug Delivery System
Recent innovations in transdermal patch technology are transforming how medications are delivered, enhancing both patient comfort and treatment efficacy. Here are some notable advancements in this field:
New patches are now capable of delivering protein-based therapies effectively. This is particularly important since proteins are often too large to penetrate the skin easily.[111] By improving the technology behind these patches, researchers are making it possible to treat various conditions with protein drugs that were previously difficult to administer.[112]
Transdermal patches are being developed for continuous glucose monitoring, offering a pain-free alternative for those managing diabetes.[113] These patches allow for real-time data collection without the need for finger pricks, making diabetes management more comfortable and less invasive. [114], [115]
A groundbreaking testosterone transdermal patch has been created for young women experiencing spontaneous premature ovarian failure.[116] This non-invasive approach provides a reliable method for hormone replacement therapy, helping to improve the quality of life while minimizing potential side effects often associated with oral medications. [117]
Transdermal patches containing Oxybutynin are now being used to treat overactive bladder (OAB). [118] These patches deliver a consistent dose of medication, which simplifies the treatment regimen and helps improve adherence by reducing the frequency of doses needed throughout the day. [119], [120]
Numerous patents have been granted to researchers in the field of Transdermal Drug Delivery Systems (TDDS) due to their clinical utility. The table below presents a selection of significant patents.
|
Sr. No. |
Patent Number |
Title |
Inventor |
Key Innovation |
Year |
Reference |
|
|
US3598122A |
Bandage for administering drugs |
Alejandro Zaffaroni |
First transdermal patch system with a drug reservoir and semi-permeable membrane for controlled delivery |
1971 |
[121] |
|
|
US-4668232-A |
Transdermal drug patches
|
Ginter Cordes, Michael Wolff |
Pioneering work on drug patches, including adhesives and drug formulations for enhanced drug delivery. |
1987 |
[122] |
|
|
US4839174A
|
Novel transdermal nicotine patch |
Richard W. Baker, Frank Kochinke, Carl Huang |
Transdermal nicotine patch for smoking cessation therapy. |
1989 |
[123] |
|
|
US 5008110A |
Storage-Stable Transdermal Patch |
Arnold G. Benecke, Daniel J. Kinne, Andrew J. Wnuk |
Development of a storage-stable transdermal patch, addressing stability issues and ensuring consistent drug delivery. |
1991 |
[124] |
|
|
US-5232702-A |
Silicone pressure sensitive adhesive compositons for transdermal drug delivery devices and related medical devices |
William R. Pfister, Jeniffer M. Wilson |
Innovative silicone-based adhesives designed for use in transdermal patches and medical devices. |
1993 |
[125] |
|
|
US5262165A |
Transdermal Nitroglycerin patch with penetration enhancers |
Sharad K. Govil, Edward M. Rudnic, Dale G. Sterner |
Transdermal patch for nitroglycerin, using penetration enhancers for improved drug absorption |
1993 |
[126] |
|
|
US-5290561-A |
Single layer transdermal drug administration system |
Bahram Farhadieh, Rajeev D. Gokhale |
Simplified single-layer patch design for efficient drug delivery and reduced production complexity. |
1994 |
[127] |
|
|
US-5486362-A |
Controlled, sustained release delivery system for treating drug dependency
|
Judith P. Kitchell, Indu A. Muni, Yvonne N. Boyer |
Sustained-release system for drug dependency treatment with controlled release mechanisms. |
1996 |
[128] |
|
|
US-5703101-A |
Agonist-antagonist combination to reduce the use of nicotine and other drugs
|
Jed E. Rose, Edward D. Levin |
Innovative combination of agonists and antagonists for drug addiction and smoking cessation therapy. |
1997 |
[129] |
|
|
US-5721257-A |
Method and therapeutic system for smoking cessation
|
Richard W. Baker, Giancarlo Santus, Susan Vintilla-Friedman |
Advanced system focusing on effective smoking cessation strategies. |
1998 |
[130] |
|
|
US5869090A
|
Transdermal delivery of dehydroepiandrosterone |
Jerry Rosenbaum |
Development of a TDDS for dehydroepiandrosterone (DHEA), a hormone with potential therapeutic uses. |
1999 |
[131] |
|
|
US-5948433-A |
Transdermal patch
|
Scott Allison Burton, Shahnaz Tata |
Transdermal patch design with improved adhesive and drug stabilization properties. |
1999 |
[132] |
|
|
US-7642232-B2 |
Compositions and methods for the prevention and control of insulin-induced hypoglycemia |
Daniel T. Green, Robert R. Henry |
Systems to prevent hypoglycemia caused by insulin treatment through innovative transdermal delivery. |
2010 |
[133] |
|
|
US8197844-B2 |
Active electrode for transdermal medicament administration |
Jamal S. Yanaki |
Active electrode design enhancing the precision of transdermal drug delivery. |
2012 |
[134] |
|
|
US-8641689-B2 |
Transdermal porator and patch system and method for using same |
Bernadette Messier, Zoran Novakovic, Jeremiah Peter O'Leary |
Integration of porators with patches to improve the efficiency of drug absorption. |
2014 |
[135] |
|
|
US-9056061-B2 |
Transdermal nicotine salt delivery system |
Robert M. Gale, Jay Audett, Rama V. Padmanabhan |
Advanced nicotine salt delivery system improving stability and absorption. |
2015 |
[136] |
|
|
US-10556106-B2 |
System and method for biphasic transdermal iontophoretic delivery of therapeutic agents for the control of addictive cravings
|
Mir A. Imran, Talat Imran, Mir Hashim |
Innovative biphasic iontophoretic delivery system for addressing addictive cravings. |
2020 |
[137] |
|
|
US-11129975-B2 |
Transdermal delivery of high viscosity bioactive agents |
Russell F. Ross |
Method for transdermal administration of bioactive agents with high viscosity. |
2021 |
[138] |
|
|
CA-2955247-C |
Abuse deterrent opiod/opiod-antagonist transdermal patch
|
Audra Lynn Stinchcomb, Dana Carmel Hammell, Stan Lee Banks, Josh ELDRIDGE, Miroslaw Jerzy Golinski |
Abuse-deterrent patch combining opioids and antagonists to prevent misuse and ensure controlled release. |
2023 |
[139] |
|
|
US11648214-B2 |
Systems and methods for long term transdermal administration |
Eun Soo Lee, Amit K. Jain, Parminder Singh |
Systems enabling sustained and long-term drug administration through transdermal patches |
2023 |
[140]
|
|
|
US11911522-B2 |
Process for the continuous manufacture of a polyisobutylene based transdermal patch |
Russell Adam Baird, Brad L. Barnett, Russell D. Beste |
Continuous production process for polyisobutylene-based transdermal systems ensuring scalability. |
2024 |
[141] |
|
|
US-11938160-B2 |
Pharmaceutical composition and method of manufacturing |
Gary J. Speier |
Improved composition and manufacturing methods for advanced transdermal patches. |
2024 |
[142] |
19. Future Innovations in Transdermal Drug Delivery Technologies
The future of transdermal drug delivery systems (TDDS) is promising, with advancements aimed at overcoming traditional challenges like low drug solubility and skin permeability.[143] New formulation techniques, such as liposomes and microemulsions, are improving the delivery of poorly soluble drugs. Innovations in patch design are expected to boost the popularity of transdermal analgesics, while technologies that leverage mechanical energy, like iontophoresis, electroporation, sonophoresis, and thermal energy, are enhancing drug delivery by modifying the skin barrier or boosting drug molecule energy.[144]
The TDDS market is growing rapidly, projected to reach $2 billion, with a 25% annual growth rate. Microneedle technology, such as the NanoPatch®, is showing promise for single-dose vaccine delivery.[145] Advances like thermal poration, jet injectors, and micro-infusion systems are further improving drug delivery efficiency. Companies like Trans Pharma and Altea Therapeutics are developing products to enhance patient compliance, focusing on sustained-release formulations and innovative vaccination methods. [146]
20. Challenges
Transdermal drug delivery systems (TDDS) face numerous challenges that can impact their effectiveness and acceptance by patients. A primary concern is the skin's natural barrier function, particularly the stratum corneum, which restricts the absorption of larger molecules and hydrophilic drugs.[147] This limitation narrows the scope of medications suitable for transdermal application, often leaving out vital treatments. Moreover, variations in skin properties among individuals such as thickness, temperature, and hydration can lead to unpredictable absorption rates, complicating dosing and therapeutic outcomes.[148]
Formulation stability is another pressing issue; many active ingredients can degrade due to environmental factors like light and humidity, leading to a potential loss of efficacy over time. [149] Additionally, patient compliance can suffer due to skin irritation or allergic reactions from adhesives or drug compounds, making it difficult to ensure consistent usage.[150] The regulatory environment further complicates the landscape, as manufacturers must navigate rigorous approval processes that require comprehensive safety and efficacy data. These multifaceted challenges underscore the need for ongoing research and innovation to improve the design and functionality of TDDS, ultimately enhancing patient outcomes and acceptance.[151], [152], [153], [154]
Transdermal drug delivery systems are one of the significant advances in modern medicine, being a patient-friendly and efficient alternative to the traditional drug delivery methods. The review discusses the evolution, mechanisms, types, and applications of TDDS with advantages and limitations. This also includes complex issues on skin permeability, formulation strategies, and advanced technologies, which might make TDDS a possible revolution in pharmacotherapy. Despite these challenges, which include adverse effects, continuous innovation and research may be able to overcome them. TDDS represents the best example of science and technology fusion into the creation of more efficient and convenient drug delivery.
ABBREVIATIONS
FUNDING:
This Review Article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
DECLARATION OF COMPETING INTEREST
The authors have no competing interests to declare that are relevant to the content of this article.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All the data was available from public databases and there was no need for ethics approval and consent.
REFERENCES


Rohan Mane, Rukayya Shaikh, Priyanka Paulzagade, A Review on Transdermal Drug Delivery Systems: Transdermal Patches, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1401-1432. https://doi.org/10.5281/zenodo.18245538
 10.5281/zenodo.18245538
10.5281/zenodo.18245538
