Karnataka College of Pharmacy.
Streptococcus pneumoniae is a major human pathogen causing severe diseases like pneumonia, meningitis, and sepsis. The rising resistance of S. pneumoniae to traditional antibiotics has instigated the development of novel therapeutic strategies. Nanotechnology has been identified as a potential solution, providing better drug delivery, improved bioavailability, and targeted antibacterial action. Nanoparticles such as gold nanoparticles (AuNPs) and polymer-based carriers have been found to hold promise in terms of enhancing antibiotic efficacy with reduced toxicity and the potential for resistance development. Nano systems allow for the controlled release of drugs, providing targeted higher drug concentrations in the site of infection and lowering systemic side effects. Even with these developments, studies are required for optimizing nanoparticle formulations, determining long-term safety, and deploying laboratory results in clinical settings. The future of nanotechnology applications for antimicrobial treatment is highly promising and may transform the treatment of S. pneumoniae infections.
Pneumococcus, also known as Streptococcus pneumoniae, is a common human pathogen that colonizes the upper respiratory tract to cause both invasive and non-invasive infections [1–2]. After Neisseria meningitides, this pathogen is the second most common cause of bacterial meningitis worldwide and the primary cause of community-acquired pneumonia [3].
Other serious infections, such as otitis media, bacteremia, pleurisy, peritonitis, and sepsis, are also brought on by this pathogen [4–5]. The WHO estimates that pneumococcal infections cause 1.6 million fatalities annually, with 0.7 to 1 million of those deaths occurring in children under the age of five, primarily in Asia and Africa [6–7].
Antibacterials like penicillin, clindamycin, rifampicin, vancomycin, and trimethoprim-sulfamethoxazole are used to treat infections brought on by S. pneumoniae. These drugs have varying effects on bacterial structures; for example, b-lactam antibiotics prevent the peptidoglycan, which is the primary component of the bacterial cell wall, from assembling. The macrolides inhibit bacterial protein synthesis by binding to the large 50S ribosomal subunit and disrupting protein elongation because they dissociate the peptidyl-tRNA [11]. Although some antibiotics have shown great efficiency for a long time, their excessive use and incomplete treatment schemes have contributed to the emergence of S. pneumoniae strains tolerant and resistant to antibiotics. The search for new alternatives that help to fight against S. pneumoniae is now considered an urgent need. Nanotechnology has emerged as an alternative that in vitro has proven to be effective, for example, the use of gold nanoparticles (AuNPs) [12–13]. Some properties that make the AuNPs stand out are: they are easily synthesizable [14–15] they are functionalizable [16-17]. they interact efficiently with the surface of bacteria [18-19], and they have a bactericidal effect [20-21]
ECOLOGY OF STREPTOCOCCUS PNEUMONIAE INFECTIONS:
The nasopharynx is the major ecological reservoir of S. pneumoniae; spread from the nasopharynx to the lower respiratory tract or other sites may cause invasive diseases [22]. Children are the major carriers [23,24,25]. Thirty to 50% of young children (< 6 years old) carry S. pneumoniae in the nasopharynx [23,26,27]. Compared with carriage rates of only 4 to 12% in adults [23,25,28] and 8.2% in adolescents [29]. Young age (< 6 years), having young siblings, and attendance in daycare centers are risk factors for nasopharyngeal (NP) carriage in children [23,24,30,27] Risk factors for NP carriage in adolescents or adults include acute upper respiratory tract infection, 23,29 exposures to passive cigarette smoke, [28,29], and asthma [29].
PATHOGENESIS OF STREPTOCOCCUS PNEUMONIAE INFECTIONS:
NP carriage of S. pneumoniae is required to transmit bacteria and invasive diseases [31]. Pneumococci bind to mucosal epithelial cells of the nasopharynx [32]. In normal healthy children, NP carriage of pneumococci is transient and is not associated with disease [33]. However, the disease is caused by contiguous spread to the sinuses or middle ear, aspiration into the lung, or invasion of the bloodstream [32]. Progression to pneumonia requires additional factors (e.g., antecedent viral infections, lung injury, impaired host defences, etc.). Clearance of pneumococci is facilitated by both humoral and cellular immune responses involving monocyte/macrophages, polymorphonuclear leukocytes (PMNs), anti-capsular antibodies, and lymphocytes [32]. Because it inhibits phagocytosis, the polysaccharide capsule is a significant pathogenic factor for invasive illness [32]. During the first two years of life, humoral antibodies against the polysaccharide capsule often form; colonization with certain serotypes may result in humoral antibodies unique to that serotype [32, 34]. Although cross-serotype protection is occasionally shown, protection is serotype-specific [31]. Nevertheless, the protection against IPD offered by these anti-capsular antibodies, whether obtained spontaneously or by vaccination, is insufficient [31,35,36].
An overview of respiratory tract infections:
An infection that affects both the upper and lower respiratory tracts is known as a respiratory tract infection (RTI) [37]. More specifically, it is defined as any respiratory disease that encompasses a range of infections in the throat, sinuses, lungs, nose, and airways. Most of the illnesses related to RTIs do not need medication and get better gradually [38]. However, in some severe cases, antibiotics are the only drugs used for treatment. Rapid diagnosis is important to identify the causative agents and provide timely therapeutic intervention [39]. Both viruses and bacteria can cause RTIs, and in most cases, they spread through direct contact, airborne particles, and droplets from an infected person [40]. Antibiotics are first-line medications for bacterial, mycoplasmic, and chlamydia-caused pneumonia [41], and they also significantly lower the incidence and mortality of pneumonia [42]. Nevertheless, treating bacterial pneumonia with antibiotics is difficult, with the main concern being the emergence of antibiotic resistance, a worldwide issue [43, 44]. The emergence of nanotechnology has reignited interest in treating pneumonia because nano-based drug delivery systems can be used to deliver both systemic and topical therapeutic agents [46,47]. In recent years, nanoengineered drug delivery systems have been recognized as a potential new strategy in the fight against bacterial pathogens [45].
Challenges of Traditional Antibiotic Therapy for Bacterial Pneumonia:
antibiotic treatment is associated with multiple important challenges, including (1) increased antibiotic resistance [48,49], (2) limited range of antibiotic agent types [50], (3) low bioavailability [51], (4) adverse side effects [52], and (5) barrier challenges [51].
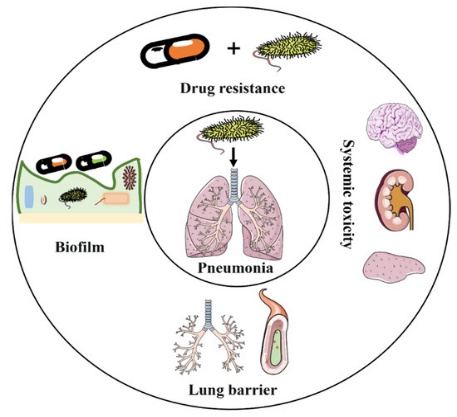
Figure No.1: Challenges in the implementation of intravenous antibiotic agents in the antimicrobial treatment of pneumonia.
Antibiotic Resistance:
Professor Selman Waksman, who identified over 20 antibiotics, coined the name "antibiotics" in 1941 to refer to antimicrobial substances [42]. Antibiotics have now become essential in treating a wide range of inflammatory conditions [53,54].Antibiotics treat bacterial infections in two primary ways: by preventing bacterial development and by directly eliminating the germs [55,51]. One of these modes of action involves disrupting the creation of cell walls. This family of antibiotics causes bacterial swelling and lysis by blocking mucopeptide synthetases, which prevents the synthesis of the mucopeptides that make up the structural foundation of the cell wall [56].
This group of antibiotics comprises glycopeptides and β-lactams like penicillin [56,57]. Inhibition of protein synthesis is a second method of action. By attaching themselves to the ribosomal subunits that are in charge of bacterial protein synthesis, these antibiotics stop bacteria from growing. For instance, macrolides, aminoglycosides, and tetracyclines can bind to the 30S subunit of the bacterial ribosome to prevent protein synthesis [58,59]. A third class of antibiotics interferes with DNA synthesis, as ciprofloxacin inhibits bacterial DNA replication by binding to bacterial topoisomerases II and IV, changing the DNA superhelix [60]
A Limited Range of Antibiotics:
Amoxicillin, fluoroquinolones, third-generation cephalosporins, and macrolides are among the antimicrobial drugs often used in hospitals to treat pneumonia [61–62]. It may be more challenging to treat infections when these antibiotics are used alone or in combination because they can cause the growth of bacteria resistant to them [48]. For this reason, treating bacterial pneumonia requires figuring out how to stop antibiotic resistance from developing. One key tactic to fight resistance is the creation of novel antimicrobial agents. However, the creation of novel antibiotics has advanced slowly despite massive research efforts and resource consumption [63,64]. The pharmaceutical industry embraced genomics and goal-based screening tools in the 1980s to spur antimicrobial discovery [65–66].
Low Bioavailability and High Side Effects of Antibiotics:
Most antibiotics are administered orally or intravenously, which results in systemic distribution; only a small amount of the drug reaches the site of infection [51]. For instance, fluoroquinolones are rapidly excreted through the biliary system after oral administration, and approximately one-third of the drug is eventually found in the stool [67]. The use of antibiotics in clinical therapy is further restricted by the negative side effects brought on by high dosages. For instance, pulmonary toxicity may result from high nitrofurantoin dosages. linezolid may lead to hematologic toxicity, metronidazole may induce neurotoxicity, fluoroquinolones may raise the risk of aortic aneurysm [52], and gentamicin is typically linked with acute renal damage [68].
Nanotechnology:
In recent years, nanotechnology has attracted a lot of interest. In nanotechnology, nanoparticles are the basic building block. Nanoparticles are particles between 1 and 100 nanometers in size and are made up of carbon, metal, metal oxides, or organic matter [69]. The nanoparticles display distinct physical, chemical, and biological characteristics at the nanoscale compared to their corresponding particles at bigger sizes. This phenomenon is attributable to a comparatively greater surface area to the volume, improved reactivity or stability in a chemical process, enhanced mechanical strength, etc [70]. Nanoparticles are used in many different applications because of their characteristics. The nanoparticles differ in diverse dimensions, shapes, and sizes separate from their substance [71]. The nanoparticles are of varied forms, sizes, and architectures. It ranges in size from 1 nm to 100 nm and can be spherical, cylindrical, tubular, conical, hollow core, spiral, flat, etc., or irregular. Surface changes can result in a uniform or uneven surface. Single or multi-crystal solids can be free or clumped together in crystalline or amorphous nanoparticles [72].
The importance of drug delivery in nanomedicine:
Nanoparticles have shown great promise in improving drug delivery systems, allowing for the targeted and controlled release of medications. This has the potential to enhance the efficacy and reduce the side effects of drug therapies. Encapsulating drugs within nanoparticles protects them from degradation, delivers them directly to the target site, and releases them in a controlled manner, maximizing therapeutic effects [73]. This breakthrough in nanomedicine has transformed drug delivery and has enormous potential to improve patient outcomes. By employing nanoparticle-based drug delivery systems, medical practitioners can now precisely regulate the dosage and timing of drug release, resulting in more individualized and successful treatment regimens [74]. Furthermore, the use of nanotechnology in drug administration has created new avenues for the delivery of medications to previously unreachable parts of the body, such as overcoming the blood-brain barrier in the case of neurological illnesses. This innovative technology has the power to revolutionize healthcare and greatly enhance patient care [75]. In addition to delivering therapeutic drugs directly to the brain for neurological disorders such as Alzheimer's disease, nanoparticles loaded with chemotherapy drugs can target tumor cells while sparing healthy cells, reducing the toxic side effects associated with chemotherapy. This targeted drug delivery system has the potential to revolutionize cancer treatment by increasing the efficacy of chemotherapy while minimizing its bad effects on the body [76].
Nanoparticle-Based Drug Delivery Systems:
Nanoparticle-based drug delivery systems have shown potential in improving cancer therapy by selectively delivering medications to cancer cells, avoiding harm to healthy tissues [77].
Nanoparticles can also actively overcome drug-resistant systems within cancer cells, allowing medications to reach their intended targets and exhibit therapeutic effects. Nanoparticles can be made to release pharmaceuticals in a regulated manner, assuring sustained drug levels and reducing adverse effects. Additionally, current research aims to increase the selectivity of nanoparticle-based systems so that they may specifically target cancer cells while preserving healthy tissues. Future research into more individualized and potent cancer therapies might greatly benefit from this [78]. Furthermore, the intricate relationship between nanoparticles and cancer cells may cause unanticipated toxicities or side effects that might endanger healthy organs and tissues. Different nanoparticle-based therapies may be more or less successful depending on the particular kind of cancer cells being targeted [79].
Structure Of the Nanoparticles:
Given that their size, shape, and surface characteristics influence how they interact with immune cells and deliver therapeutic agents, nanoparticles are essential to the efficacy of immunotherapies [80]. The structure of nanoparticles can be optimized by researchers to increase the effectiveness of immunotherapy overall and in terms of targeting. For long-term patient safety and to reduce harmful effects, stability and biocompatibility are crucial. Targeted delivery to certain immune cells or tumor areas is made possible by the safe and regulated release of therapeutic drugs provided by biodegradable polymers such as chitosan and polylactic-co-glycolic acid (PLGA) [81]. These nanoparticles provide gradual, regulated medication release, guaranteeing long-lasting therapeutic benefits and fewer doses. In tissue engineering, scaffolds based on chitosan have been utilized to produce artificial bone or cartilage implants, which offer short-term support structures while encouraging tissue regeneration [82].
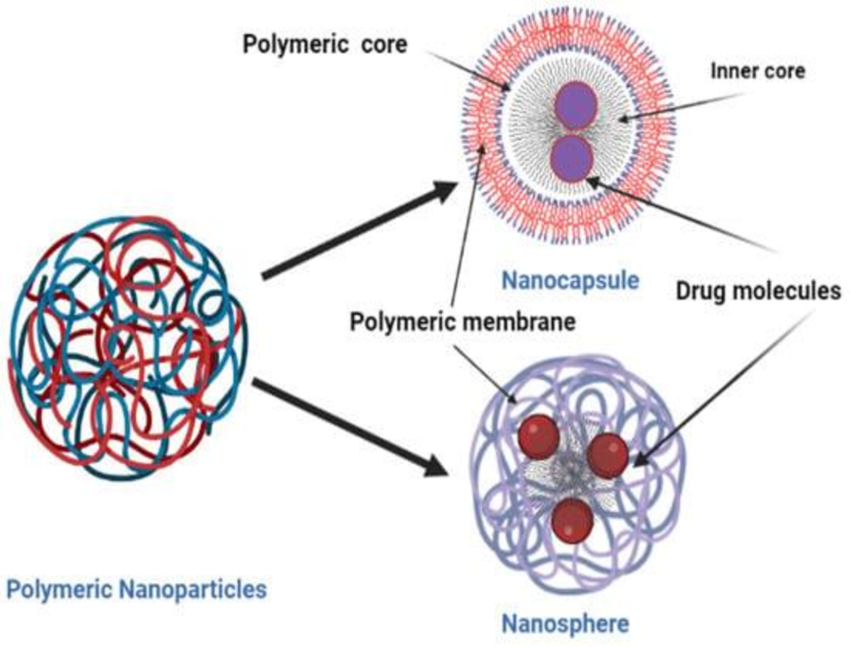
Figure No. 2: Structure of nanoparticles
Types Of Nanoparticles Used in Drug Delivery:
Nanoparticles, like liposomes, polymeric nanoparticles, and metallic nanoparticles, can make different drug delivery systems that work well for certain cancer cells. Polymeric nanoparticles, made from biocompatible polymers, provide a safe and efficient means of drug delivery. In contrast, metallic nanoparticles, like gold or silver, offer unique optical and physical properties for targeted drug delivery and imaging [83]. These nanoparticles can be coated with specific antibodies or proteins that bind to cancer cells, allowing for targeted drug delivery. In addition to their targeting capabilities, biocompatible polymers also offer the advantage of controlled release, allowing for a sustained and prolonged drug effect [84].
Inorganic Nanoparticles:
Because of their special characteristics, inorganic nanoparticles—such as gold and silver nanoparticles—have shown a lot of promise in the treatment of cancer. By specifically targeting cancer cells, these nanoparticles can improve the efficacy of conventional therapies like radiation or chemotherapy. To maximize their safety and effectiveness characteristics, however, more investigation is required. Preventing unintentional injury to patients requires an understanding of the possible long-term consequences of nanoparticles on the human body [85]. To fulfill clinical applications, researchers must also tackle the problem of scaling up the manufacturing of nanoparticles. The broad availability and affordability of these potential cancer therapy alternatives depend on standardized and economical production techniques. Researchers must also think about the moral ramifications of treating cancer with nanoparticles. Furthermore, the establishment of policies and procedures for the safe and responsible use of nanoparticles in clinical settings depends on cooperation between scientists, physicians, and regulatory organizations [86]. According to a clinical study, by concentrating on cancer cells and reducing harm to healthy cells, nanoparticles and chemotherapy medications improved the efficacy of the treatment. Continuous flow reactors are one example of an innovative production approach that has been created to lower costs and guarantee that this state-of-the-art technology is widely accessible [82].
Organic Nanoparticles:
Since they are biocompatible and may be engineered to have certain characteristics, such as the capacity to carry medications to particular regions, organic nanoparticles hold great promise as a substitute for metallic nanoparticles in medical applications [87]. Because these nanoparticles may carry anticancer medications directly to the disease site and precisely target tumor cells, they have demonstrated promise in cancer therapy by lowering side effects and improving treatment effectiveness [77]. Better vision is made possible by the ability of organic nanoparticles to engage with certain tissues or organs and release fluorescent signals. But in addition to the possibility for toxicity and adverse consequences, this method also presents challenges for precisely imaging particular tissues or organs. To completely comprehend the possible hazards and long-term impacts of employing organic nanoparticles in medical therapies, more research is required [88]. Their use in medical treatments also raises questions about the potential long-term accumulation of organic nanoparticles in the body. Unexpected repercussions and negative reactions might arise from this accumulation. Consequently, it is essential to conduct a thorough study to evaluate the safety and efficacy of organic nanoparticles before their widespread usage in therapeutic applications [89].
Hybrid Nanoparticles:
By fusing the benefits of inorganic and organic materials, hybrid nanoparticles provide a viable solution to issues with organic nanoparticle buildup. These nanoparticles can be made more biocompatible and less likely to accumulate over time by adding inorganic materials such as metals or metal oxides [90]. The possible interactions and long-term impacts of these hybrid nanoparticles in the human body, however, require more investigation. Different immune responses may occur depending on the size, shape, and surface characteristics of hybrid nanoparticles [85]. It is generally accepted that organic nanoparticles are biocompatible; nevertheless, introducing inorganic components may cause an immunological reaction that might result in inflammation or other negative consequences. Therefore, before these hybrid nanoparticles are extensively employed in medical applications, it is imperative to look into the immune response to them and ascertain their safety profile [91]. A study on hybrid nanoparticles with both organic and inorganic parts found that smaller nanoparticles with a spherical shape and smooth surface were more likely to pass the immune system and be considered biocompatible [87].
Nanoparticles Preparation:
Coacervation Or Ionic Gelation Method [92]
To prepare the nanoparticles, biodegradable hydrophilic polymers such as sodium alginate, gelatin, and chitosan are used. creating a technique for ionic gelation to produce hydrophilic chitosan nanoparticles. This process creates coacervates that are in the nanoscale range by interacting the positively charged amino group of chitosan with the negatively charged tripolyphosphate.
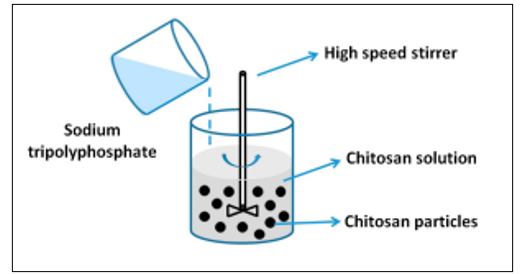
Figure No. 3: Ionic Gelation Method
Solvent Evaporation Method [93]
In this method, the polymer is dissolved in an organic solvent such as dichloromethane, chloroform, or ethyl acetate, which is also used as the solvent for dissolving the hydrophobic drug. The mixture of polymer and drug solution is then emulsified in an aqueous solution containing a surfactant or emulsifying agent to form an oil in water (o/w) emulsion. After the formation of a stable emulsion, the organic solvent is evaporated either by reducing the pressure or by continuous stirring. Particle size was found to be influenced by the type and concentration of stabilizer, homogenizer speed, and polymer concentration. To produce small particle sizes, often, a high-speed homogenization or ultrasonication may be employed.
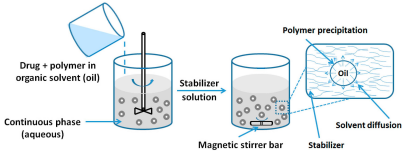
Figure No. 4: Solvent Evaporation Method
Spontaneous Emulsification or Solvent Diffusion Method [94]
This is a modified version of the solvent evaporation method. In this method, the water-miscible solvent, along with a small amount of the water-miscible organic solvent, is used as an oil phase. Due to the spontaneous diffusion of solvents, an interfacial turbulence is created between the two phases, leading to the formation of small particles. As the concentration of water-miscible solvent increases, a decrease in the size of the particle can be achieved. Both solvent evaporation and solvent diffusion methods can be used for hydrophobic or hydrophilic drugs. In the case of a hydrophilic drug, a multiple w/o/w emulsion needs to be formed with the drug dissolved in the internal aqueous phase.
Polymerization Method [95-96]
This process creates nanoparticles in an aqueous solution by polymerizing monomers. After polymerization is finished, drugs are integrated either by adsorption on the nanoparticles or by dissolving in the polymerization media. The suspension of nanoparticles is then re-suspended in an isotonic surfactant-free medium after being purified by ultracentrifugation to eliminate different stabilizers and surfactants used during polymerization. Polybutylcyanoacrylate or poly (alkyl cyanoacrylate) nanoparticles have been produced using this method.
Characterization of Nanoparticles
Zeta Potential [97]
The Zeta potential of a nanoparticle is often used to describe the surface charge characteristic of nanoparticles. It is affected by the particle's makeup and the medium in which it is distributed, and it represents the electrical potential of particles. Because the surface charge stops the particles from aggregating, nanoparticles having a zeta potential greater than (±) 30 mV remain stable in suspension.
Particle Shape [98]
SEM characterizes the nanosuspension before going for evaluation; the nanosuspension is lyophilized to form solid particles. The solid particles are coated with platinum alloy using a sputter coater.
Particle Size [99]
The two most crucial aspects of nanoparticle systems are particle size and size distribution. They ascertain the toxicity, targeting capability, biological destiny, and in vivo dispersion of nanoparticle systems. They can also affect the stability, drug loading, and drug release of nanoparticles. At the moment, dynamic light scattering or photon-correlation spectroscopy are the most common and quick ways to measure particle size. Scanning or transmission electron microscopy (SEM or TEM) is typically used to validate the results of photon-correlation spectroscopy.
Drug Entrapment Efficiency [100]
Ultracentrifugation was used to extract the nanoparticles from the aqueous medium for 30 minutes at 50°C and 10,000 rpm. The decantation and dispersion of the resultant supernatant solution into phosphate buffer saline pH 7.4 followed this. To fully eliminate the unentrapped drug molecules, the process was therefore carried out again. The difference between the total quantity of drug utilized to generate the nanoparticles and the amount of drug present in the aqueous medium was used to calculate the amount of drug entrapped in the nanoparticles. The amount released from the lysed nanoparticle multiplied by 100 is the drug entrapment efficiency (%). quantity of medication initially used to make the nanoparticles.
Advantages of Nanoparticles [101]
The following are some benefits of using nanoparticles as a medication delivery system:
Disadvantages Of Nanoparticles (102,103,104,105,106)
a) Nanoparticles may toxically affect human cells, which might have detrimental biological effects.
b) Environmental risks and inadvertent exposure may result from their tiny size and reactivity.
c) The prohibitively high manufacturing costs and few long-term safety data provide regulatory challenges.
d) Health risks associated with exposure to nanoparticles include cardiovascular, neurological, and respiratory disorders.
e) Variations and high costs result from difficulties in producing and scaling up nanoparticle production.
f) Variability in nanoparticle size may affect their efficacy and excretion from the body.
Limitations Of Nanoparticles [107-108]
a) Small size and large surface area can lead to particle-particle aggregation, making physical handling of nanoparticles difficult in liquid and dry forms.
b) Also, small particle size and large surface area readily result in limited drug loading and burst release. These practical problems must be overcome before nanoparticles can be used clinically or be commercially available.
Applications Of Nanoparticles [109]
Future Perspective:
CONCLUSION:
The study highlights the urgent need for innovative strategies to combat Streptococcus pneumoniae infections, particularly in light of rising antibiotic resistance and the limitations of traditional therapies. It emphasizes the potential of nanoparticle-enhanced approaches, such as gold nanoparticles, which can improve antibiotic bioavailability, reduce side effects, and aid in overcoming resistance. By leveraging the unique properties of nanotechnology, these strategies may offer more effective treatments against bacterial pathogens, ultimately reducing the public health burden associated with pneumococcal infections and addressing the critical challenge of antibiotic resistance.
REFERENCES





Akhilesh Kumar Yadav*, S. Swetha Malika Devi, Beny Baby, S. Rajarajan, Manoj S., A Review on Nanoparticle Enhanced Antibiotic Strategies Against Streptococcus Pneumoniae, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 90-107 https://doi.org/10.5281/zenodo.15319200
 10.5281/zenodo.15319200
10.5281/zenodo.15319200
