Raosaheb Patil Danve College of Pharmacy Badnapur, Jalna.
The burden of stroke is strongly affected by ageing. Intracerebral haemorrhage (ICH) has catastrophic effects, and treatment options are limited. ICH has long been considered to be the stroke specific type with the worst diagnosis. Hypertensive Intracranial Haemorrhage is a form of stroke that occurs when an artery in the brain bursts and the blood spreads to surrounding areas. Nonetheless, acute stroke unit care improves outcome after ICH, patients benefit from interventions to prevent complications, acute blood pressure lowering appears safe and might have a modest benefit, and implementing a bundle of high-quality acute care is associated with a greater chance of survival. Chronic arterial hypertension represents the major risk factor for bleeding. The incidence of hypertension-related ICH is decreasing in some regions due to improvements in the treatment of chronic hypertension. Anticoagulant-related ICH (vitamin K antagonists and the newer oral anticoagulant drugs) represents an increasing cause of ICH, currently accounting for more than 15 % of all cases. Although questions regarding the optimal medical and surgical management of ICH still remain, recent clinical trials examining hemostatic therapy, blood pressure control, and hematoma evacuation have advanced our understanding of ICH management.
The possibility of hypertension is the powerful modifiable risk factor for intracerebral haemorrhage, and it rises with age (ICH). The scientific information is essential on common chronic degenerative diseases for specific age group of people.
Hypertensive Intracranial Haemorrhage can be identified as a stroke. This stroke is caused by the brain’s artery breaks out in and spreading of blood and bleeding begins from nearby tissues. Damage of brain cells is caused due to bleeding .
Swelling of brain tissues can be due to blood from infuriation due to trauma and it is called as cerebral oedema. The collection of blood and mass making is called a hematoma. Due to this condition, the pressure increases on surround tissues and essential blood flow decreases and causes permanent damage to brain cells. Intracranial haemorrhage (ICH) is responsible for stroke in the 15% cases with poor outcomes and increased death rate.
Diverse pathology can be the cause for high mortality rate. There is diversity in symptoms of Intracranial haemorrhage. In some cases, the major hemogenic symptoms like trauma, haemorrhagic conversion of ischemic infarction, hypertension, vasculitis, and venous sinus thrombosis have seen.
Nerve symptoms like cerebral amyloid antipathy, cerebral aneurysms, and cerebral arteriovenous malformations can also be faced in some cases of ICH.
Intracranial hemorrhage includes epidural hematoma, subdural hematoma, subarachnoid hemorrhage (SAH), intraventricular hemorrhage (IVH), hemorrhagic transformation of ischemic stroke (HT), venous hemorrhage from cortical vein or sinus thrombosis and intracerebral hemorrhage.1
Spontaneous intracerebral haemorrhage (ICH) refers to non-traumatic bleeding in the brain parenchyma and is the deadliest form of stroke. The high 1-month case-fatality rate of ~40% and poor long-term outcome make it a major contributor to global morbidity and mortality.
Although ICH accounts for a minority of stroke world wide (10–30%), it is associated with a greater burden of disability-adjusted life years than ischaemic stroke, given its high incidence in low- and middle income countries.
Despite dramatic drops in ischaemic stroke mortality rates,3 there has been limited improve ment in case fatality from ICH in the last few decades245and most survivors are left with severe disability.
ICH is not a single entity; 85% of cases are due to cerebral small vessel disease, predominantly deep perforator arterio pathy (also termed hypertensive arterio pathy or arteriosclerosis) and cerebral amyloid angiopathy, while the remainder results from a macrovascular (eg, arterio venous malformation, cavernoma, aneur ysm and venous thrombosis) or neoplastic cause.
Vascular malformations are the most common cause of ICH in young adults, accounting for up to one third of cases.2
Psychosocial, ethnic, and economic factors play a role in the prevalence of cerebral hemorrhage, with ICH being twice as common in low-income and middle-income coun tries compared with high-income countries.
Other identified risk factors for ICH include age (i.e., each decade from 50 years of age is associated with a 2-fold increase in the incidence of ICH) and an elevated alcohol intake.
Etiologies of ICH to always consider include: intracra nial aneurysms (typically presenting as subarachnoid hemorrhage); arteriovenous malformations (ICH is the first presentation of AVMs in 60 % of cases); cerebral venous sinus thrombosis and venous infarction3
Risk Factors for Intracranial Hemorrhage The most common risk factor for IPH is hypertension. Anti platelet and anticoagulant medications also increase the risk of spontaneous IPH.
Cerebral amyloid angiopathy is related to build-up of amyloid proteins in arterial walls, making them more susceptible to rupture. Hemorrhages due to cerebral am yloid angiopathy are typically lobar (near the cortex), multiple, and occur in patients at least 55 years of age.
The rupture of an intracranial aneurysm (SAH) may be spon taneous, precipitated by exertion, or from hypertension. About 1 2% of the adult population harbors an unruptured intracranial aneurysm, but only about 1% of these rupture, and how best to select patients for prophylactic aneurysm obliteration is unset tled .
The most important modifiable risk factors are tobacco use, hypertension, and cocaine use ; nonmodifiable risk factors include a personal history of SAH, familial history of SAH , larger aneurysm size , female sex , connective tissue disease, and older age.
Arteriovenous malformations are often congenital and may become symptomatic later in life.4
EPIDEMIOLOGY
Since the 1980s, the incidence of ICH-related hospitalizations in the United States has largely remained stable at around 20 per 100,000 persons per year,3, 6 but global incidence increased 47% between 1990 and 2010, primarily driven by low-income countries.
In high income countries, despite improved hypertension management, it is hypothesized that overall incidence has remained stable due to increased use of antithrombotics, resulting in more anticoagulant-related ICHs.8
This idea is supported by a study investigating the incidence of ICH in Cincinnati from 1988 through 1999.
This may in part be due to improved access to imaging and a five-fold increase in anticoagulant-associated ICH during the 1990s.9 ICH is more common in men, occurs more frequently in the winter months, and incidence increases with age.
In-hospital mortality following ICH decreased between the 1970s and 1980s, but has since remained roughly stable around 35–40%.3, 6 One study investigating both early and late case fatality found that from 1985 to 2011 30-day case fatality fell from 40–33%, while 48-hour case fatality did not change.11
Longer-term case fatality rates at 1 year and 5 years remain high with rates of roughly 55% and 70%, respectively.8, 12 Population-based studies of ICH in different racial and ethnic groups have consistently found a higher incidence of ICH in Blacks and Hispanics in the U.S. population when compared to whites.
Incidence of ICH in whites increases with age, while this age-related difference does not occur in Blacks.13 The increased incidence of ICH in Blacks and Hispanics is attributed to more hypertension in these populations.
Additionally, in-hospital and 30-day mortality are higher in Blacks, and young and middle-aged patients are more commonly affected.
Internationally, the incidence of ICH and the proportion of ICH out of total stroke burden in Japan is nearly 40%, more than twice that in Western countries,8, 16 although case-fatality is lower.5
MATERIALS AND METHODS
The study was done in the setting of tertiary hospital, Department of Neurosurgery at Vijayanagar Institute of Medical Sciences (VIMS), Bellary, Karnataka, India, during the period of June 2013 to January 2015.
Depending on the size, loca tion, and etiology of hematoma, some of the patients were treated by surgical evacuation of the hematoma, excision of the tumor, and other patients were treated conservatively.
Among the selected patients, the clinical profile, operative details, and the surgical interventions were undertaken and the outcome was noted.
All patients were followed for 3 months to assess the clinical outcome. Clinical variables included age at the time of pres entation, sex, etiology, location of the hematoma, and the GCS scoring.
Outcome variables included survived (improvement in the GCS), death, and vegetative state or severely disabled.
The outcome variable was compared with respect to age, sex, GCS, etiology, location of the hematoma, and the modality of treatment to find out any statistically significant difference in the rate of outcomes.
Statistical Analysis All the collected data variables were entered into an excel sheet and later transferred to and analyzed using Statistical Package for the Social Sciences software version 22. Appropriate descriptive statistics like percentages/ proportions were used to describe the data variables.
Appropriate tests of significance were applied to know the difference in the rate of outcomes between the groups (chisquare test, Fisher’s exact test), and pvalue.6
CLINICAL MANAGEMENT OF INTRACEREBRAL HAEMORRHAGE
Management of ICH is a complex and multidisciplinary process that begins with patient contact either on the field or in the emergency room.
For completeness of the review, we will touch upon most medical and surgical aspects of management as a key for the practicing intensivist to refer to original trials and research in the field.
As a true neurological emergency, ICH patients are best managed in a dedicated neurocritical care or stroke unit for at least the first 24 to 48 hours as this has been shown to reduce the likelihood of mortality,34 and a Swedish cohort showed that these units were associated with better longterm survival.35
This acute period is usually associated with rapid deterioration because of hematoma expansion, intraventricular extension, and uncontrolled HTN.7
NEUROLOGICAL OUTCOMES
The most common complication in surviving infants is motor impairment, seen in 22/ 80 (28%) of those without clear evidence of parenchymal hemorrhage, and 35/47 (75%) with PVHI and 12/13 (92%) with IPH.
Many studies on isolated GMH-IVH have reported mild motor impairments (e.g., transient tone abnormalities, dyspraxia), whereas more severe impairment (e.g., cerebral palsy) may occur in parenchymal hemorrhage.
The location and extent of parenchymal hemorrhage tends to correlate with the topology of motor impairment16; however, the relationship between fetal MRI findings, timing of hemorrhage, and the degree of functional motor impairment is not known.
Cerebral palsy was reported in 2/ 16 (13%) cases of cerebellar hemorrhage in the meta-analysis by Sileo et al.,44 and there were no cases of motor impairment in a more recent single-center cohort.8
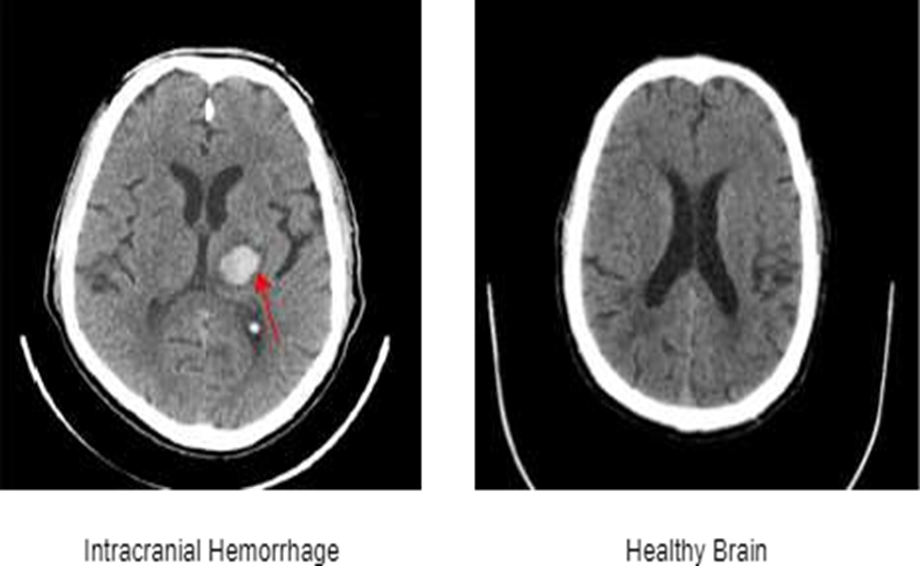
Fig. 1. Sample images of CT scan with Intracranial Hemorrhage (marked with red arrow) and Healthy Brain.
Intracranial Brain Hemorrhage comprises five types, named as, epidural hemorrhage, subdural hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage, and intraparenchymal haemorrhage.9

Fig. 2. Types of hemorrhages: (From Left to Right) Intraparenchymal, Intraventricular, Sub- arachnoid, Subdural, Epidural. Source.9
GENERAL SUPPORTIVE THERAPY
Anticoagulation Reversal and Resumption of Antithrombotic Therapy in ICH
ICH presents a substantial clinical challenge, particularly in anticoagulation reversal and the resumption of antithrombotic therapy [124].
Prompt reversal of anticoagulation in patients with ICH is crucial, as delays are associated with increased HE and mortality rates, especially among older individuals.
(INR) to below 1.3 within 4 h of admission correlates with lower HE rates and improved outcomes. The choice of reversal agent depends on the anticoagulant used. For patients on vitamin K antagonists, prothrombin complex concentrates and intravenous vitamin K are recommended to quickly restore INR levels.
In contrast, specific reversal agents such as idarucizumab for dabigatran and andexanet alfa for factor Xa inhibitors are effective for patients on direct OACs.
However, limited availability and high costs of these agents remain barriers in some clinical settings. Current evidence supports the feasibility and effectiveness of resuming antithrombotic therapy (anticoagulation or antiplatelet therapy) after ICH, regardless of hemorrhage location or the presence of microbleeds.
For instance, the RESTART trial suggests that resuming antiplatelet therapy post-ICH does not significantly increase the risk of recurrent hemorrhage and may reduce the occurrence of major vascular events.
Achieving a balance between preventing thromboembolic events and minimizing the risk of recurrent hemorrhage 14 of 40 MedComm, 2025 requires careful consideration of factors such as timing, the type of anticoagulant, and patient-specific characteristics.10
BP Management
Compared with patients with subarachnoid hemorrhage (SAH), those with spontaneous ICH often exhibit a more complex and multifactorial hypertensive response that is less reliant on catecholamines .
Numerous studies emphasize the importance of early and aggressive BP control in reducing HE and improving clinical outcomes.
The INTERACT2 trial is a landmark study demonstrating that intensive BP reduction is associated with improved functional outcomes at 90 days and tends to reduce mortality rates and severe disability.10
SIGN & SYMPTOMS:-
DIAGNOSIS
Rapid diagnosis is critical for a positive outcome.
TREATMENT
NEED OF WORK:-
Systematic reviews are necessary to clarify optimal approaches for treating brain hemorrhage
Reviewing studies on diagnostic techniques like CT scans and advanced MRI can assess their effectiveness and identify areas for improvement.
While primary injury from the initial bleed is unavoidable, secondary brain damage from factors like inflammation, oxidative stress, and swelling occurs over days to weeks.
Reviews can advocate for the use of more comprehensive outcome measures that better reflect functional recovery and patient-reported outcomes. This includes incorporating cognitive assessments, which are often overlooked.
Many promising therapies show success in preclinical animal models but fail in human trials. Reviews are needed to analyze these discrepancies and improve the translational process.
AIM:-
The aim of brain hamorrhage to provide a comprehensive, critical analysis of existing research on a specific aspect of brain hamorrhage.
OBJECTIVES:-
CONCLUSION:-
Brain hemorrhages are an extra complication that trauma patients—especially those over the age of 55—experience when using antiplatelets and anticoagulants.
The current study shows that these drugs come with an additional cost in the form of extra hospital and ICU days, return visits after release, intracranial bleeding requiring neurosurgical intervention, and hospital and mortality within three months.
Because of this, trauma patients who experience head injuries should be seen as having a high risk factor for antiplatelet and anticoagulant use in the past.
About half of these hemorrhages are caused by hypertension; the remaining ones are brought on by vascular malformations, tumours, aneurysms, inflammatory and degenerative vasculopathies, and hematologic and iatrogenic coagulation abnormalities.
In certain cases, the cause is never identified. Depending on where it occurs, hypertensive brain hemorrhage in the deep gray nuclei of the hemispheres, the cerebellum, and the pons causes distinct clinical symptoms.
In cases of lobar and putaminal hemorrhages, surgical hematoma removal is recommended if the patient's condition worsens despite receiving intensive medical treatment.
Furthermore, the majority of severe cerebellar hemorrhages (>3 cm) and smaller hemorrhages that cause a notable compression of the brain stem should be assessed. More research is required to determine how immediate surgery, elective late surgery, and intense medical care affect final functional outcomes
SUMMARY:-
Brain hemorrhage is a severe stoke subtype caused by a ruptured blood vessel, leading to bleeding into the brain tissue ( intracerebral hemorrhage ) or the surrounding space (subarachnoid hemorrhage).
Key risk factors include uncontrolled high blood pressure, vascular malformation, and certain medications like anticoagulants.
Rapid diagnosis with CT scans or MRI is essential, followed by prompt treatment including blood pressure control, reversal of anticoagulation and potential surgical damage and improve outcomes.
A brain hemorrhage is a life-treatening condition where a blood vessel ruptures and bleed within or around the brain. It is type of hemmorrhagic stroke and can lead to severe disability or death.
In this review, we focus on the current standard of care of acute ICH and discuss emerging therapies that may alter the landscape of this devastating disease.
Spontaneous brain hemorrhage accounts for about 10% of all strokes and is fatal in about 50% of the cases.
Its incidence, in contrast to other types of strokes, has not declined.
Hypertension accounts for about half of these hemorrhages; the rest are due to tumors, aneurysms and vascular malformations.
Inflammatory and degenerative vasculopathies and hematologic and iatrogenic disorders of coagulation.
In some patients no cause is ever found. Hypertensive brain hemorrhage occurs in the deep gray nuclei of the hemispheres, the cerebellum, and the pons and results in specific clinical syndromes depending on the location
FUTURE SCOPE:-
REFERENCES


Suchita Lathi, Pallavi Shinde, Pawan Hanute, Komal Pawar, A Review on Brain Hemorrhage, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1214-1224. https://doi.org/10.5281/zenodo.18231401
 10.5281/zenodo.18231401
10.5281/zenodo.18231401
