Chhatrapati Shivaji College of Pharmacy, Deori, Gondia, Maharashtra, India
One reason treatments differ so much? People are not identical. Standard methods can miss the mark, sometimes causing harm instead of help. Since the early 2000s, tools like gene mapping, protein analysis, and smart algorithms began shifting the landscape. Because of these, care now adjusts to DNA, body signals, daily habits, even surroundings. Diagnosis got sharper, medication choices wiser, bad reactions less common - this shift didn’t stay in labs. Fields from cancer to heart health started using it. Nowhere near every hospital uses new methods, even though results in cancer care show better survival rates when treatment matches the person. One reason is fear about who gets to see DNA details, another is price tags too high for most clinics. Some groups barely appear in studies, which skews how well fixes work across communities. Getting these tools into daily checkups feels like pushing uphill - doctors lack support, systems resist change. Progress hinges on doctors talking with lab experts, software builders, and rule makers more often than before. When machines learn patterns from wider pools of people, smarter choices could follow - for real this time. Out in the void of space, new uses might just begin to take shape. When guided by care and clear moral direction, tailored medical approaches could actually get nearer to helping people everywhere receive treatment that works better, causes less harm, and feels more fair.
Personalized medicine, sometimes called precision care, tries to fit treatments to a person's specific biology [1]. Instead of one-size-fits-all methods built on average results from large groups, this approach recognizes that people react differently - to meds, illnesses, or therapies. Thanks to progress in gene research, computing power, and lab testing, custom healthcare plans are now more doable than ever before [2] .
At first, experts saw genetics as key to personalizing healthcare. Instead of guessing, Abrahams and Silver believed DNA data could guide smarter treatment choices - matching patients with effective therapies when it mattered most [1] . Meanwhile, Ginsburg and Willard pointed out new methods popping up that put genetic science front and center in changing how doctors care for people [2] .
The world of tailored medical care’s grown fast over time. Right now, it includes gene-based drug response analysis, protein studies, treatments guided by biological markers, smart tech helping plan care, also wide-scale methods aiming at precise community health efforts [4–8,26]. This article pulls together findings from many fields to look at how custom healthcare is changing lab science, doctor routines, along with rules guiding medicine delivery.
2. Historical Evolution of Personalized Medicine
The idea behind tailored healthcare goes way back. Even when tech was basic, some writers saw that one-size-fits-all treatments missed personal differences. Back in '71, Gibson wondered if healing could move past rigid norms to fit each person [18]. That doubt sparked future breakthroughs.
A big step happened in the early 2000s thanks to the Human Genome Project. Thanks to new tools like pharmacoproteomics and pharmacogenomics, researchers started looking at how people react differently to drugs - how they process them, side effects, or if they even work [4]. Not long after, key voices began pushing for changes in how medicines are made and care is given, so these genetic advances could actually be used [1,29].
Collins, along with Hamburg, called precision medicine a way to upgrade how doctors treat patients and develop treatments - highlighting the role of genetic testing in everyday healthcare [22]. In the following ten years, it shifted from an idea on paper to real-world use in various medical fields.
3. Foundations of Personalized Medicine
3.1 Genomics as the Central Pillar
Genomic studies are key to custom medicine approaches. Differences in genes - like SNPs, CNVs, or passed-down changes - affect how likely someone is to get sick or react to meds [2,28]. Fast DNA scanning tools now make it possible to map genomes widely, so doctors can spot useful gene shifts but also adjust therapy based on that info.
Offit broke down how old-school genetics still plays a role in today’s gene-based medical choices [33]. Instead of broad guesses, doctors now use DNA clues to tell apart illness types, get better outcome forecasts, or pick precise treatments [34].
3.2 Proteomics and Biomarkers
Proteomics adds to genomics, showing how proteins change and affect how drugs work inside the body. Jain pointed out that studying drug-related proteins helps tailor medicines better and improve how treatments are used [4].
Biomarkers help tailor treatments by spotting diseases, showing how serious they are, also pointing to where meds should act. Drugan with Leucu?a stressed checking new markers carefully - this boosts diagnosis precision while making care fit each person better [12].
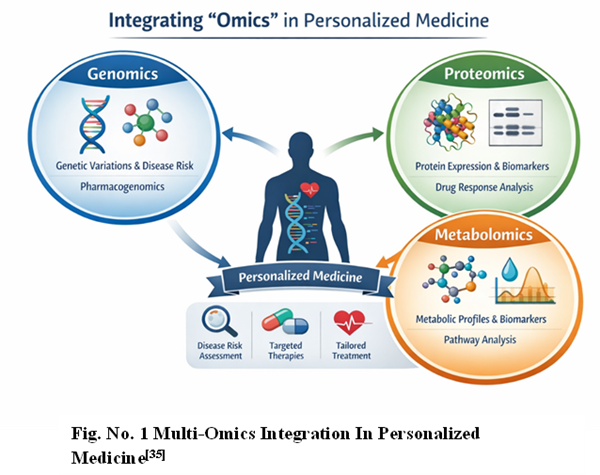
3.3 Systems Biology and Multi-Omics Integration
Today’s tailored medical care uses a broad biological view, mixing gene info, RNA patterns, protein levels, metabolic signals, plus patient records. According to Mathur and Sutton, combining these elements might completely change medicine - boosting how we foresee illness, stop it before it starts, or adjust treatments to each person [9].
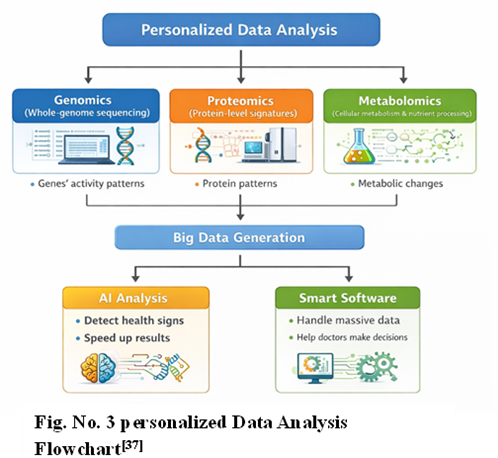
4. Emerging Role of Artificial Intelligence in Personalized Medicine
AI’s growth boosted how we tailor medical care. Because of machine learning, systems now study detailed biological data, spot likely results from treatments, also create custom plans for patients [3,8].
Schork explained that AI helps grasp differences among patients better, also guiding tailored approaches in treating cancer [3]. In the same way, Parekh’s team showed how smart systems can build custom treatment ideas from DNA and health records - boosting real-world medical choices [8].
New breakthroughs in AI for finding and giving medicines have sped things up. Serrano's team showed how AI helps craft precise drugs tailored to individuals [32].
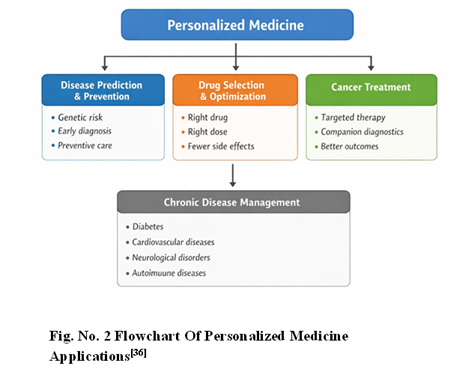
5. Applications of Personalized Medicine
5.1 Oncology
Oncology’s still ahead when it comes to using customized treatments. Because of genetic testing, cancer drugs now work way better than before. Gambardella's team showed how far we’ve come in adjusting therapies - lives are longer, side effects fewer [10]. Building on that, Hoeben's group highlighted steady gains in matching meds to DNA data [11].
Latest work on colon cancer shows new chances but also hurdles when dealing with varied tumor cells and treatments aimed at individual patients [30].
5.2 Psychiatry
Personalized care in mental health tries to improve diagnosis and therapy by combining genetics, brain science, and life experiences. Instead of cancer, which uses clear biological signs, psychiatry struggles because conditions come from many causes. Ozomaro’s team pointed out the potential but also the hurdles in tailoring treatment for mental illnesses - symptoms differ a lot between people, plus proof for reliable markers is still weak [6].
Thanks to new brain-gene research, scientists can now spot DNA differences that affect how people react to mood and mental health meds. On top of that, smart computer systems help guess which patients won't respond well to standard treatments or figure out better mixtures of drugs. Even so, big hurdles stick around - like shaky biological signals, weak forecast accuracy, plus a shortage of broad, real-world patient info.
5.3 cardiovascular diseases
The use of tailored treatments in heart health has been rising slowly. Because of work by Lee and team, we now know gene data along with detailed scans or biological markers help forecast risks better - also guide treatment choices for heart issues [17]. When it comes to problems like inherited high cholesterol, blood pressure disorders, or irregular heartbeats, custom approaches make a real difference.
Savoia et al. showed that custom strategies for treating high blood pressure - like pinpointing key molecular signals tied to the condition - help shape personalized drug plans [24]. Because of genomic findings, doctors can better pick patients who might benefit from newer treatments, such as PCSK9 blockers, medicines that prevent clotting, or drugs that thin the blood.
5.4 Respiratory Diseases
Personalized medicine might really help people dealing with long-term breathing issues like COPD. Franssen’s team looked into tailored treatments using factors like inflammation types, genes, or what surroundings a person faces [20].
COPD looks different in every person - how fast it worsens, how often flare-ups happen, and what meds work best. Things like eosinophil levels or protein patterns might help pick the right treatment, maybe inhalers with steroids or newer targeted drugs. Still, fitting routine biomarker checks into day-to-day clinic routines isn’t easy.
5.5 Infectious Diseases and Antibiotic Therapy
In treating infections, tailored medical approaches help pick the right drug, dose, and how long to use it. Moser’s team explained that things like a person’s immunity, gut bacteria mix, or body chemistry can change how well antibiotics work [7].
AI tools now guess which germs resist drugs, helping doctors pick better treatments early. Instead of waiting for lab tests, care can start smarter. Tailored antibiotic use might slow down resistance while lowering side effects. This approach could save more lives - particularly among people with weak immune systems.
6. Personalized Medicine in Public Health
6.1 Population-Level Precision Medicine
Though tailored treatments usually focus on single patients, wider community-focused methods matter just as much. Khoury and team pointed out that blending targeted techniques with large-scale health systems might boost prevention efforts while narrowing gaps in care among varied groups [26].
Population-wide tailored healthcare means:
6.2 Human Genetic Diversity and Global Health
Globally, personalized medicine needs to reflect how gene patterns differ across groups. Because genetic variety shapes who gets sick or responds to drugs, Lu and team pointed out - making custom DNA libraries plus broad-based studies essential [28].
Failing to tackle differences in genes might boost gaps in world health care. Because scientists want better results everywhere, they’re now adding more ethnic groups into DNA records.
7. Personalized Medicine in Space and Extreme Environments
Personalized medicine isn't just for people on Earth. In space, astronauts face weird body changes - like low gravity, radiation, messed-up sleep cycles, also weakened immunity. Pavez Loriè's team checked if smart health tech could help tailor fixes for each astronaut on long trips [14].
Key applications include:
8. Drug Repositioning and Personalized Therapeutics
Drug repositioning means using old medicines for new health problems - it’s become a handy method in tailored treatments. Li and Jones found it works well to spot custom cures, particularly when dealing with uncommon or tough-to-treat illnesses [15].
Genomic or proteomic methods can spot fresh biological pathways where existing meds might work, speeding things up yet spending less. Machine learning boosts this even more - finding unexpected links between medicines and illnesses inside huge piles of data.9. Advances in Personalized Cancer Therapy Cancer’s pushed big changes in custom healthcare. Thanks to gene analysis, precise treatments, or better testing, patients now do much better.
9.1 Molecular Profiling and Targeted Therapy
Finding specific gene changes lets doctors pick treatments more accurately than before. With insights from Gambardella’s team, today's cancer care uses DNA clues - not just to choose drugs, but also to guess how well they’ll work or when adjustments are needed [10].
Important parts inside cells that drugs aim for are:
9.2 Immunotherapy and Personalized Biomarkers
Immunotherapy now plays a key role in tailored cancer treatment. Things like PD-L1 levels, how many mutations a tumor has, or signs of microsatellite issues help pick the right checkpoint drugs. Instead of guessing, doctors use these clues to choose therapy. Each marker gives a hint about which drug might work best.
Hoeven's team pointed out that custom immune treatments - one shaped by how aggressive a tumor is and its DNA makeup - are changing how doctors fight cancer [11]. On top of that, made-to-fit vaccines targeting new tumor markers or engineered T-cells show major progress aimed right at each person’s unique cancer traits.
9.3 Personalized Treatment of Colon Cancer
Colon cancer shows how tough it is to tailor treatment to each person. Dey’s team shared new progress - like sorting tumors by genes, custom chemo setups, also blending different data types to map illness traits [30].
Fighting colon cancer differently for each person is tough because tumors change a lot, spread in different ways, or stop responding over time. Even so, smart computer systems are getting better fast at guessing how well drugs might work.
10. Biomarker discovery and validation
What makes care fit a person? Biomarkers do that job. They show differences in how bodies work, so doctors can pick treatments for one person instead of guessing from group averages. Spotting illness earlier, judging its path, choosing drugs - biomarkers help at each step. Without solid proof they measure what they claim, day after day, across different labs and patients, their value falls apart. Real results matter most. Trust comes only when testing holds up outside theory.
Not every patient reacts the same way to medicine - some clues lie in predictive markers that point to who might respond best to certain drugs, helping doctors choose wisely while reducing unwanted reactions. Disease outlooks can be clearer through prognostic signs that hint at how illness may unfold regardless of therapy, shaping decisions about monitoring and follow-up. Spotting trouble before it shows up physically is possible thanks to diagnostic signals caught during routine checks or screenings. When treatment begins, pharmacodynamic indicators shift in response, revealing whether a drug hits its mark inside the body. Each type plays a role - not always loud, but steady - in guiding choices tailored to one person at a time [21,22].
Nowhere is progress more clear than in how scientists find biological markers using many types of data at once. Instead of just one layer, they combine DNA patterns, RNA activity, proteins, and small molecules inside cells. Changes in genes can hint at who might get sick or react to medicine a certain way. At the same time, shifts in RNA and proteins show what's active in real time. What happens deep inside metabolism gets revealed through chemical traces left behind during bodily processes. When all these pieces come together, the result is messy but rich - too tangled for old-style analysis. Tools powered by smart algorithms help make sense of it all. Because of this mix, signals stand out better and hold up under testing. Slowly, steadily, some findings move toward actual medical use - especially where illnesses change form or drag on for years [20,21,24].
11. AI in Drug Discovery and Personalized Drug Delivery
AI helps create custom meds while improving how they’re delivered, depending on each person’s needs.
11.1 AI in Drug Discovery
Serrano’s team showed AI speeds up finding new drugs - by guessing how molecules interact, modeling how compounds act, or spotting potential treatments [32].
AI models get put to work in different ways
Looking at tons of substances online
Predicting drug-target interactions
Mapping disease pathways
Identifying repurposing opportunities
These tools cut down on build time while making exact medicine creation smoother.
11.2 Personalized Drug Delivery Systems
Medicine release systems today include:
12. Ethics Law and Society in Tech
One step toward custom treatments brings weighty questions about ethics, law, and society just as much as it offers medical promise. When gene information meets powerful computing, old rules on privacy and justice start to creak. If protections lag behind progress, confidence in health care could slip quietly away. How choices are honored - and how clearly data is handled - matters just as much as lab breakthroughs when shaping these new forms of therapy [21,22].
Privacy around genetic data raises stakes when it reveals risks for diseases or ties between relatives - effects ripple past one person. When safeguards fail, information might be used unfairly, leading to bias or judgment by others. Protection needs solid rules, systems built for security, and clear limits on who can view what. Trust in medical care and studies depends heavily on how carefully DNA records are managed, as Offit pointed out [33]. What happens to a sample doesn’t stop at the lab - it follows people into their lives.
Not everyone gets the same chance to benefit from custom medical tools. Cost, complicated tech, and scarce expert knowledge block many people. Uneven healthcare setups and location play a role too. Across Europe, some areas lag because equipment differs and payment rules are inconsistent. Precision treatments aren’t rolled out evenly, so patients face different levels of care. Another issue - genetic data mostly comes from narrow groups. That gap makes results less useful for others. When studies miss diverse backgrounds, gaps in health outcomes grow wider [19,28].
Finding out about hidden health clues through gene tests makes agreeing to them trickier than it seems. What happens to your DNA details later matters just as much as the test itself. Family members might be affected without expecting it. Old ways of signing off on medical choices do not cover what comes up now. Clearer paths for permission need to unfold over time, not just once. Real say in tailored healthcare grows when people truly follow how their information moves. Understanding beats assumption every single time.
13. Limits and hurdles in personalized medicine
Few gains have been made, yet hurdles remain in making tailored treatments common practice across all patient groups. Still, uneven access blocks many who might benefit.
When tested on different groups of people, many biological markers do not work the same way, making them less useful in real medical settings [12,21]. Because genes and surroundings mix in complicated ways, guessing how a sickness will go - or how someone might respond to care - gets tricky, especially when multiple factors are involved [22,28].
Facing hurdles in real-world settings? Genomic and multi-omics data often sit unused. Doctors lack preparation, while meaning of genetic changes stays unclear. Heavy computing needs pile up challenges. Systems that do not talk to each other add friction. Progress crawls inside clinics because of these blocks [5,13,25].
Money troubles hit hard when genome tests and custom treatments cost too much, pushing systems to their limits while gaps in care grow wider [1,9]. Even as science moves fast, approval rules and payment setups drag behind - slowing real-world use and shrinking who gets help [19,25]. When some groups rarely show up in research, results lose balance, skewing what works for whom [31].
Looking ahead, new tools and smarter analysis slowly shape how tailored treatments evolve. Each step forward opens different doors than expected before.
Patterns hidden from people come clear when different data types join with smart algorithms. Machines spot what we miss, sorting illnesses into finer groups than before. Prediction grows sharper, timing shifts earlier, thanks to layered biological signals mixed with learning systems. Diagnosis moves faster because connections emerge where none were seen. These methods go further by combining layers of life’s code with computational reasoning [2,15,29].
Early warnings shape smarter health choices, steering medicine before problems grow. Instead of waiting, spotting risks sooner helps stop issues faster. Using existing data to find new uses for medicines speeds up healing options - especially when conditions are tough to crack. This path also saves money, making treatments more reachable over time.
Wider reach begins with cutting expenses, bringing in varied groups, while building stronger understanding of genes. In places like outer space, health care must shift to fit each person - one size does not work when bodies react differently under stress [14,31].
14. Personalized Medicine: Remaining Barriers and Proposed Solutions
Even though things have moved forward, some hurdles still block broad use - obstacles remain despite gains.
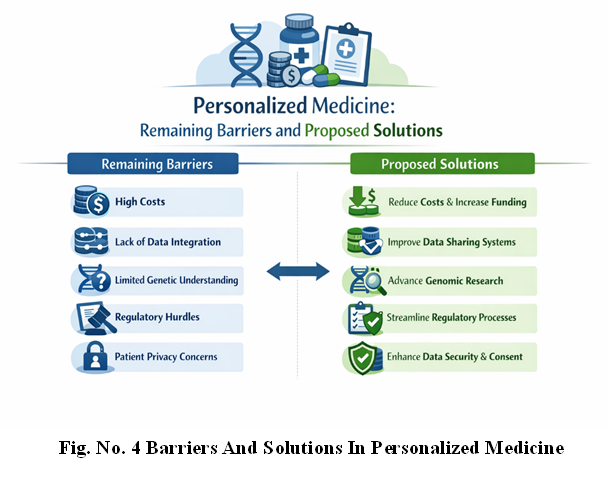
14.1 Cost and Economic Sustainability
Genomic sequencing along with multi-omics tools can cost a lot. Bates pointed out progress won’t stick unless tech gets cheaper, also better value assessments are needed [5].
Proposed solutions:
14.2 Healthcare System Preparedness
Putting tailored treatments into practice means overhauling how medical systems work. Goetz plus Schork pointed out hurdles - like adding DNA details to digital patient files while getting doctors up to speed on reading lab results [21].
Solutions include:
14.3 Ethical and Social Barriers
Offit stressed protecting patients' genetic info - so it’s not abused or used unfairly [33]. As tech moves forward, ethics should keep up - but through different paths.
Key requirements:
14.4 Biological Complexity and Data Gaps
Even after mapping countless DNA sets, we’re still missing key pieces. Paveli?’s team once asked - how solid is personalized medicine really? Turns out, it's a shifting picture [13]. Mixes between genes and surroundings frequently block lab findings from reaching patients.
Solutions include:
15. The Role of Human Diversity in Advancing Personalized Medicine
Lu and team pointed out that differences in people’s genes can strongly affect how well treatments work or who gets sick [28]. If varied groups aren’t part of gene studies, the results might favor some while leaving others behind. While missing key data, tools could end up flawed - so care must be taken during research design.
15.1 Importance of Diverse Genomic Databases
To make sure it works well worldwide:
African genomes need fair inclusion - also Asian ones, while Middle Eastern data shouldn't be left out either, yet Latin American samples matter just as much.
Changes in genes seen more often in people outside Europe need checking to see how they affect medicine reactions.
15.2 Reducing Global Health Disparities
Nimmesgern’s team broke down how Europe handles precise medical care, showing gaps that exist even in wealthy areas [19]. Outside those zones, the differences get way bigger.
Steps forward:
16. Personalized Medicine and the Pharmaceutical Industry
Folks aiming at tailored treatments need fresh ways to make drugs. While old methods fade, new paths open up for better results - each step matters more now than before.
16.1 Targeted Therapeutics and Companion Diagnostics
New medications often need special tests to find the right users. Because of AI, making these targeted treatments is faster - Serrano’s team showed this link clearly [32].
16.2 Challenges in Drug Development
Old-school medicine creation takes forever plus costs a ton. Custom treatments need way more focus
Tiny patient clusters picked by their DNA traits
Adaptive trial designs
Biomarker-guided stratification
These updates make trials run smoother - yet they need fresh rules to back them up.
17. Emerging Models of Precision Healthcare
With personalized medicine moving forward, health systems need to change - bringing in genetic testing, data focused on patients, while weaving in custom treatments. These new approaches mark a big move away from just treating symptoms toward care that predicts issues, prevents problems, yet fits each person differently.
17.1 The P4 Medicine Framework
Folks get treatments that fit their needs, tying into a system focused on foreseeing issues, stopping problems before they start, tailoring plans to individuals, also getting patients involved.
Key components include:
17.2 Digital Health and Remote Personalized Care
Digital health gadgets like wearables or remote trackers grab body info nonstop. So instead of waiting, doctors can tweak treatments based on live updates. Apps powered by smart tech help spot issues before they get worse. This way, care shifts from reacting to staying ahead.
Recent advancements include:
17.3 Personalized Medicine in Aging Populations
With more older people around the world, tailored medical care matters now more than ever. Conditions linked to aging - like cancer, heart problems, or brain-related illnesses - need custom solutions because everyone’s genes react differently, while also handling treatments in their own way.
Bates pointed out that older populations are pushing faster use of targeted approaches - these help boost results while also lifting daily living standards [5].
18. Education and Workforce Transformation
A working system for tailored treatments needs people who understand gene info, while also using combined biological data to guide patient care.
18.1 Training Healthcare Professionals
Key competencies required include:
18.2 Interdisciplinary Collaboration
Personalized medicine relies on collaboration between:
19. Global Implementation Strategies
Putting tailored healthcare worldwide into action needs teamwork, funding, or strong rules behind it.
19.1 Policy and Regulatory Frameworks
Rules need to change fast so new medicines, matching tests, and smart tech can get approved easier. Instead of sticking to old ways, experts like Collins plus Hamburg say fresh thinking helps bring better, safer care to patients sooner [22].
19.2 Strengthening International Research Networks
Working together across countries boosts variety in data while speeding up findings - take, for instance:
19.3 Addressing Ethical and Cultural Barriers
Cultural views shape how people see genetic tests. Because of this, outreach efforts help build confidence while making sure practices respect local values.
Adewoyin with Nwogoh pointed out how public views in numerous nations make it tough to bring in precision medicine - so clear messaging and learning efforts are needed [31].
Future Directions and Innovations
Several innovations will shape the next decades of personalized medicine.
CRISPR-Cas7 helps fix harmful gene errors in body cells - so treatments for inherited diseases might change completely because of it. Still, worries about risks or right-wrong questions mean rules have to be tight. How we use this tool really matters when lives are on the line.
Genomics-based vaccine plans might boost immunity in certain people or groups. While mRNA vaccines were first tested on infections, they're now getting checked out for treating cancer or uncommon illnesses.
The human gut affects how meds work, your immune system, also if you're prone to illness. Coming treatments might tweak microbes, use custom probiotics, or test health through gut analysis.
Khoury and team claimed blending custom data into health policies might boost prevention across large groups [26]. Think gene-based check-ups, local efforts shaped by needs, or outbreaks tracked using smart algorithms.
CONCLUSION
Personalized medicine started as an idea but now it's a hands-on method changing how we treat people today. Thanks to progress in gene studies, protein analysis, and identifying health markers, doctors are moving away from standard treatments that suit everyone - instead they're focusing on care tailored to each person [1–4,10–12].
The use of AI, multi-omics tools, or digital tech is pushing personalized medicine further - seen in cancer treatment, heart care, mental health, infections, even public wellness [3,6,7,8,17,24,26]. Gains have reached unusual spots like outer space, showing how broadly tailored healthcare can work [14].
Still, hurdles stick around - worries about ethics show up alongside steep prices, people's readiness for change, leaks in data safety, also gaps in healthcare access; these need fixing before the world can fully embrace it [18,19,21,22,33]. With tech and science pushing forward, custom-tailored medical care could bring sharper diagnoses, stronger therapies, plus prevention plans built for each person.
The future of healthcare? It’s being built now - driven by tailored treatments, forecasting tools, plus patient involvement - all leading to real shifts in how people stay healthy worldwide.
REFERENCES


Chanchal Ray, Rita Soyam, A Review on Personalized Medicine, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4295-4309. https://doi.org/10.5281/zenodo.18790468
 10.5281/zenodo.18790468
10.5281/zenodo.18790468
