ITM SLS BARODA UNIVERSITY
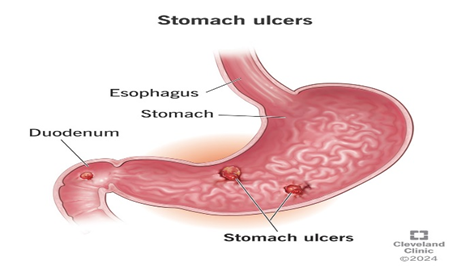
Breaks in the stomach lining's mucosa that pass through the muscularis mucosa and have a diameter greater than 5 mm are known as gastric ulcers. The changes in the stomach's defense mechanisms can alter the gastric mucosa, which can lead to erosion and ultimately ulceration. The two main factors impairing mucosal resistance to injury are Helicobacter pylori (H. pylori) infection and non-steroidal anti-inflammatory drugs (NSAIDs). Gastric acid secretion or pepsin cause the inner lining of the gastrointestinal (GI) tract to discontinue, which is a characteristic of gastric ulcers. It penetrates the gastric epithelium's muscularis propria layer. It typically happens in the proximal duodenum and stomach. It could affect the jejunum, distal duodenum, or lower esophagus. Patients with gastric ulcers typically experience epigastric pain, 15 to 30 minutes after eating. On the other hand, a duodenal ulcer typically causes pain two to three hours after eating. Proton pump inhibitors (PPIs) and histamine-2 (H2) receptor antagonists are two gastric ulcer treatments that have shown side effects, relapses, and a variety of drug interactions. However, a variety of diseases can be prevented and treated with the help of medicinal plants and their chemical compounds
A peptic ulcer, also known as a stomach ulcer, is characterized by extensive damage to the mucosa or lining of the stomach and duodenum that goes beyond the muscular mucosa, notably to the muscle layer, due to the environment's generation of gastric acid. The two most frequent etiological antecedents are chronic Helicobacter pylori (H. pylori) infection and the use of nonsteroidal anti-inflammatory drugs (NSAIDs), which naturally include acetylsalicylic acid (ASA). Less than 5% of cases of peptic ulcer PU are caused by particular, uncommon, and carefully considered coupled antecedents. Among these is gastronomy, or Zollinger-Ellison syndrome (ZES). (1)
Since excessive gastric acid secretion was thought to be the main cause of the gastric ulcer, the previous treatment concentrated on lowering stomach acid output with antacids, histamine, H2 receptor blockers, and proton pump inhibitors. The main culprit behind stomach ulcers, Helicobacter pylori, could not be eliminated by such medications, however. Antibiotics have the potential to eradicate Helicobacter pylori, but their long-term use can cause toxicity and the emergence of antibiotic resistance in bacteria. As a result, there is an urgent need for safe, effective, and reasonably priced anti-ulcer medications. Herbal remedies have naturally occurred active ingredients that could have anti -ulcer characteristics are a potentially effective new treatment option for stomach ulcers. (2)
There are four times as many peptic ulcers in the duodenum. Since around 4% of stomach ulcers are caused by metastases, many biopsies are required to rule out cancer.
Duodenal ulcers are often benign. Convex, resembling a colon polyp, concave, pit-like, or classic erosive ulcers are some possible ulcer shapes. The duodenum and pylori generally exhibit the convex form, whereas the right stomach usually exhibits the erosive concave form. Although the shapes of these convex growths vary, they are invariably higher than the surrounding tissues. These growths are distinguished by the mucosal tissues' persistent lack of surface breaches, and even at larger sizes, they first fail to distinguish themselves visually from nearby tissues. (3)
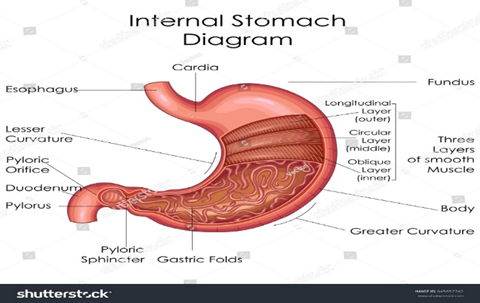
ANATOMY OF STOMACH:
The bottom portion of the rib cage covers the left hypochondrial area, which is where the stomach is primarily located. On the other hand, the upper umbilical and epigastric regions of the abdomen include the lower and distal portions of the stomach. The stomach is an organ that may expand. It can hold 1.5 litres on average in an adult. The stomach is roughly J-shaped, though some people may have a steer-horn stomach, in which case it lies transversely. Depending on the person's posture and how full their stomach is, the size, shape, and location of the stomach can change significantly. The stomach seems flattened when empty. It has two surfaces: the anterior and the posterior, which are separated by larger and smaller curvatures.
In the diagnostic interpretation of gastric diseases and their treatment, endoscopists, radiologists, and surgeons consider the notable physiological and histochemical variations among the stomach's regions. Projecting upward above the level of the heart opening is the stomach's fundus. It connects with the left diaphragm dome while lying to the left of the abdominal oesophagus. There is a noticeable notch called the angular notch (incisura angularis) two-thirds of the way from the cardiac orifice along the stomach's lesser curvature. The stomach's body stretches from the cardiac orifice to the angular notch. (4)
(5)
PHYSIOLOGY OF STOMACH:
An organ's structure mostly determines the role it serves in the body, as is the case with the majority of physiological processes. The purpose of the stomach wall is to help create a temporary acidic environment that facilitates the breakdown of food into chyme, a semisolid mixture. The fundus, cardia, body, and pylorus are the four parts of the stomach organ. The stomach's inner surface is rotated to give the gastric mucosa more surface area, which permits the stomach to expand as food is consumed. The mucosal layer, submucosa, muscularis externa, and adventitia/serosa are the four distinct tissue layers that make up the stomach wall. The lamina propria, a layer of connective tissue, the muscularis mucosa, and the surface epithelium are the three additional layers that make up the stomach mucosal layer. (6)
PATHOPHYSIOLOGY OF STOMACH ULCER:
H pylori infection and long-term NSAID use are the main causes of PUD cases. Usually, the infection starts early in childhood and lasts for a few decades. The two primary modes of transmission for H pylori are fecal-oral and oral-oral. This bacterium is primarily seen in developed nations and is primarily spread by oral-oral transmission. Sharing utensils during meals appears to be the main way that infections spread across family members, particularly from an adult to a youngster. Contaminated water, which is frequently seen in nations with inadequate sanitation, is the source of fecal-oral transmission.
The helical (spiral) gram-negative bacterium H pylori causes harm to host cells by colonizing the surface of stomach epithelial cells and causing an adverse inflammatory response. Numerous bacterial virulence factors that contribute to the pathophysiology of PUD have been identified. Three pathogenic pathways can be distinguished in H pylori infection: immune evasion, illness induction, and colonization. (7)
(8)
CAUSES OF STOMACH ULCER:
Ulcer disease is thought to be primarily caused by excess acid. Therefore, neutralizing and controlling stomach acid secretion is the main focus of treatment. According to Franceschi et al. (2014), acid is still thought to have a key role in the development of ulcers. The primary cause of ulcer illness nowadays is thought to be a stomach infection caused by a bacteria known as "Helicobacter pyloricus" (H. pylori). The use of long-term anti-inflammatory medications, sometimes known as NSAIDs (anti-inflammatory drugs), such as aspirin, is another significant cause of ulcers. Additionally, smoking contributes significantly to the development of ulcers and the failure of ulcer therapy.
The bacteria Pylori is quite prevalent. Globally, these bacteria infect around one billion individuals. According to estimates, 50% of Americans over 60 have H. pylori infections (Parsonnet et al. 1996). More than 80% of individuals with stomach and duodenal ulcers have an H. pylori infection, which often lasts for years and causes ulcers in 10% to 15% of those infected. However, the exact process by which H. pylori causes ulcers is still unknown. It has been amply demonstrated that using antibiotics to eradicate these germs stops ulcers from returning. NSAIDs are medications used to treat painful inflammatory diseases and arthritis, according to Brewer et al. (2010). NSAIDs alter the composition of stomach mucus, which may make it easier for pepsin to break it down.
Examples of medications in this class include aspirin, ibuprofen (Motrin), naproxen (Naprosyn), and etodolac (Lodine). Prostagladins play a crucial role in preventing gut lining injury. Corrosive acids. Overproduction of prostaglandins is crucial for the protection of the stomach mucosa. By interfering with prostaglandins in the stomach, NSAIDs lead to ulcers. (9)
CLINICAL SYMPTOMS:
Patients with NSAID-induced PUD often report experiencing regurgitation and heartburn. The main cause of this is gastroesophageal reflux brought on by PUD-induced erosions. Patients could also exhibit bleeding symptoms. Alarming symptoms including melena and hematemesis are linked to the bleeding, which is a major PUD consequence. Anorexia may be one of the symptoms of a PUD patient.
This weight loss worry is often linked to postprandial discomfort. Anemia, which is usually caused by GIB or iron deficiency, may also be to blame. Although PUD is usually associated with recurring ulcers caused by NSAID misuse, it can occasionally result in serious, potentially fatal effects like bleeding and perforations. (10)
DIAGNOSIS:
Numerous techniques are available to identify H. pylori infection. Due to its trophic status for gastric epithelium, the organism is mainly found in the stomach, where it produces the distinctive and easily identifiable histologic pattern of acute-on-chronic inflammation. The most accurate method of detecting organisms is immunohistochemistry utilizing antibodies specific to H. pylori. Usually, organisms are abundant and may be identified using specialized stains. There are numerous more tests available, from molecular testing with next-generation sequencing to serologic assays for anti-H. pylori IgG antibodies. While some tests can be performed noninvasively, others need an endoscopy to take a sample of the stomach contents. Non-invasive testing is usually preferable.
One of the current requirements for using IgG serology is having a very high pretest chance of an H. pylori-related condition, like an active duodenal ulcer. If serology is performed without a very high pretest probability, it is advised that, depending on the presentation, a urea breath test (UBT), stool antigen test, or endoscopy be performed to confirm the presence of an active infection prior to beginning therapy. The UBT and stool antigen test are non-invasive methods for detecting active infection. (11)
COMPLICATIONS OF STOMACH ULCER:
The outcomes of PUD (adenocarcinoma and MALT lymphoma) included persistent symptoms, bleeding, perforation, penetration, limitation of the stomach outlet, and gastric cancer. In 15 to 20% of cases, bleeding is the most common outcome. The majority of acute upper gastrointestinal bleeding (40–60%) is brought on by PUD. Upper gastrointestinal bleeding must be assessed and treated immediately since it is an emergency. When inspecting a bleeding patient, alerting a GI expert early on can aid in the coordination of severely ill patients' care. To categorize risks, Glasgow-Blatchford and Rockall ratings were employed. For treatment, proper resuscitation using intravenous fluid and blood products is necessary to maintain the target hemoglobin level above 7.
Activated charcoal can be given within four hours of ingestion to treat a NOAC overdose. Idarucizumab with hemodialysis can be used to treat life-threatening bleeding caused by dabigatran. The use of anticoagulants and antiplatelet medications can resume if hemostasis has been achieved. The timing is determined by the speed with which anticoagulation must be restored. Due to the increased risk of acute thrombosis following the implantation of a drug-eluting stent, patients receiving dual antiplatelet therapy should refrain from discontinuing both drugs patients who immediately begin taking aspirin after reaching hemostasis (within 1-3 or 7 days). Low molecular weight heparin cross-linking is recommended for patients with mechanical mitral valves or other thrombotic disorders since their warfarin levels are below therapeutic ranges. (12)
TREATMENT:
MANAGEMENT:
(14)
ROLE OF HERBAL & NATURAL MEDICINE USED FOR ULCER PREVENTION:
|
PLANT NAME
|
COMMON NAME |
FAMILY |
PART USED |
CHEMICAL CONSTITUENTS |
ROLE IN ULCER PREVENTION |
REFERENCE |
|
Camellia sinensis |
Green tea |
Theaceae |
Leaves |
Catechin |
Anti-inflammatory |
(15) |
|
Azadirachta indica |
Neem |
Meliaceae |
Seed |
Azadiradione |
Antioxidant |
(16) |
|
Annona squamosa |
Sugar apple |
Annonaceae |
Leaves |
Alkaloids, flavanoids |
Antiulcer |
(17) |
|
Glycyrrhiza glabra |
Liquorice |
Fabaceae |
Roots |
Glycyrrhizitic acid |
Anti-ulcer |
(17) |
|
Embilica officinalic |
Amla |
Euphorbiaceae |
Fruit |
Gallic acid |
Antioxidant |
(18) |
|
Allivum sativum |
Garlic |
Liliaceae |
Bulb |
Alliin |
Antioxidant |
(18) |
|
Bacopa monniera |
Brahmi |
Scrophulariaceae |
Leaves |
Bacosides |
Anti-ulcer |
(18) |
|
Moringa oliefera |
Drumstick |
Moringaceae |
Flowers,fruits,leaves |
Alkaloids |
Anti-ulcer |
(19) |
|
Curcuma longa |
Turmeric |
Zingiberaceae |
Root |
Curcumin |
Antioxidant |
(19) |
|
Aloe vera |
Aloe |
Liliaceae |
Leaves |
Saponin |
Anti-ulcer |
(19) |
|
Carica papaya |
Papaya |
Caricaceae |
Fruit |
Quercetin |
Anti-ulcer |
(20) |
|
Panax ginseng |
Ginseng |
Araliaceae |
Root |
Ginsenoside |
Cytoprotective |
(21) |
|
Mangifera indica |
Mango |
Anacardiaceae |
Leaves |
Alkaloids, flavonoids |
Anti-inflammatory |
(21) |
|
Wuthenia somnifera |
Ashwagandha |
Solanaceae |
Root |
Alkaloids |
Anti-inflammatory |
(22) |
|
Musa paradisca |
Banana |
Musaceae |
Fruit |
Glycosides, tannins |
Anti-ulcer |
(22) |
|
Rheum emodi |
Rhubarb |
Poligonaceae |
Leaves |
Sennosides |
Constipation |
(23) |
MECHANISM OF ANTI-ULCER ACTIVITY:
Antioxidant activity:
Gastric ulcers and oxidative stress are known to be related. It is probably because of their antioxidant qualities that many herbal remedies help with stomach ulcers. Malondialdehyde (MDA) levels in the stomach were elevated whereas superoxide dismutase (SOD) and catalase (CAT) levels were lowered in indomethacin-induced gastric ulcer mice. As effective as misoprostol, piper betel extract treatment not only restored normal MDA levels but also markedly raised SOD and CAT levels.
Encouragement of mucosal growth:
In order to heal ulcers, mucosal proliferation is necessary. Certain herbal remedies that aid in the healing of ulcers work by encouraging the growth of new cells. According to one study, taking Centella asiatica orally for three days boosted the expression of basic fibroblast growth factor and proliferated and angiogenesis. Additionally, seven days of oral ethanol extract of Tabebuia avellanedae boosted cell proliferation in rats with stomach ulcers caused by acetic acid. It is possible that the elevation of epidermal growth factor and its receptor expression is what causes herbal medicine to stimulate cell proliferation.
Inhibition of acid generation:
Gastric ulcers may be improved by inhibiting the generation of acid. Gastritic acid production is decreased by a number of herbal medications that have anti-gastric ulcer properties (Table 1). For instance, taking Ocimum sanctum extract orally for three days reduced overall stomach acidity by more than fifty percent. Similarly, 400 mg/kg of oral Solanum nigrum fruit extract reduced stomach acid concentrations on par with 10 mg/kg of omeprazole. The decrease in acid production caused by herbal medicine may result from either (1) stimulation of prostaglandin E2 production or (2) suppression of H(+)/K(+)-ATPase activity, as shown in animal models of gastric ulcers. (24)
LIMITATIONS OF CONVENTIONAL ANTI-ULCER:
FUTURE PROSPECTS
Growing antibiotic resistance, which lowers the effectiveness of eradication therapy, and abuse of PPIs, which causes unanticipated new side effects, coexist with the global drop in peptic ulcer disease and the incidence of H. pylori [56]. Additionally, the prevalence of idiopathic ulcers linked to high mortality is rising [57], and the best way to treat the idiopathic illness needs to be determined. The optimum course of action for treating people who are at risk for both H. pylori infection and NSAIDs or aspirin is still unknown.
There is still much to learn about the etiology of stomach lesions caused by H. pylori. Although the host immune response and H. pylori virulent factors work together to drive its development, it is still unclear exactly how these variables interact with the host genetic profile. The genetic variants linked to H. pylori-induced peptic ulcers and the reasons why certain patients are more vulnerable than others to the gastrointestinal toxicity of NSAIDs and aspirin are also unknown. Antibiotic resistance remains a significant problem in the lack of any potential breakthrough antimicrobial drug for H. pylori, and new treatments are actually old treatments. The focus of research on developing antiulcer treatments has been on H. pylori urease.
In individuals with peptic ulcer disease, comorbidities are now the leading cause of death, and intestinal bleeding as a consequence is still potentially fatal. Randomized controlled studies and prospective data are desperately needed to determine the optimal patient treatment approach.
As a consequence of peptic ulcer disease, intestinal bleeding is still potentially fatal, and comorbidities are now the main reason why these individuals die. Prospective data and randomized controlled trials are desperately needed to determine the optimal approach to patient care. In order to sustain effective peptic ulcer treatment, H. pylori treatment plans will be required. (25)
RECENT ADVANCES IN ANTI-ULCER THERAPY:
Recent developments in the field of treating Peptic Ulcer Disease (PUD) indicate a move toward more complex and individualized approaches. Helicobacter pylori (H. pylori) elimination techniques have changed throughout time, with customized regimens that take into account the changing antibiotic resistance landscape. This action optimizes treatment results and aims to counteract the declining effectiveness of traditional medicines. The development of the new acid suppressor vonoprazan represents a significant advancement. Vonoprazan shows promise in eliminating clarithromycin-resistant H. pylori strains thanks to its competitive inhibition of gastric H+ /K+ -ATPase. However, long-term use of acid suppressants—whether conventional or novel—introduces possible side effects, including as hypergastrinemia, pneumonia, bacterial overgrowth, and C. difficile infection, which call for careful consideration in treatment planning.
Ongoing research toward a vaccine against H. pylori offers optimism for a ground-breaking advancement in the preventative field. As it continues to improve, this vaccine could be used as a main preventive strategy to lower the prevalence of H. pylori infection and the consequences that come with it. Additionally, research into natural products—particularly monoterpenes generated from medicinal plants—has been prompted by the search for new therapeutic routes. These substances, which have a variety of chemical structures, have antibacterial, healing, and anti-ulcer properties, making them viable substitutes for PUD treatment. The intricacy of properly maintaining PUD is shown by ongoing difficulties, nevertheless. Even while antibiotic resistance in H. pylori is on the decline, it is still a major obstacle. Rates of resistance, especially to clarithromycin, affect how well traditional antibiotic-based treatments work. (26)
CONCLUSION
Herbal products and conventional anti-gastric ulcer medications may work in concert to combat H. pylori and gastric ulcer disease and enhance the prognosis of gastric ulcer patients. It is advised to carry out additional clinical research with larger sample sizes on the effectiveness and safety of medicinal plants with antiulcer activity because there have only been a few human studies. Research on the mechanisms of action of medicinal plants used to treat or prevent peptic ulcers would also be beneficial.
Lastly, licensing is necessary for herbal products used for medical purposes in order to improve their quality and safety and guarantee that demands for their potential efficacy are validated by randomized controlled trials. The issue of inadequate research in this area persists despite the rise in reports of herb-drug interactions, and no action has been taken to solve this issue. Therefore, whether using herbal preparations alone or in conjunction with other herbal or conventional therapies, pharmacists and physicians should be particularly aware of the risks involved.
ACKNOWLEDGEMENT
We would like to thank all those individuals who helped in making this study successful. First of all, we would like to thank our guide Ms. Mohini Patel for all the advice, help, and guidance in this study.
We would also like to thank the head of the department and each member of the faculty for giving us what we needed to finish this task. Each member has been very crucial to the final completion of this project.
REFERENCES





Riturajsinh Parmar, Harshil Desai, Himanshukumar Chauhan, Pruthvirajsinh Gohil, Mohini Patel, Dr Jaswandi Mehetre, A Review on Herbal Plantsused in The Management of Stomach Ulcer, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3348-3357, https://doi.org/10.5281/zenodo.19230868
 10.5281/zenodo.19230868
10.5281/zenodo.19230868
