Department of Pharmaceutics, Shri Sarvajanik Pharmacy College, Mehsana
This review explores the development and potential of in situ nasal gelling systems as a superior delivery vehicle for Vortioxetine Hydrobromide (VHB), focusing on overcoming the limitations of conventional oral administration. Vortioxetine, a multimodal antidepressant, suffers from extensive first-pass metabolism and delayed onset of action when taken orally. Furthermore, the Blood-Brain Barrier (BBB) limits its therapeutic concentration in the central nervous system. Nasal delivery offers a non-invasive "nose-to-brain" pathway, bypassing the gastrointestinal tract. The article evaluates various stimuli-responsive polymers—including pH-triggered (e.g., Carbopol), temperature-triggered (e.g., Poloxamer), and ion-activated (e.g., Gellan gum) systems—that transition from a liquid to a semi-solid gel upon contact with the nasal mucosa. We discuss the mechanisms of mucoadhesion, the role of permeation enhancers, and the pharmacokinetic advantages of increased residence time
Nowadays, nasal drug delivery has drawn a lot of attention because to its easy, promising, and dependable method of systemic drug administration, particularly for medications that are ineffective when taken orally and require injections. Large surface area, a porous endothelium membrane, high total blood flow, avoiding first-pass metabolism, and easy accessibility are all provided by this pathway. Due to the lack of pancreatic and stomach enzymatic activity as well as interference from gastrointestinal contents, the nasal mucosa is also more permeable to substances than the gastrointestinal system. [1] Nasal drug administration was only used topically for medications meant to have local effects in the early historical records. But in recent years, its use has expanded to target many other parts of the body in order to have both local and systemic effects. Nasal medication distribution also has a special role in traditional medical systems, such as the Ayurvedic system of Indian medicine, which is known as "Nasya karma" and is a widely accepted kind of treatment. [2]
Possible Nasal Drug Delivery:
A. Local Delivery: [3, 4]
When opposed to oral administration, nasal distribution offers the least chance of systemic side effects, making it suitable for local (or topical) treatment.[3] As a result, nasal administration of relatively low dosages has minimal systemic adverse consequences. In addition to antihistamines and corticosteroids for allergic rhinitis, well-known therapeutic medication types include decongestants for cold nasal symptoms. [4]
B. Systemic Delivery: [5]
When compared to oral and intravascular methods of administration, intranasal delivery of medications is an efficient way to ensure systemic availability. Compared to oral and parenteral delivery, it offers quicker and longer drug absorption. Analgesics, cardiovascular medications like propranolol and carvedilol, hormones like levonorgestrel, progesterone, and insulin, anti-inflammatory medications like indomethacin and ketorolac, and antiviral medications like acyclovir are among the therapeutic classes of medications administered. Zolmitriptan and sumatriptan are two examples that are on the market for treating migraines and cluster headaches.
C. Nasal Vaccines: [6]
The use of nasal mucosa for immunization, primarily for respiratory illnesses, has been thoroughly examined since it is the first point of interaction with inhaled antigens during inhalation9. Since nasal vaccination can raise systemic levels of particular immunoglobulin G and nasal secretory immunoglobulin A, it is actually a prospective substitute for the traditional parenteral approach. Intranasal vaccinations against influenza A and B viruses, proteosoma influenza, adenovirus-vectored influenza, Group B meningococcal native, attenuated respiratory syncytial virus, and parainfluenza 3 virus are examples of how effective they are for humans.
Central Nervous System (CNS) Delivery through Nasal Route: [7, 8]
The medications can reach the brain through the intranasal route. The olfactory neuroepithelium is where medications are delivered from the nasal pathway to the central nervous system.[7] There have been reports of drug administration via the nasal route into the central nervous system for conditions like Alzheimer's disease, brain tumors, epilepsy, pain, and sleep disturbances.[8]
Advantages of Nasal Drug Delivery System: [9]
Limitations: [10]
ANATOMY & PHYSIOLOGY OF NASAL CAVITY [11,12]
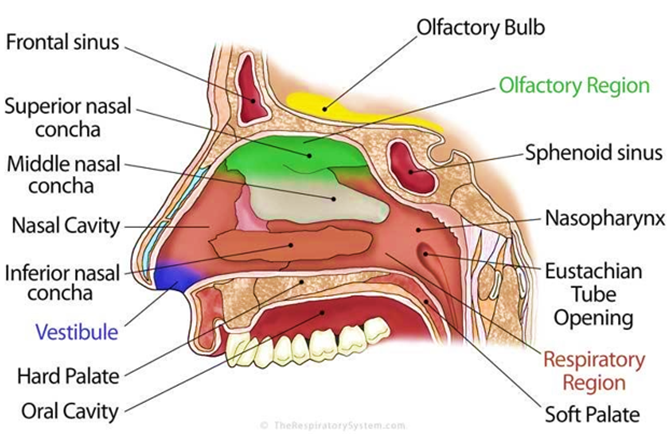
Figure 1: Anatomy of nasal cavity
The nasal vestibule, which is the most anterior portion of the nasal cavity, opens to the face through the nostril. The nasal septum separates the nasal cavity into two halves and extends posterior to the nasopharynx. The nasal vestibule, olfactory region, and respiratory region are the three primary areas that make up the nasal cavity. The nasal cavity's lateral walls, which comprise a folded structure, can increase the nose's surface area by around 150 cm2. This is a fairly big surface area in relation to its tiny volume. The superior, median, and inferior turbinates make up this folded structure. The primary nasal airway's tiny passageways, which are typically 1-3 mm wide, are beneficial to the nose. [11]
The nasal vestibule, which is covered with skin-like stratified squamous epithelium cells, is part of the nonolfactory area of the nasal cavity's mucous membrane. The respiratory region, on the other hand, has a typical airway epithelium covered with numerous microvilli, creating a large surface area available for drug absorption and transport. This causes the mucus layer to move from the anterior to the posterior region of the nasal cavity. The mucus membrane that covers the atrium and nasal turbinate contains goblet cells, which release mucus in the form of granules that swell in the nasal fluid and add to the mucus layer.
About 95% water, 2% mucin, 1% salts, 1% additional proteins such al-bumin, immunoglobulins, lysozyme, and lactoferrin, and 1% lipids make up the mucus secretion. Mucus secretion protects the immune system from viruses and bacteria that are inhaled.It also carries out certain physiological tasks. It protects the mucosa both physically and enzymatically by covering it. The mucus has the ability to retain water. It has electrical activity on its surface. It makes effective heat transfer possible. It transports particulate debris to the nasopharynx and functions as an adhesive. [12]
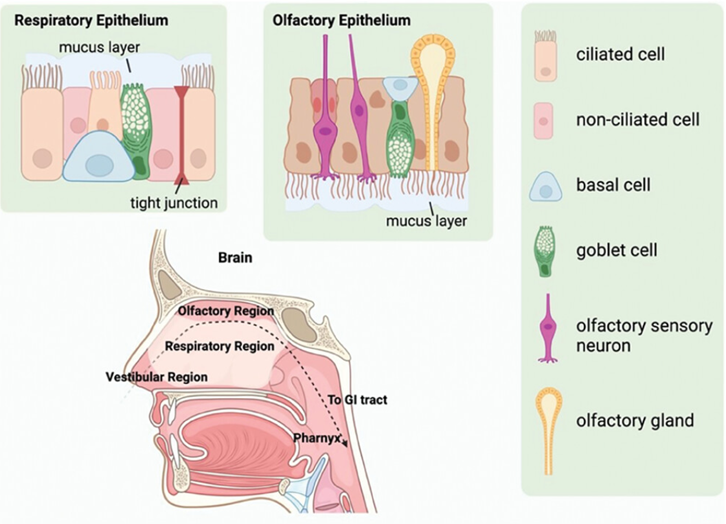
Figure 2: The nose anatomy with epithelium structures
IN SITU NASAL GEL [13-16]
Since ancient times, people have used their noses to give drugs for both medicinal and recreational purposes. The use of the nasal route to transport medications to the brain through the olfactory region has drawn a lot of attention in recent decades.
Due in part to its appeal for immunization during the Covid-19 epidemic, research into the intranasal route has quickly gained prominence in recent years. Nasal administration has potential benefits as a non-invasive method, including quick onset of action, easier application, and improved patient compliance. [13]
Thus, the nasal route is an attractive route ofadministration compared to traditional ad-ministration routes.
Nasal administration has several clear benefits for drug delivery in addition to the benefits it offers for potentially quick and patient-friendly vaccination: The first-pass impact and degradation brought on by gastric acid when taken orally can be mitigated by nasal administration. Because of the direct connection between the brain and the olfactory area in the nasal cavity, it can avoid the blood-brain barrier (BBB). Furthermore, due of its widespread vascular circulation, it provides rapid action and compliance for systemic drug delivery. [14]
In situ gel formulations have been investigated for both local and systemic medication administration among the various nasal drug delivery systems. Before being provided, these drug delivery systems are in sol form; however, after being administered, they go through gelation to form a gel. The temperature of the microenvironment, pH variations, ion presence, UV radiation, and polymers are the variables controlling the in situ gel formation process.
Gels' rheological characteristics, which are essential to their effectiveness, play a key role in keeping the gel at the application or absorption site. In order to avoid first-pass metabolism and increase bioavailability, the current work attempts to formulate loratadine into nasal in situ gel. [15]
However, nasal delivery is not without its difficulties. One of the main obstacles to drug retention is nasal mucociliary clearance (MCC), a physiological process that occurs naturally in the human body. Every 15 to 20 minutes, MCC occurs to remove foreign pathogens and particles from the nose. It also clears drug formulations, which results in shorter drug retention periods at the targeted site of action, a significant contributing reason to reduced therapeutic efficacy. Furthermore, liquid formulations may flow back to the throat after delivery because of the architecture of the nose. Apart from the issue of retention, nasal administration frequently necessitates the use of tools like a spray to apply the drug formulations, which frequently calls for evenly distributed coverage. More and more research is concentrating on developing nasal sprays to accommodate various dosage forms; The final section of this review discusses a few of them. It is still necessary to handle the possibility of inhalation during application. Therefore, extending the duration of drug residence is the main obstacle to overcome in order to completely establish the nasal route as a feasible mode of administration. Because in situ gel compositions are solid, they present an alluring approach to overcoming MCC.
In-situ gels are easy to administer and reduce the need for frequent dosing, patients find them more convenient and comfortable.
Preparation Methods of In?situ gel:
In situ gel preparation uses a number of techniques, such as:
EVALUATION PARAMETERS OF IN SITU NASAL GEL [17-19]
The developed formulations will be visually examined against a white background to check for clarity, color, and the presence of any particulate matter in the solution or gel form.
One milliliter of the prepared gels will be transferred to a 10 ml volumetric flask, and the solution will be diluted with distilled water. The pH of the resulting solution will be determined using a digital pH meter. [17]
The viscosity of the in situ gel will be determined using a Brookfield viscometer. The measurements will be taken at 4 °C and 35 °C using spindle no. 27 and 64, respectively, at a shear rate ranging from 0.3 to 20 rpm. The formulation under study will be placed in the sample holder, and the spindle will be inserted perpendicularly into the sample. The spindle will be rotated at a constant optimum speed. The viscosity determinations of the formulation will be carried out before (at 4 °C) and after (at 35 °C) the formation of the gel.
The Brookfield Viscometer will be used to examine the rheological characteristics of in situ gel compositions. Initially, the temperature will be maintained above 40 °C. By increasing the spindle rotational speed from 0.3 to 100 rpm, the rheological parameters will be examined and the viscosity (η), shear rate (γ), and shear stress (τ) will be recorded. Each measurement will be carried out three times. [18]
A rheometer will be used to assess this parameter. A certain amount of gel will be prepared in a beaker from the sol form, depending on the gelling agent's method of action. The beaker containing the gel will be elevated at a set rate, allowing the gel to be probed slowly. The probe's variations in load will be determined by measuring the probe's immersion depth below the gel's surface.
Take 2 mL of the gel sample in a test tube. Immerse the test tube in a water bath. Gradually raise the temperature of the water bath by 1°C every 2 minutes, starting from room temperature. Keep checking the sample until the gel forms. Gelation is considered to occur when the liquid sample stops moving even when the test tube is tilted at 90°.
It will be the temperature at which the gel will transform from liquid to solid. For thermoreversible vaginal gel, a gelation temperature range of 30–36°C will be considered appropriate. When the test tubes will be tilted to a 90° angle, the temperature will progressively rise to the "gelation point," which will be the point at which the formulations will no longer flow. When a pH- or ion-dependent polymer will come into contact with vaginal fluid, it will change from a sol to a gel. [19]
VORTIOXETINE: [20-21]
Over 10% of older persons suffer from major depressive illness, which is typically linked to negative consequences. The first-line pharmacological therapy for treating late-life depression is typically selective serotonin reuptake inhibitors (SSRIs). [20]
One of the most common mental illnesses is major depressive disorder (MDD), which is typified by vegetative symptoms, diminished interest, sad mood, and cognitive dysfunction. Women are twice as likely as males to have major depressive disorder (MDD), which affects about 6% of adults globally each year. It is expected that 20% of all people will at some point in their lives meet the criteria for MDD. MDD is thought to be the leading cause of illness burden and years spent disabled, and it has a detrimental effect on quality of life. MDD has been connected to an increased risk of cancer, diabetes, stroke, Alzheimer's disease, and cardiovascular disease in addition to suicide.
Interestingly, vortioxetine's mechanism of action is said to be unique and connected to the blockage of the serotonin transporter and the regulation of several serotonin receptors. [21]
History: [22]
The FDA authorized vortioxetine hydrobromide (referred to as vortioxetine in the material that follows) in September 2013 for the treatment of major depressive disorder. Vortioxetine is a multimodal antidepressant with a number of distinct modes of action. Vortioxetine is useful not just for MDD but also for managing depressive symptoms in older individuals, treating bipolar depression, and reducing depressed symptoms in epileptic patients. In therapeutic settings, vortioxetine is well tolerated and rarely causes severe side effects.
How should I take vortioxetine? [20]
As directed by your physician, take vortioxetine. Read all drug guides and adhere to all instructions on your prescription label. Your dose may occasionally be altered by your physician.
Typically, vortioxetine is taken once day, either with or without food.
If you abruptly stop using vortioxetine, you can experience withdrawal symptoms. Before quitting the medication, ask your doctor.
Side effects of Vortioxetine [23]
DEPRESSION: [24]
As estimated by WHO, depression is a common mental disorder that presents with depressed mood, loss of interest, feelings of guilt, disturbed sleep or appetite, low energy and poor concentration. Not just adults, but 2% of school children and 5% of teenagers also suffer from depression. It can result from a combination of biological, psychological and social factors. Depression affects people of all ages and backgrounds and can be temporary or long-lasting.
Symptoms:
Depression affect: [25]
Anyone can experience depression, including adults and children.
CONCLUSION
In situ gels significantly enhance the bioavailability of VHB, providing a rapid therapeutic response and reduced systemic side effects, marking a pivotal shift in the management of Major Depressive Disorder (MDD). It is Providing a needle-free, easy-to-administer alternative to traditional tablets, which is particularly beneficial for patients with dysphagia or those requiring rapid stabilization.
REFERENCES



Mitali Oza, Krina Patel, Varsha Chaudhary, Dr. Pankaj Prajapati, A Review on: In-situ Nasal Gel of Vortioxetine hydrobromide, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1666-1674. https://doi.org/10.5281/zenodo.19046381
 10.5281/zenodo.19046381
10.5281/zenodo.19046381
