Rungta Institute of Pharmaceutical Sciences and Research, Kokha, Kurud, Bhilai, Chhattishgarh-490024, India.
Insufficient production of the brain chemical dopamine by brain cells leads to Parkinson's disease (PD), a type of movement disability. Environmental exposure may be a contributing factor, although most cases do not seem to run in families, however it can occasionally be inherited. Parkinson's disease (PD) symptoms include tremor of the hands, arms, legs, jaw, and face; stiffness of the arms, legs, and trunk; slowness of movement; poor balance and coordination; and eventually, depression, difficulty sleeping, or trouble speaking, chewing, swallowing, or speaking as symptoms develop. It may be difficult to diagnose PD because it cannot be tested in a lab. Doctors consider a patient's neurological status and medical history when making a diagnosis. PD usually appears around age 60, though it can begin sooner. It is more common in men than in women. There is no recognized cure for PD. Sometimes, a variety of drugs can greatly lessen symptoms. Deep brain stimulation (DBS) and surgery may be beneficial in extreme situations. During DBS, electrodes are surgically placed inside the brain. They send electrical pulses to the parts of the brain that control movement.
People of many races and cultures are affected by Parkinson's disease (PD), which is estimated to afflict 6.3 million people globally. A part of the brain is impacted by Parkinson's disease, a chronic, persistent illness. It bears the name of the doctor who first described it. In 1817, James Parkinson wrote the first description of Parkinson's disease [1–4]. Parkinson's disease is a degenerative neurological condition that makes it harder for a person to control their movements and gets worse with time. It mostly affects how the brain synchronizes the movements of the muscles in various body parts. It is not contagious or lethal. It is thought to be hereditary in a very small percentage of instances [5]. PD usually appears around age 60, though it can begin sooner. "Early onset" Parkinson's disease, which begins before the age of fifty, affects five to ten percent of individuals. Early-onset types of Parkinson's disease are often inherited, although not always, and have been linked to certain gene alterations. Although it can also affect younger people, men are more likely than women to be affected by Parkinson's disease by more than 50%. This is known as Young Onset Parkinson's disease [5–6]. As Parkinson's syndrome progresses, these non-motor indications develop problematic. Pharmaceutical treatment is now the keystone of managing Parkinson's disease (PD); then, these indicative actions consume important drawbacks popular cases of severe illness. Advanced trendy the virus's development, a number of incapacitating features arise, such as per non-motor indications, dopamine-resistant motorized indications, and motorized lateral belongings afterward lengthy dopamine treatment. Despite notable progress in the medicinal then clinical organization of Parkinson's disease, here stays now no proven disease-modifying medication. However, scientists are optimistic that they may be able to pinpoint possible disease-modifying targets. This review will cover the mechanism, diagnosis, clinical characteristics, epidemiology, and medicinal and surgical treatment of Parkinson's disease. Experimental treatments won't be covered here because they have only produced a small number of test findings thus far.
History
Dr. James Parkinson 1817 "An Essay on the Shaking Palsy" by English physician Dr. James Parkinson was the first to describe Parkinson's disease. He described the symptoms of what is now called Parkinson's disease in this study, such as bradykinesia, stiffness, and tremor. The condition was known as "shaking palsy" by Parkinson (Parkinson, J. 1817). Limited Knowledge in the Early to Late 19thCentury When Parkinson first described the condition, it was thought to be "shaking palsy," and little was known about it. Though few advances were made in the study of its origin or treatment during this time, researchers continued to record instances. Dr. Konstantin Tretiak off in 1912 One important discovery was made by Russian neurologist Dr. Tretiakoff, who connected Parkinson's disease to the degeneration of the substantia nigra, a part of the brain that produces dopamine. This finding was a turning point in our biological understanding of Parkinson's disease. 1940s: Dopamine and Neurotransmitters' Function Studies conducted in the 1940s established that dopamine depletion, a neurotransmitter essential for motor function, is a hallmark of Parkinson's disease. This clarified the motor symptoms associated with Parkinson's disease. The foundation for medical advances in our understanding of Parkinson's disease was laid throughout this time. 1950s Levodopa’s (L-DOPA) discovery. In the 1950s, levodopa (L-DOPA) was identified as a Parkinson's disease medication. In the brain, levodopa is changed into dopamine, which helps to reduce Parkinson's disease's movement symptoms. Its application transformed PD treatment. 1980s: DBS, or deep brain stimulation. Deep brain stimulation, or DBS, has become a surgical treatment for Parkinson's disease symptoms. To lessen motor symptoms, including tremors, DBS entails activating electrodes that are implanted in particular brain areas. Parkinson's Disease Foundation,1997 In order to promote research and educate people about Parkinson's disease, the Parkinson's Disease Foundation now known as the Parkinson's Foundation was founded. 1990s Genetic Findings Research on genetics started to pinpoint particular mutations linked to Parkinson's disease, most notably the identification of mutations in the alpha-synuclein gene, which is present in uncommon family cases of the condition. Understanding the disease's sporadic and hereditary forms was made possible by this.
Causes Of Parkinson Disease
There is currently no recognized reason or explanation for why someone gets Parkinson's disease. Although there are numerous ideas regarding the causes, it is generally accepted that a number of elements are at play. The cause of dopamine destruction is yet unknown to medical professionals. generating nerve cells or the factors that brand about persons additional liable to Parkinson's sickness than others [7]. Numerous studies trust that the disease might vary from person to person and be brought on by a mix of environmental and genetic variable star. But Parkinson's illness is non-infectious and is not a communicable condition [8].
Genetics
Numerous genetic changes, or mutations, have been demonstrated to raise an individual's risk of developing Parkinson's disease, while it is unclear how precisely these make certain people
Parkinson's disease is rare, more vulnerable to condition. but it can run in families if a child inherits the disorder from their parents because of faulty genes. Recent advances in genetic research have identified mutations in a number of pathogenic genes, including SNCA, Parkin, UCHL1, DJ-1, PINK-1, LRRK2, and ATP13A2, which result in family versions of Parkinson's disease (PD) [9,10].
Environmental
Environmental variables may potentially raise an individual's chance of Parkinson's disease, according to some experts. It has been proposed that the illness may be exacerbated by industrial or traffic pollution, as well as pesticides and herbicides used in agriculture. Nevertheless, there is conflicting evidence that environmental variables contribute to Parkinson's disease. Farming, pesticide exposure, drinking well water, and a history of head trauma are some of the possible environmental risk factors [10,11].
Other causes of Parkinsonism:
Additional causes of Parkinson's disease: The general term for the symptoms of tremors, muscle rigidity, and slowness of movement is "parkinsonism." Although Parkinson's disease is the most prevalent form of Parkinsonism, there are other, less common forms for which a particular etiology can be found [10]. Among these are Parkinsonism brought on by:
Medication (also known as "drug induced Parkinsonism"): a condition in which symptoms appear after taking specific drugs, such as some antipsychotics, and typically go away after stopping the treatment. Additional progressive brain disorders include corticobasal degeneration, multiple systems atrophy, and progressive supranuclear palsy. A cerebral infarction occurs when a major stroke results in the death of many brain regions.
Parkinsons Symptom
Both motor and non-motor symptoms are common in Parkinson's disease. However, not every PW experiences every symptom, and each person experiences symptoms to varying degrees. Numerous more symptoms are taken into account during the diagnostic process in addition to these four cardinal motor signs. The non-motor symptoms are frequently more difficult for Parkinson's patients to manage. Parkinson's disease patients may also experience nonmotor symptoms that affect their daily lives, such as pain, sadness, memory loss, and sleep issues [2, 4,12,13]. Physical movement is impacted by the four primary symptoms of Parkinson's disease:
Tremor: Unilateral, usually resting tremor in body parts, usually in the upper extremities, is the most prevalent sign of Parkinson's disease. However, as the disease progresses, this discovery may spread to other body regions such as the lips, chin, jaw, and tongue. About 70% of persons who present with Parkinson's disease have this early symptom. Parkinson's disease tremor is a rest tremor, meaning that the shaking happens when the patient is not attempting to use the limb and goes away when they do. Tremor may be the symptom that responds the least to dopamine replacement therapy since it is linked to an imbalance of the neurotransmitter’s dopamine and acetylcholine. This is more likely to happen when the limb is at rest and commonly starts in the hand or arm [14,15].
Bradykinesia: which includes slowness, dysrhythmia, and decreased movement amplitude, can be the most incapacitating sign of the disorder. Physical motions are significantly slower than usual, which can make daily chores challenging and cause a characteristically slow, shuffling gait with tiny steps [16,17,18,19].
Stiffness (rigidity) of the muscles: Parkinson's disease may cause the tendon to become more tense, which may cause structural adjustment and a rise in tendon stiffness. Parkinson's patients may not notice muscle rigidity, but a doctor can detect it in limb muscles when they are manipulated passively. Tension and stiffness in the muscles can cause severe cramping (dystonia) and make it hard to move and form facial expressions [16,20,21].
Postural instability: One of the most incapacitating aspects of Parkinson's disease is postural instability. A sign of the advancement of the disease, postural instability is frequently encountered in the latter stages of Parkinson's disease. The function of visual cues as an adaptation strategy to offset postural instability in Parkinson's disease is not well understood. Gait abnormalities and postural instability frequently appear later in the course of the illness. Early falls due to a loss of postural reflexes are not indicative of typical Parkinson's disease. One crippling aspect of Parkinson's disease (PD) is postural instability, which increases the risk of falls and injury from them. A modest flexion of the neck or trunk with a slight tilt to one side may be seen in the posture of those with early-stage Parkinson's disease [22,23]. Anosmia, anxiety, constipation, depression, exhaustion, speech impediments, postural hypotension, and micrographic are additional symptoms [24].
Parkinson's disease progression: Parkinson's disease is a neurological condition that worsens gradually over time. As Parkinson's disease worsens, symptoms typically start on one side of the body and move to the other. Estimating the rate of advancement is challenging because each person with Parkinson's disease may have unique symptoms. As Parkinson's disease progresses, symptoms that were already there may get worse and new ones may emerge. Unfortunately, medications do not slow the progression of Parkinson's disease; they only help manage its symptoms.
Early Parkinson's: The symptoms of Parkinson's disease might be moderate in the early stages and make it difficult to do fine motor tasks like tying shoes or buttoning shirts.
Function Of Parkinsons Disease
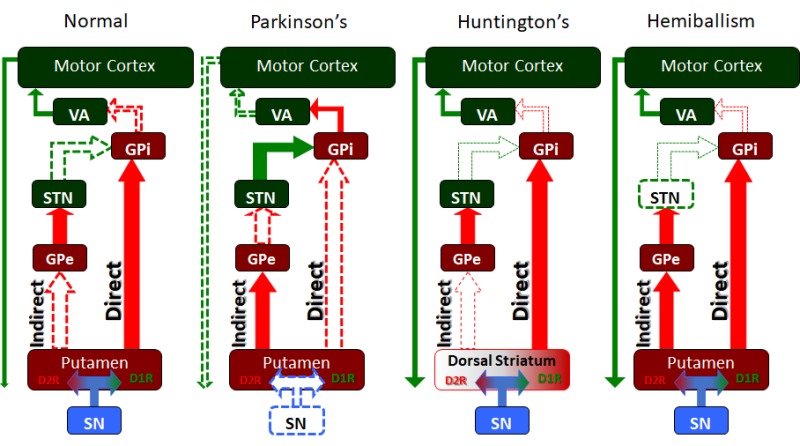
Among its various roles, the basal ganglia are particularly involved in "disinhibiting" or releasing motor action. These sped-up circuit diagrams show how the different basal ganglia nuclei and pathways work together in healthy people and people with a number of extrapyramidal motor diseases, like Huntington's disease, Parkinson's disease, and hemiballismus.
Parkinson's Diagnosis
Parkinson's disease is difficult to diagnose. Since there are no laboratory tests (like a blood test or brain scan), an expert, like a neurologist, must make the diagnosis. The expert will take a thorough history of the patient's symptoms and check for any outward manifestations of Park disease [7]. Parkinson's disease is frequently hard to diagnose, and early warning signals are overlooked. Starting therapy and living a healthier life would be much easier with early detection. The symptoms that occur during the early stages of Parkinson's disease are listed below. It is not necessary to be concerned right away if you only have one of the symptoms below. Nonetheless, if you experience two or more of the following symptoms: slouched posture, slowed and stiff motions, tremor, frozen shoulder, altered voice, facial masking, sleep difficulties, small, crammed handwriting, and loss of smell or anorexia. Making an appointment with a neurologist would be wise [8]. There is currently no reliable biological test or radiological approach to diagnose Parkinson's disease, and autopsy-based research has revealed that even among neurologists, up to 25% of cases are found to be erroneous at the time of death [7].
The clinical picture of four cardinal symptoms and a favourable response to levodopa remains the basis for the provisional medical diagnosis of Parkinson's disease, notwithstanding advance in treatment. Bradykinesia, muscle rigidity, postural instability, and tremor make up the diagnostic check list of symptoms [25].
Diagnostic Investigations: Brain scans may lessen misdiagnosis by identifying dopamine depletion in the brain. Possible neuroimaging techniques include:
MRI Scan (Magnetic Resonance Imaging): This produces images of the brain using magnetic currents. This provides a clearer picture of the brain's deep structures. Although MRI scans are typically normal in Parkinson's disease, they can occasionally be helpful in finding disorders that can mimic the disease and in differentiating Parkinson's from other types of Parkinsonism, such as Multiple System Atrophy (MSA) or Progressive Supranuclear Palsy (PSP). [26,27].
CT scan (Computerized Tomography): An anatomical image of the brain is provided by a sequence of X-rays that are transmitted through various directions. This aids in ruling out blood disorders and brain malignancies that may resemble Parkinson's. Although computerized tomography (CT) does not show any alterations associated with Parkinson's disease, it can rule out structural abnormalities that could cause symptoms similar to Parkinson's [28,29].
Dat Scan (Dopamine transporter Scan): A Dat scan, an imaging method that has been FDA-approved since 2011, aids in taking pictures of the brain's dopamine system. This involves injecting the body with a radioactive tracer, which attaches itself to neurons that release dopamine. Specialized cameras then record the signals. Parkinson's disease is supported by a low signal, or an aberrant DAT scan, which shows that there are fewer dopamine-producing neurons. Additionally, Dat scans can be utilized to distinguish between essential tremor And Parkinson's disease.
It should be mentioned, nonetheless, that a clinical examination is required in addition to a Dat scan, which cannot be used alone to diagnose Parkinson's disease.
Metaiodobenzylguanidine (MIBG) scan: MIBG uptake might offer a special chance to identify extremely early Parkinson's disease in situ during a preclinical window. To aid in the differential diagnosis of Parkinson's disease, associated Lewy Body Disease, and a collection of disorders referred to be Parkinson's Plus, a metaioabenzylguanidine scan may be prescribed [30,31].
Neuropathophysiological
Brain regions associated with movement
Understanding the sequence of biochemical events in the brain that control movement is crucial since Parkinson's disease (PD) primarily affects movement [35] (Fig. 4). In particular, the striatum, the internus and externus globus pallidus (GPi/GPe), the thalamus, and the substantia nigra (SN), which is divided into the substantia nigra pars compacta (SNpc) and the SN pars reticularis (SNpr), are involved in restricting undesired movement and regulating voluntary movement. Despite using the same brain regions, the direct and indirect pathways' activities are divided into restraining involuntary movements and boosting voluntary movement, respectively, due to the distinct molecular reactions involved. The SNpc releases dopamine into the striatum through neuronal projections, stimulating the D1 dopamine receptors for conscious and proprioceptive motion (Fig. 5). When the striatum is activated by excitatory glutamatergic D1 receptors, the neurotransmitter γ-aminobutyric acid (GABA) is released, which inhibits the function of both the GPi and the SNpr. The thalamus can then use its corticospinal projections to send stimulatory signals to the motor cortex and start movement because these two structures' ability to inhibit the ventral anterior and lateral thalamic nuclei with their own GABA secretions is compromised [33]. Similar to the SNpc, the indirect pathway starts with the striatum's inhibitory D2 dopamine receptors to limit excessive or erratic movements. This triggers the release of GABA to the GPe, which then releases more GABA to decrease glutamate signals sent to the SNpr and GPi from the subthalamic nucleus (STN). Since the SNpr and GPi cannot be inhibited by the STN, they can inhibit the thalamic nucleus and, consequently, the motor cortex, which stops motion [34]. Given that both processes start with the SNpc secreting dopamine, it is clear that issues controlling movement would be an obvious result of a condition like Parkinson's disease (PD) when this pathway is disrupted.
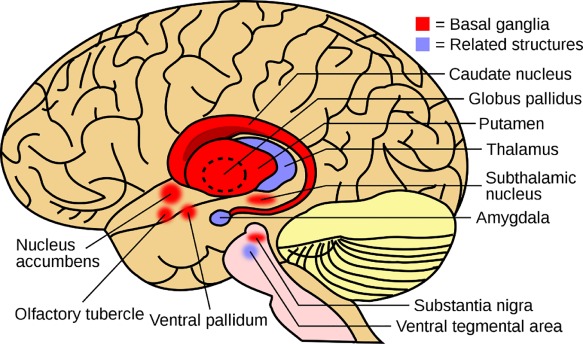
Figure 4. Neuroanatomy of The Brain Regions Associated with Movement (Creative Commons).
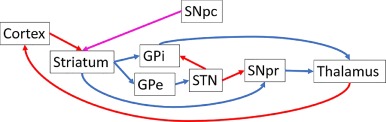
Figure 5. Flowchart of brain regions involved in motion (red = glutamatergic, blue = GABAergic, and magenta = dopaminergic) . (creative commons).
Treatment
Pharmacologically, this is usually levodopa (when paired with carbidopa, which enhances CNS absorption and reduces adverse effects). Younger people may be started on a dopamine agonist (Pramipexole, Ropinirole); these medications have fewer adverse effects but may not be as successful as levodopa. If tremor is the main symptom that needs to be managed, anticholinergics or amantadine may be utilized. Selegiline can relieve minor symptoms and is frequently used to treat early illness. For three to six years, the majority of antiparkinsonian drugs effectively control symptoms. Following this time, the illness worsens and frequently becomes resistant to treatment. Younger patients should generally receive more vigorous treatment than elderly individuals. When it comes to managing Parkinson's disease, a multidisciplinary approach is crucial. When an organized physical therapy program tailored to Parkinson's disease (PD) is used, patients perform significantly better; they can learn how to maintain an active lifestyle, increase their stability, and enhance their gait and balance. Some of this movement disorder's special characteristics have been used to its benefit; patients benefit from music therapy in boxing, cycling, and physical fitness programs. People who are unable to walk might be able to dance. Psychosis, paranoia, REM sleep disturbance, depression, constipation, and caregiver fatigue are frequently observed. All of them must be treated, whether they are drug side effects or a component of the underlying illness. Individuals who respond well to pharmaceutical treatment may eventually become resistant, experience debilitating dyskinesia as a side effect, or experience sudden on/off motor symptoms. Changing levodopa's pharmacokinetics, such as using a continuous GI pump infusion version or more recent delayed-release formulations, has occasionally been beneficial. The patient may be significantly impacted by the addition of other drugs and by the timing of the medicine. Deep brain stimulation techniques are becoming more widely available to regulate the balance of excitatory and inhibitory impulses to the globus pallidus or subthalamic nucleus for certain patients who do not respond to all measures. It is yet unclear why this has such a good impact on PD therapy failures, but it is a field that is actively making progress and offers advanced PD patients new hope. [32,33,34] Psychiatric, autonomic, and sensory symptoms are nonmotor and far more difficult to control. Due to the possibility of adverse reactions and drug-drug interactions, just adding more medications to the patient's regimen is not the solution.
The following are current recommendations: Levodopa for period limb movements during sleep; Sildenafil for erectile dysfunction; Modafinil for daytime somnolence; Polyethylene glycol for constipation; Methylphenidate for fatigue; Cholinesterase inhibitors for dementia; SSRIs for depression; and antipsychotics and pimavanserin for psychotic symptoms.
Cognitive behaviour therapy is used to treat impulse behaviours, and SSRIs are used to treat anxiety. Because deep brain stimulation is reversible, does not harm brain tissue, and can be modified as the disease worsens, it has emerged as the preferred surgical technique. The STN, globus pallidus interna, and thalamus are all stimulated during DBS. DBS is not without complications, though; it is extremely costly, and its long-term advantages are still up for debate.
There is more proof that exercise can enhance flexibility, balance, and gait. Sadly, the benefits of exercise are short-lived, and there is a significant danger of falls.
Some patients may benefit from speech therapy.
Putative disease-modifying therapies for PD.
An expanding number of drugs are being considered for their ability to influence the pathogenic processes of PD. These include novel agents and technologies, such as active and passive immunisation and RNA interference techniques to limit the propagation, and synthesis, of α-synuclein. Additionally, several drugs used for other conditions are of interest for potential use in PD given their ability to influence pathways such as the lysosome–autophagy system, mitochondrial function, and neuroinflammation, for example. Abbreviations: α-syn, α-synuclein; ASO, anti-sense oligonucleotide; GCase, glucocerebrosidase; PD, Parkinson’s disease; RNA, ribonucleic acid; UDCA, ursodeoxycholic acid.
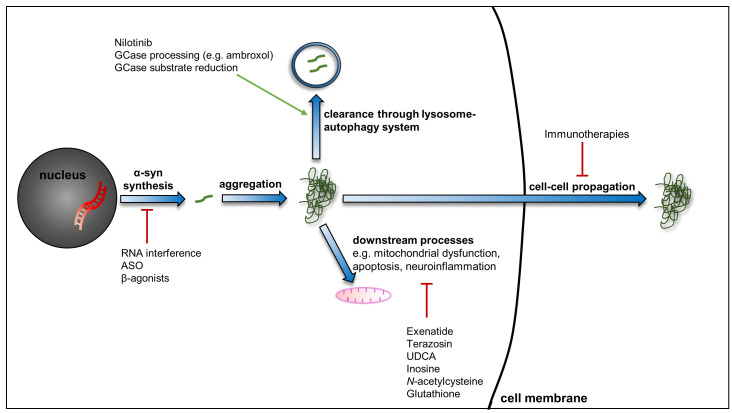
Figure 1. Putative disease-modifying therapies for PD
Therapy for Motor Symptoms
Dopamine is the main component of pharmacological treatment for Parkinson disease motor indications (Table 1). Monoamine oxidase-B (MAO-B) inhibitors, dopamine agonists, and levodopa preparations are effective first treatments. 43 Anticholinergic drugs, such as trihexyphenidyl, are helpful for young people with noticeable tremor, but care must be taken because of the possibility of side effects, especially those related to cognition. Over 40% of patients on oral dopamine agonists (ropinirole, pramipexole) suffer from impulse control disorders, such as compulsive spending, gambling, compulsive medicine use, aberrant eating and sexual activities, and hobbyism. 46Fifteen to twenty percent of people who stop using dopamine agonists—often as a result of impulse control disorders—experience withdrawal symptoms, such as anxiety, panic attacks, irritability, diaphoresis, pain, and drug cravings. Because of this, dopamine agonists can occasionally cause major side effects including impulse control disorders that make it impossible to stop using them. Choosing the best course of action for beginning Parkinson disease treatment necessitates discussing advantages and disadvantages with the patient. Although using levodopa increases functional improvements, it also increases the risk of dyskinesia, especially at larger doses. Infrequently, severe dyskinesias occur. 40 Dopamine agonists and MAO-B inhibitors are linked to a higher overall risk of adverse events, while dopamine agonists are linked to less strong symptom alleviation but a reduced risk of dyskinesia. 45 In the end, the majority of people with Parkinson's disease take drugs from many classes in order to achieve complementary benefits while avoiding excessive dosages and dose-related side effects.
Advanced Therapies for Motor Symptoms
To determine enduring suitability, transmit available the events, then supervise nonstop medication and expedient optimization (e.g., software design inspiration bounds in deep brain stimulation or titrating dosing of the enteral postponement), field centre assessments are necessary for deep brain stimulation, MRI-guided focused ultrasound, and treatment with levodopa-carbidopa enteral suspension. For those with Parkinson's disease who have motor symptoms that reply to treatment but have side effects such dyskinesias or off periods that don't improve with drug changes, these methods can be helpful. Medication-refractory tremor can be pointed with deep brain stimulation and targeted ultrasound that targets the thalamus. Age (75 years), cognitive damage (especially dementia), and the existence of levodopa-unresponsive symptoms (e.g., gait, balance instability) are characteristics linked to poorer deep brain motivation results. 64 Connected and questionnaire-based screening methods can assist in determining and ordering suitable individuals for deep brain inspiration. 65,66 An expert multidisciplinary side's valuation and conversation of likely dangers and benefits, medical strategy, brain target selection, and drug and stimulation optimization are the maximum successful program methods.
CONCLUSION
One of the most dominant neurodegenerative sicknesses moving the old people, Parkinson's disease is linked to higher rates of morbidity and mortality. The optimization of the cases needs the consciousness of the project arrivals, the actions, and the liberal lasting sequence of the design. Parkinson's illness has no recognized cure, although there are drugs that can help manage its symptoms, and research is being done to develop new ones. Gene therapy is one such treatment that can stop brain cell loss by introducing healthy genes straight into your brain. Another is looking into the possibility of replacing nerve cells that are lost in Parkinson's disease affected role. There are innumerable different hypotheses about what causes Parkinson's disease, but most people agree that a mixture of mutable stellar is to blame substituted by new, strong lockups complete after stalk lockups refined in a lab.
REFRENCES


Payal Sahu*, Mayur Hirve, Anshika Singh Chauhan, Enti Srivalli, Suchita Wamankar, Dr. Gyanesh Kumar Sahu, A Review of Parkinson Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 1669-1681. https://doi.org/10.5281/zenodo.15046154
 10.5281/zenodo.15046154
10.5281/zenodo.15046154
