Dr. D. Y. Patil College of Pharmacy, Akurdi, Pune.
Medical coding serves as a vital bridge connecting healthcare providers, insurance companies, and regulatory organizations, ensuring smooth communication and efficient operations within the healthcare ecosystem. This overview highlights the core objectives of medical coding, explores its transformative relationship with artificial intelligence (AI), and delves into key aspects such as the coding process, certification programs, the critical importance of accuracy, and opportunities for careers or entrepreneurship in this dynamic field. The advent of AI has dramatically reshaped the landscape of medical coding. By employing technologies like machine learning algorithms, AI has made the coding process more efficient and precise. Automated systems can now analyze vast amounts of healthcare data, translating complex narrative details into accurate medical codes with remarkable speed. This innovation not only accelerates the workflow but also significantly reduces the risk of errors, ultimately enhancing the overall quality of medical coding practices.
Medical coding is all about translating medical diagnoses, procedures, services, and equipment into a universal set of alphanumeric codes. It's a key component of medical billing and plays a critical role in keeping the healthcare industry running smoothly. By meticulously extracting details from patient records, physician notes, lab results, and other medical documentation, coders assign standardized codes for diagnoses and procedures. This process ensures accurate billing, allows healthcare providers to receive the right payment for their services, and helps eliminate billing errors. Additionally, it keeps patient records precise, which is crucial for future care. Beyond billing, medical coding also fuels healthcare data analysis, research, and policy-making, making it an indispensable aspect of the modern healthcare ecosystem. The objective is to provide a comprehensive analysis of current practices, advancements, challenges, and future prospects in the field.It serves as a valuable resource for healthcare professionals, coders, policymakers, and researchers by fostering better understanding and improvements in medical coding systems.
Purpose Of Medical Coding
1. Facilitating Accurate Billing and Reimbursement
Medical coders play a vital role in healthcare by converting medical diagnoses, procedures, and treatments into universal codes such as ICD-10 and CPT. These codes are essential for insurance companies to accurately evaluate claims and decide on the reimbursement healthcare providers should receive. When coding is done correctly, it ensures that healthcare providers are compensated fairly and helps avoid financial setbacks caused by delayed or denied claims.
2. Standardizing Medical Documentation
It offers a standardized way to describe diseases, treatments, and medical procedures, creating a common language that everyone in healthcare can understand. This standardization helps maintain consistency in medical records, no matter the healthcare facility, ensuring accuracy and reliability across the board.
3. Enhancing Patient Care and Safety
Provides an efficient way to maintain accurate records of patients' medical history, treatments, and results. Supports informed medical decisions through well-documented and comprehensive information.
4. Supporting Healthcare Research and Analytics
Enables researchers to study patterns of diseases and evaluate how effective treatments are. Plays a crucial role in monitoring public health and shaping policies to improve community well-being.
5. Ensuring Legal and Regulatory Compliance
Supports healthcare professionals in meeting legal and regulatory standards, such as those set by HIPAA. Helps prevent fraud, misuse, and mistakes in the medical billing process, ensuring accuracy and transparency.
6. Improving Healthcare IT and Automation
Serves as a cornerstone for electronic health records (EHRs) and advancements in healthcare informatics. Facilitates the automation of medical billing and streamlines revenue cycle management, ensuring efficiency and accuracy.
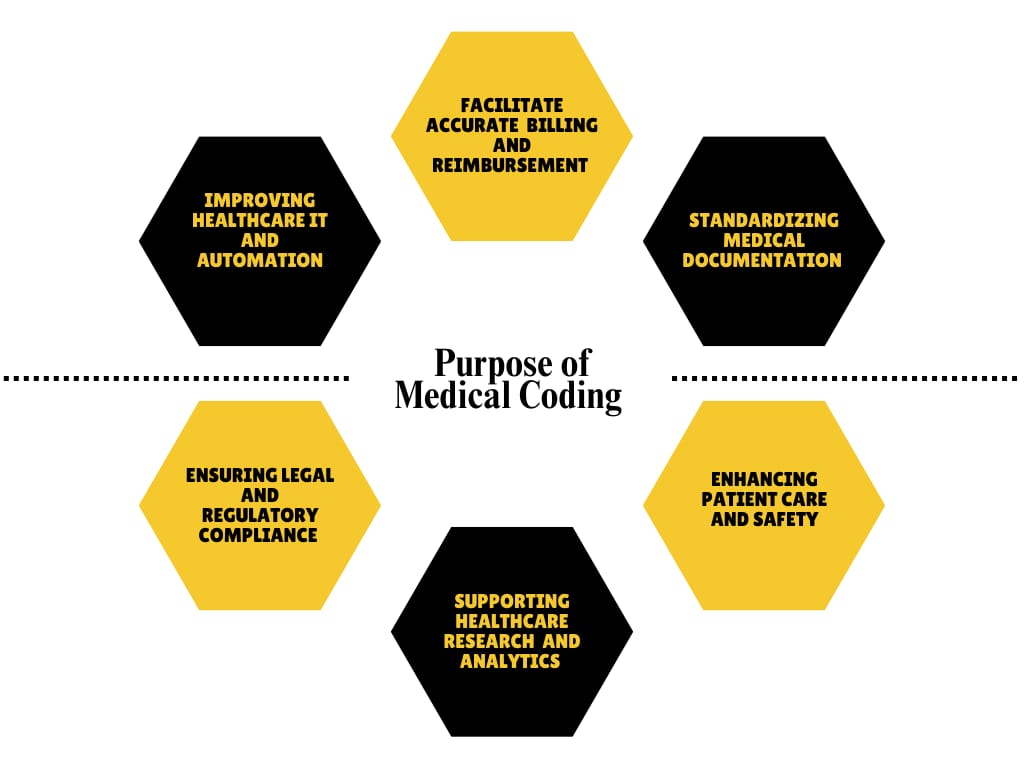
Fig.1. Purpose Of Medical Coding
Process Of Medical Coding
There are two coding processes—manual and automatic
1) Automatic Coding: When researchers input a term into the data collection tool, and it matches exactly with a term from the medical dictionary, the system automatically assigns the relevant code. This streamlines the process and eliminates the need for manual intervention.
2) Manual Coding: However, not all terms are a perfect fit. When a term doesn’t align with the appropriate category or level in the medical hierarchy, automatic coding isn’t sufficient. In these cases, a medical coder steps in. The coder reviews the term, searches for the most suitable match in the designated medical dictionary, and manually assigns the correct code to ensure accuracy.
1) Pre-sales Requirements Analysis: Once the client approves, we move forward with assessing and defining the potential benefits of outsourcing. At this stage, we focus on conducting comprehensive requirements analysis studies. These studies explore the processes that require support, the file types and formats in use, the reports that need to be created, and the required service levels to ensure effective outcomes.
2) Receiving Client Files: The client provides patient charts and related information in the form of scanned copies, which are then securely uploaded to an FTP site for safe access and handling.
3) Downloading and Allocating Files: Once the data is downloaded, the medical coding team ensures it is distributed to the appropriate coders and pre-coders for further processing.
4) Pre-coding: After receiving and downloading their assigned files, Pre-coders extract and document essential details like the physician's name, service location, pricing modifiers, and other key information.
5) Coding: The coding process is divided into two key categories: Procedural Coding and Diagnostic Coding. Certified Professional Coders (CPCs) play a pivotal role in ensuring this process aligns with guidelines such as CPT Assistant, HCPCS Level II, ICD-10-CM, and LMRP. Subsequently, the Coding team reviews the documents to confirm that the assigned procedure codes are accurate and correspond appropriately to the diagnosis provided.
6) Upload of Completed Files: Files with the successfully completed coding work are uploaded to secure FTP site.
7) Quality Evaluation: The client accesses the files uploaded to our FTP site and carefully reviews them to ensure the data meets quality standards and maintains consistency.
8) Feedback from Client: To ensure reliable and precise medical coding services, we take the client's feedback on data quality into account and work collaboratively to implement necessary improvements and adjustments.
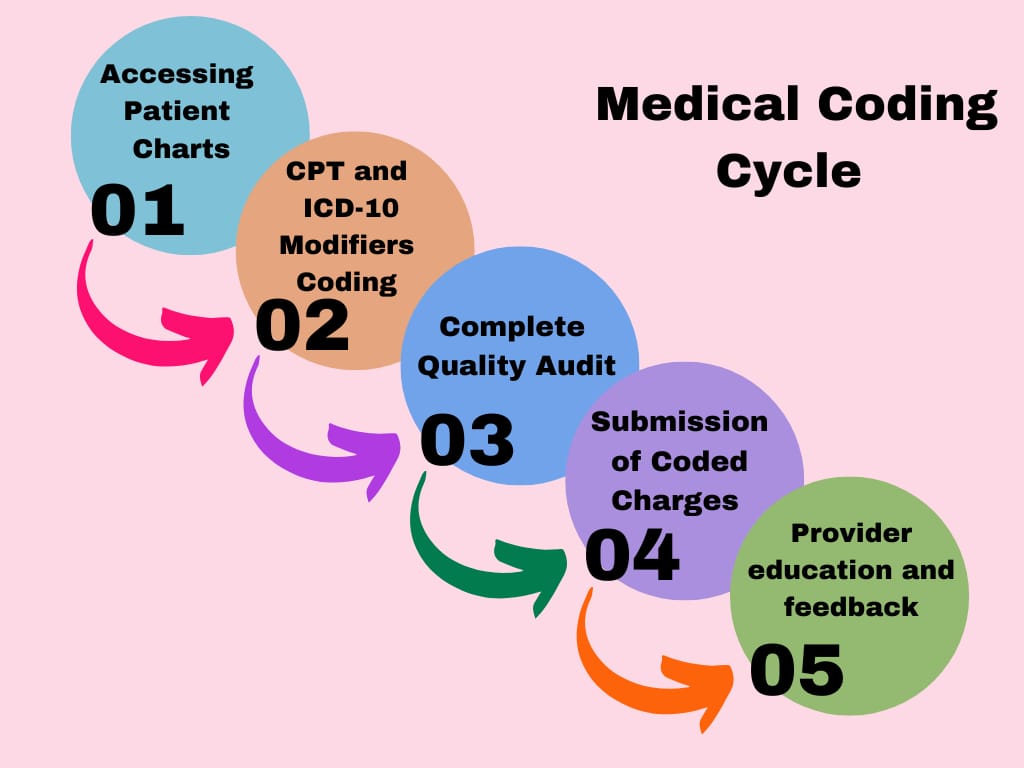
Fig. 2. Medical Coding Cycle
Code Sets Used During the Process
1) ICD-10: International Classification of Diseases, Tenth Revision
Diagnosis codes play a crucial role in healthcare by providing a standardized way to describe a patient’s injury, illness, social factors, and other health characteristics. These codes, essential for billing and record-keeping, are managed using the 10th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-10).
There are two main types of ICD-10 codes:
ICD-10-PCS (Procedure Coding System): Designed specifically for hospital inpatient procedures.
ICD-10-CM (Clinical Modification): Used to categorize diagnoses across all types of healthcare settings.
These codes carry detailed information about a patient’s condition, such as the severity and location of an injury or illness, as well as whether the visit is the patient’s first or a follow-up. For context, the ICD-10-CM set alone has over 70,000 unique codes. The World Health Organization (WHO) oversees this coding system, which is widely used worldwide in various forms to standardize medical records and improve healthcare communication.
2. CPT: Current Procedural Terminology
CPT codes, or Current Procedure Terminology codes, are essential for documenting most medical procedures carried out in a doctor’s office. These codes, which consist of five digits, are published and maintained by the American Medical Association (AMA). The AMA ensures these codes are updated annually and holds their copyright.
CPT codes are divided into three distinct categories:
1. Category I: This is the most commonly used group, covering six main medical specialties: Evaluation and Management, Anesthesia, Surgery, Radiology, Pathology and Laboratory, and Medicine. These codes account for the majority of coding tasks in healthcare.
2. Category II: These are optional codes used to track performance measures or, occasionally, the results of laboratory or radiological tests. These alphanumeric codes are often attached as a hyphenated addition to a Category I code. While they cannot replace Category I codes, they offer additional precision and are particularly useful for monitoring the performance of healthcare professionals and facilities, ultimately reducing the administrative burden on physician offices.
3. Category III: This category is reserved for new and emerging medical technologies. While it is important, coders will generally focus more on the first two categories. Additionally, CPT codes have modifiers—short numeric or alphanumeric add-ons that provide extra details about a medical procedure. For example, modifiers can indicate the side of the body where a procedure was performed. These modifiers enhance the specificity and accuracy of the coding process. The AMA has also introduced updates and addenda to ensure CPT codes stay relevant and precise, making them a valuable tool for streamlining healthcare documentation and communication.
3. HCPCS: Healthcare Common Procedure Coding System
The Healthcare Common Procedure Coding System (HCPCS), often referred to as "hick picks," is an extension of CPT codes, designed to cover services, treatments, and equipment that aren’t addressed by CPT codes. These codes were developed by the Centers for Medicare & Medicaid Services (CMS), the same organization behind CPT codes, and their maintenance is handled by the American Medical Association (AMA). They’re used for documenting items like prosthetic limbs, durable medical equipment, ambulance services, and specific medications. HCPCS serves as the standard coding system for Medicaid, Medicare, chemotherapy drugs, and outpatient hospital treatments, making it a vital tool for medical coders, especially given its connection to government-funded healthcare programs.
The HCPCS system is divided into two levels:
Level I: These codes are closely tied to CPT codes and are primarily used for medical procedures and services.
Level II: This is a separate set of alphanumeric codes, divided into 17 sections. Each section focuses on specific categories, such as medical supplies, laboratory services, or rehabilitation services. Like CPT codes, each HCPCS code must be paired with a relevant diagnostic code to justify the medical procedure. By offering detailed documentation for services outside of traditional CPT coverage, HCPCS plays a critical role in ensuring accurate billing and efficient healthcare communication.
4) Charge Capture Codes
Medical coders play a key role in connecting clinical services, patient care items, and physician orders to what's known as a charge master code. The charge master is essentially a comprehensive list of standard rates for all the goods and services offered by a healthcare provider. Charge capture codes, used in this process, include details like procedure descriptions, time references, departments involved in the treatment, and billable supplies or items. As part of the CMS Hospital Price Transparency rule, hospitals are required to publish their charge masters online, along with the prices for 300 "shoppable" services. This ensures patients can access pricing information more easily. In addition to transparency, these charges also serve another purpose. Revenue cycle management executives use these published prices in negotiations with insurers and payers to secure better reimbursement rates for claims, a process known as charge capture. This helps ensure accurate billing and financial efficiency within the healthcare system.
5) Professional And Facility Codes
Medical coders play an essential role in translating patient records into specific codes that ensure accurate billing and documentation. They use professional codes to detail the services provided by physicians and other clinical staff, connecting these services to the medical records for billing purposes. At the same time, hospitals rely on facility codes to cover the broader costs involved in providing healthcare, including charges for medical equipment, medications, nursing care, and other technical services. These facility codes ensure that the expenses linked to operating a healthcare institution are properly accounted for. In some cases, hospitals include professional codes in their claims—specifically when clinical services are delivered by in-house providers. However, if an external provider simply utilizes the hospital's facilities and resources, the hospital cannot add a professional code to their claims. To simplify this process, hospitals can integrate professional and facility coding onto a single platform. Using advanced technology like computer-assisted coding (CAC) systems can further streamline the process, boosting both accuracy and efficiency in medical coding.
Types Of Errors In Medical Coding
1) Insufficient Documentation
When healthcare providers fail to provide comprehensive patient details—be it about the patient’s overall condition, discharge summary, operative report, diagnosis, or the scope of services rendered—it can lead to serious challenges in documentation. Issues such as missing details, conflicting or incomplete records, or even neglecting certain documents during code assignment can create problems. To ensure accurate code assignment and proper documentation, it’s crucial to pinpoint and address these documentation-related issues. By recognizing and resolving such gaps, the risk of assigning incorrect codes can be minimized, enhancing the overall accuracy and reliability of the healthcare process.
2) Wrong principal diagnosis selection
The principal diagnosis refers to the condition that primarily necessitated a patient’s admission to the hospital. Errors in its selection can occur for various reasons, such as coding a symptom or sign instead of a confirmed diagnosis, failing to use a complication code when required, relying solely on the discharge summary, or assuming a diagnosis without clear, definitive documentation. These mistakes can lead to inaccuracies in coding, affecting the overall quality and reliability of the medical records. Ensuring precise and thorough documentation is key to avoiding such issues and selecting the correct principal diagnosis.
3) Lack of Medical Necessity
A lack of medical necessity arises when a physician does not provide the coder with precise or sufficient details about a patient’s diagnosis. This can lead to incorrect coding during the billing process, which may result in the patient’s insurance company rejecting the claim, citing “lack of medical necessity.” Additionally, submitting claims for items like medical equipment, supplies, or services that are deemed unreasonable or unnecessary can further contribute to such denials. Ensuring clear and accurate communication between physicians and coders is vital to avoid these issues and secure proper claim approvals.
4) Appending inappropriate modifier
Modifiers are two-digit codes added to a service to inform payers about specific circumstances that might affect billing. They are used to clarify any potential misunderstandings, correct inaccurate information, or address specific issues to ensure a claim is processed appropriately. However, improper use of modifiers or applying them carelessly can result in coding mistakes and billing errors. Proper understanding and careful application of modifiers are essential for accurate and seamless claim processing.
5) Non-Response Errors
This happens when a provider fails to submit the necessary documentation to justify the services rendered. In such cases, insurance companies often request clarification to understand the reasoning behind coding for additional services. At times, insurers may require access to medical records before approving reimbursement. These records could include the patient’s medical history, physical examination reports, physician consultation notes, discharge summaries, radiology findings, or operative reports. Ensuring complete and accurate documentation is crucial to avoid delays or denials in claim processing.
6) Documentation written by a medical Student
When medical documentation is prepared by a medical student who lacks experience in the medical field and familiarity with coding guidelines, it can lead to mistakes in coding and billing. Student team members are generally limited to documenting aspects like the review of systems, as well as past medical, social, and family histories. However, it is the physician's responsibility to thoroughly review this information, make any necessary updates, and provide their own documentation before proceeding with billing. This process is crucial to ensure accuracy and prevent potential errors in medical records and billing.
7) Duplicate billing
Duplicate billing happens when a patient is charged multiple times for the same service, procedure, treatment, or test. It can also occur when services are mistakenly billed to the wrong patient, for procedures that were never actually performed, or when claims are simultaneously sent to Medicare, Medicaid, private insurers, or the patient. This can result in repeated charges for the same service, leading to errors in billing and potential disputes. To avoid such issues, meticulous attention to detail in billing practices is essential.
8) Selecting the wrong procedure code
The root cause of selecting an incorrect procedure code often isn’t due to confusion about the procedure itself. Instead, errors frequently arise from inaccurate code details recorded on chart sheets, encounter forms, or electronic charge systems. Another common issue stems from overlooking the editorial comments at the beginning of sections in the CPT book or ignoring the notes provided near specific codes. Paying close attention to these details is essential to avoid such coding errors and ensure accuracy in the process.
9) Outdated knowledge
While medical practices and hospitals often prioritize budget constraints, they sometimes fall short in staying up to date with evolving coding rules. Every year, coding guidelines are updated with additions or deletions to the existing codes. If coders are not familiar with these changes, they might accidentally use outdated codes for services where the codes have been revised, leading to errors. Keeping coders informed about these updates is crucial to ensure accurate and compliant billing practices.
10) Entering Incorrect Information
Errors such as misspellings or typos in key details—like a patient's address, account number, birth date, or other identifying information—can cause significant issues. Mistakes in entries like the insurance ID, date of service, or clinician's name are frequent culprits that often result in claim denials. These problems, however, can be avoided by carefully reviewing and verifying all patient information before submitting claims. Taking this extra step ensures accuracy and helps prevent unnecessary complications or rejections.
Management Of Errors
1) Coding audits
To minimize errors and enhance accuracy, coding audits should become an essential part of the coding process. Rather than being conducted sporadically, these audits should be a continuous effort that fosters regular collaboration among clinicians, coders, and auditors. Integrating coding workflows with databases can simplify data collection and facilitate retrospective audits. Additionally, it’s crucial to consistently track clinical documentation improvement (CDI) metrics—such as query rates, response times, and revenue impact—and evaluate how they influence coding efficiency and productivity.
2) Computer Assisted Coding (CAC)
Computer Assisted Coding (CAC) has demonstrated its ability to boost productivity, enhance accuracy, and ensure consistent coding practices while also lowering overall costs. To minimize billing errors, Parker suggested that payors implement an automated auditing platform capable of verifying the accuracy of clinical coding efficiently.
3) Revenue integrity
Revenue integrity emphasizes improving coding practices and charge capture to lower the chances of noncompliance, ensure accurate and optimized payments, and reduce the costly efforts required to resolve issues later, such as those related to claim edits.
4) Clinical documentation improvement
Hospitals often opt to establish a Clinical Documentation Improvement (CDI) team, bringing together skilled nurses and other professionals. This team works alongside healthcare providers, reviewing patient records in real-time and seeking clarifications to ensure accurate documentation before a patient is discharged. To make this process seamless, it's crucial to have a clear and structured query system in place. This allows the CDI specialists and coders to efficiently gather the necessary details for comprehensive and accurate documentation.
5) Accurate and appropriate medical record documentation
Hospitals often opt to establish a Clinical Documentation Improvement (CDI) team, bringing together skilled nurses and other professionals. This team works alongside healthcare providers, reviewing patient records in real-time and seeking clarifications to ensure accurate documentation before a patient is discharged. To make this process seamless, it's crucial to have a clear and structured query system in place. This allows the CDI specialists and coders to efficiently gather the necessary details for comprehensive and accurate documentation.
6) Medical coder / physician training
Training for providers, clinical documentation specialists, and coders plays a vital role in adapting to the evolving requirements for accurate coding of medical conditions and quality standards. It fosters a shared understanding of both clinical and coding terminology, ensuring better collaboration. Regular, hands-on practice using ICD-10-CM/PCS codes with real patient health records is a practical and effective way to enhance their skills and confidence in documentation.
7) Code with highest level of specificity
The alphabetical index in ICD-10 serves as a resource for diagnosis and procedural terms, while the tabular list organizes codes and their descriptions numerically. To ensure you choose the most accurate and specific code, always rely on the tabular list. The alphabetical index should only be used as a guide and not for final coding decisions. It's also important to code only for confirmed diagnoses and avoid coding for signs or symptoms. Utilizing official coding manuals is often more effective and reliable compared to online tools, payer websites, or reference books for achieving accurate and productive coding.
8) Medical coders’ background
According to a survey conducted by the American Association of Professional Coders (AAPC), several factors influence the accuracy of coding and billing. These include coders’ educational backgrounds, their interactions with physicians, their involvement in billing and compliance processes, and even demographic variables. Key determinants of coding productivity are the coders’ credentials, level of education, and years of experience. Professional coders with a strong grasp of anatomy and medical terminology tend to be the most efficient when assigning codes.
National Medical Professional and Outpatient Coding Certifications
1. American Academy of Professional Coders (AAPC)
The AAPC is recognized as the leading organization in the United States for training and certifying professionals in the administrative and business aspects of healthcare. Its certified members, specializing in areas such as medical coding, billing, auditing, compliance, and practice management, are regarded as experts at the highest level in the field. With a membership exceeding 155,000, the AAPC has a significant presence in the industry. Certification exams, which are overseen by local AAPC chapters, are conducted three to four times annually. These exams last 5 hours and 40 minutes, comprising 150 multiple-choice questions, and require a minimum score of 70% to pass.
- Certified Professional Coder (CPC)
- Certified Professional Coder Apprentice (CPC-A)
- Certified Professional Coder Hospital (CPC-H)
The AAPC also has various other certifications for healthcare auditors, compliance officers, inpatient coding and specialty specific coding.
2. American Health Information Management Association (AHIMA)
The American Health Information Management Association (AHIMA) is a globally recognized leader for professionals in the field of health information management (HIM). With affiliations to 52 state-level associations and a network of over 101,000 HIM professionals, AHIMA is celebrated as a trusted authority for advancing knowledge, education, and training in the industry. Its certification exams, including the CCS-P examination, are held in major cities throughout the year under strict proctoring. To pass the CCS-P exam, candidates must achieve a scaled score of 300 out of 400.- Certified Coding Specialist-Physician (CCS-P)
3. The Medical Management Institute (MMI)
The Medical Management Institute (MMI) is a prominent educational institution specializing in training for medical billing, coding, auditing, management, and ICD-10. With over 25 years of expertise in the Revenue Cycle field and an impressive network of nearly 250,000 alumni, MMI is a trusted name in the industry. Its certification programs equip professionals to become certified in roles such as physician office-based medical coder, medical biller, medical manager, or medical auditor. Graduates of these programs earn respected credentials like RMC, RMB, RMM, and RMA. All MMI certification exams are conducted online, giving candidates a 24-hour window to complete their test once they begin. The exam includes 150 multiple-choice questions, and a minimum score of 76% is required to achieve certification.
MMI certifications include:
- Registered Medical Coder (RMC)
- Registered Medical Auditor (RMA)
- Registered Medical Biller (RMB)
- Registered Medical Manager (RMM)
Effect Of Artificial Intelligence (AI) IN Medical Coding
1. Increased Efficiency and Speed
Automation of repetitive tasks: AI systems can automatically extract relevant data from medical records and input the correct codes, reducing the time spent by medical coders on routine tasks. This allows coders to focus on more complex cases.
Faster claims processing: By automating coding, AI can speed up the submission and approval process for claims, resulting in faster reimbursements for healthcare providers.
2. Improved Accuracy and Reduced Errors
Error reduction: AI-driven systems can analyze vast amounts of data quickly and identify inconsistencies or missing information that a human coder might miss. This helps reduce human error, which can lead to claim denials or legal issues.
Compliance with coding standards: AI can help ensure adherence to the latest coding standards (such as ICD-10, CPT, and HCPCS codes), reducing the risk of non-compliance, which could result in fines or penalties.
3. Cost Savings
Reducing labor costs: With AI handling much of the repetitive coding work, healthcare organizations may need fewer human coders, leading to reduced payroll expenses.
Minimizing claim denials: Accurate coding reduces the likelihood of denied claims from insurance companies, improving the financial flow and reducing the need for costly rework.
4. Improved Coding Quality and Standardization
Consistency: AI ensures that medical coding follows standardized guidelines across different healthcare providers and settings. It can help provide consistent coding practices, making it easier for insurance companies to process claims and for researchers to analyze health data. Real-time updates: AI systems can be updated with the latest coding changes (such as updates in ICD-10 or CPT), ensuring that coders use the most current codes.
5. Better Resource Allocation
Focus on complex cases: With AI handling routine or straightforward coding tasks, human coders can be allocated to more complex or nuanced cases, requiring human expertise to interpret intricate clinical documentation.
Reduced burnout: By offloading repetitive and tedious tasks to AI systems, coders can experience less burnout and job dissatisfaction.
6. Data Analysis and Predictive Insights
Clinical insights: AI can analyze coding patterns and predict trends in medical diagnoses and treatments, potentially offering healthcare organizations valuable insights into patient care trends.
Fraud detection: AI systems can analyze patterns and identify suspicious billing or coding activity, helping detect fraudulent claims or misuse of resources.
7. Challenges and Concerns
Initial setup costs: Implementing AI-driven medical coding systems can require significant investment in technology and training. Job displacement: While AI can improve efficiency, there are concerns that it might lead to job losses, especially in roles that heavily rely on manual coding. Reliability and transparency: AI systems need to be highly accurate to prevent errors. Healthcare providers must also ensure that AI-driven decisions can be explained and audited when necessary, as errors in coding can have serious implications for patient care and billing.
8. Integration with Electronic Health Records (EHRs)
Seamless integration: AI can be integrated into EHR systems to automate coding as part of the documentation process, reducing the need for manual input and increasing the accuracy of coding directly from the medical records.
Benefits Of Medical Coding
1. Accurate Billing and Reimbursement
Medical coding plays a vital role in healthcare by converting detailed medical records into universally recognized codes. This process ensures that healthcare providers can submit accurate bills and receive timely payments from insurance companies. By reducing the chances of claim rejections or delays, coding helps maintain the financial health of medical facilities. Additionally, proper coding guarantees that healthcare professionals are fairly compensated for their services, supporting the delivery of consistent, high-quality care while preserving the financial stability of healthcare organizations.
2. Improved Healthcare Data and Research
Standardized medical coding plays a key role in gathering and analyzing extensive datasets, which can reveal significant trends, patterns, and potential risk factors among patient groups. Such data is invaluable for research, helping healthcare experts develop innovative treatments and enhance patient care. Additionally, medical coding facilitates the monitoring of how effective various treatments and interventions are, driving continuous improvement in healthcare outcomes.
3. Enhanced Communication and Collaboration
Standardized coding acts as a universal language, fostering clear communication and seamless collaboration among healthcare providers, insurance companies, and other stakeholders. By enabling medical professionals to easily exchange information about patients and their conditions, it enhances the coordination of care. Additionally, it streamlines the processes of maintaining medical records and accessing patient data, leading to greater efficiency in healthcare systems.
4. Streamlined Operations and Cost Savings
Medical coding simplifies the billing and reimbursement process, helping to cut down on administrative tasks and boost overall efficiency. Outsourcing coding services allows healthcare facilities to lower staffing expenses and concentrate more on their primary responsibilities, such as patient care and core operations. Moreover, precise coding helps minimize the chances of fraud and curbs unnecessary healthcare spending, fostering a more reliable and sustainable system.
5. Compliance and Risk Mitigation
Medical coding plays an essential role in helping healthcare facilities adhere to regulatory standards and coding guidelines. By ensuring accuracy, it minimizes the likelihood of audits and the potential penalties associated with non-compliance. Additionally, accurate and complete medical records not only meet legal requirements but also safeguard patients' rights and maintain the confidentiality of their personal information.
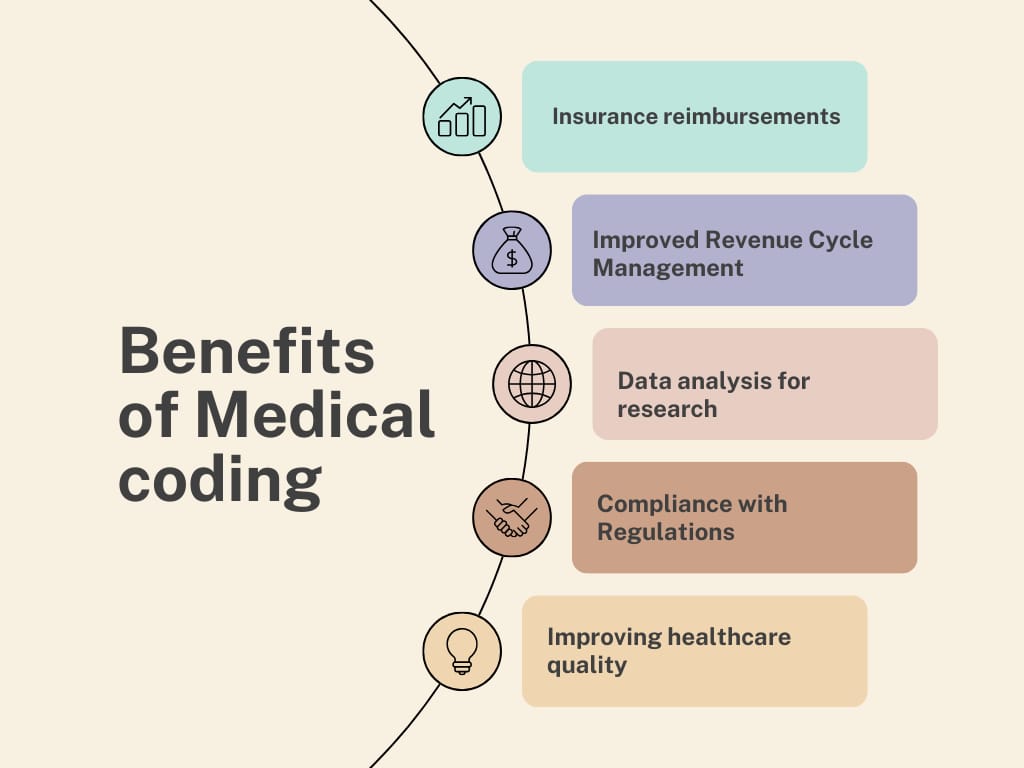
Fig.3. Benefits of Medical Coding
Career Opportunities in Medical Coding
1. Medical Coder
A medical coder is responsible for reviewing patient records and assigning the appropriate codes for diagnoses, procedures, and treatments. This is a highly sought-after role within healthcare organizations such as hospitals, private practices, and insurance companies. Coders typically need to stay updated with the latest coding systems, such as ICD-10, CPT, and HCPCS.
2. Medical Coding Auditor
Medical coding auditors examine the accuracy of codes assigned to patient records. They ensure compliance with federal regulations and help identify errors or inconsistencies in coding. This role often involves working for healthcare organizations or government agencies to ensure proper reimbursement and adherence to laws.
3. Compliance Officer
Medical compliance officers ensure that healthcare practices comply with regulatory requirements and guidelines related to coding and billing. This position requires knowledge of both legal and medical coding practices to ensure organizations avoid legal issues and penalties related to incorrect coding.
4. Health Information Technician
Health information technicians manage patient data and ensure that it is coded, classified, and stored appropriately. They also work with medical records and handle sensitive information, making this role vital in healthcare administration.
5. Medical Billing Specialist
While distinct from coding, medical billing often overlaps with coding duties. Medical billing specialists are responsible for submitting claims to insurance companies and ensuring that payments are processed correctly. Medical coders may choose to specialize in billing for additional career prospects.
6. Medical Coding Trainer or Educator
With the demand for medical coders increasing, there is also a need for educators to train the next generation of coding professionals. Medical coding trainers can work for educational institutions, coding certification programs, or offer their own private tutoring and training sessions.
Entrepreneurial Opportunities in Medical Coding
1. Medical Coding Consultancy
Experienced medical coders can offer consultancy services to healthcare organizations. They can help practices streamline their coding processes, ensure compliance, or implement coding systems tailored to their specific needs. This can involve helping with internal audits, training staff, or optimizing workflows.
2. Medical Coding Business
For those with entrepreneurial ambitions, starting a medical coding business is an appealing option. By offering medical coding services to healthcare providers, insurance companies, or private practices, entrepreneurs can provide essential support for organizations needing outsourced coding services. This type of business can be run remotely, offering flexibility for the business owner.
3. Medical Coding Software Development
As technology continues to play a significant role in healthcare, there is a growing need for innovative software that assists with coding and billing. Entrepreneurs with coding or software development experience can create and sell software solutions that help automate and streamline the coding process, improving accuracy and efficiency for healthcare organizations.
4. Medical Coding Training Program
Entrepreneurs with expertise in medical coding can develop online courses, certification programs, or workshops aimed at training individuals to become professional medical coders. This can be a lucrative business venture, especially with the increasing demand for coders in the healthcare industry.
5. Health Information Management Services
Another entrepreneurial opportunity lies in offering health information management services, which can include coding, billing, auditing, and compliance management. By starting a business that provides comprehensive solutions to healthcare providers, entrepreneurs can serve a broad market, including hospitals, private practices, and insurance companies.
6. Freelance Medical Coder
With the rise of remote work, freelance medical coding is becoming increasingly popular. Medical coders can choose to work independently, offering their services to various healthcare facilities or billing companies on a contract basis. This provides flexibility and the potential to work with multiple clients, increasing income potential.
CONCLUSION
Medical coding stands as the backbone of modern healthcare systems, transforming complex medical procedures, diagnoses, and treatments into a standardized, universally understood language. It not only bridges the gap between healthcare providers and insurers but also ensures the delivery of efficient and accurate patient care. By enabling data-driven decisions, fostering transparency, and ensuring regulatory compliance, medical coding significantly contributes to the overall quality and sustainability of healthcare systems. As the field continues to evolve with advancements in technology and artificial intelligence, the role of medical coding professionals remains irreplaceable. Their expertise ensures precision, integrity, and consistency, which are essential for safeguarding patient well-being and maintaining trust in healthcare systems worldwide. Therefore, investing in training, innovation, and collaboration is paramount to advancing this indispensable pillar of modern medicine.
REFERENCES


Prateeksha Pawar*, Dr. B. V. Yadav, A Review on Medical Coding in Healthcare, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 1863-1878 https://doi.org/10.5281/zenodo.15222504
 10.5281/zenodo.15222504
10.5281/zenodo.15222504
