Samarth College of Pharmacy, Belhe, Pune, Maharashtra, India-412410
The existence of kidney stone disease is among the oldest illnesses identified by medicine; little is understood about the mechanisms behind the development and production of stones. Due to recent technological advancements, many ideas and techniques have been created and applied in the surgical management of kidney stones over the past few decades. The authors and other research groups' observations point to five distinct primary pathways for kidney stone production. Intrarenal crystal precipitation is caused by urine supersaturation and crystallisation. The production of calcium oxalate stone is known to have originated from Randall's plaques. Sex hormones may play a significant role in the development of nephrolithiasis, making them possible targets for novel medications that prevent the creation of kidney stones. Because of its metabolic output and other contributions, the microbiome, which includes urease-producing bacteria, nanobacteria, and intestinal microbiota, is anticipated to have a significant impact on urological health, both positively and negatively. Finally, renal calcium oxalate crystal production is significantly influenced by the immunological response, namely macrophage differentiation. The current understanding of each of these five features of kidney stone production is reviewed in the current study. Urologists, nephrologists, and primary care physicians can use this information to investigate new research avenues and enhance their comprehension of the onset and progression of kidney stones.
Kidney stone disease, also known as nephrolithiasis or urolithiasis, is one of the oldest diseases known to medicine. It is estimated that 1?15% individuals suffer from kidney stone formation at some point during their lifetime, and the prevalence and incidence of kidney stones is reported to be increasing worldwide [1,2]. A recent study concluded that the prevalence of kidney stones was 5.8% among Chinese adults [6.5% in men and 5.1% in women], with about 1 in 17 adults currently affected [3]. Without proper treatment, kidney stones can cause the blockage of the ureter, blood in the urine, frequent urinary tract infections, vomiting or painful urination, culminating in the permanent functional damage of the kidneys [4]. The worldwide prevalence of urolithiasis has increased over the past decades. [4] Over the past few decades, urolithiasis has become more commonplace globally. With a recurrence incidence of 50% within 5–10 years and 75% within 20 years, urolithiasis is frequently a chronic and recurrent illness [5]. According to certain research, a rise in kidney stone incidence is anticipated as a result of several environmental factors, such as dietary and lifestyle modifications and global warming [1,4,6]. However, the exact causes of the increased incidence and recurrence of urolithiasis are yet unknown. Kidney stone disease has a significant impact on the person and society due to its high frequency in working-age adults. It has become a public health concern, especially for populations living in hot, dry climates [7,8]. According to the mineralogical composition, kidney stones can be classified into five primary types: calcium oxalate [CaOx; 65.9%], carbapatite [15.6%], urate [12.4%], struvite [magnesium ammonium phosphate], 2.7%, and brushite [1.7%] [9,10]. Kidney stones can be roughly classified as either non-calcareous or calcareous [containing calcium]. Calcium phosphate [CaP] and calcium oxide [CaOx], either separately or in combination, are the most prevalent forms of kidney stones in humans. These stones are radioopaque and calcareous [9,11]. Randall's plaques [RPs], a foundation of caP that starts at the basement membranes of thin branches of the loop of Henle on the renal papillary surface, are where kidney stones originate [12]. While females are more likely than males to have carbapatite and struvite stones, males are more likely to have CaOx and urate stones [10,13]. However, it is still unclear how sex differences can also may have contribution in the pathophysiological mechanisms of urinary stone disease. Urinary supersaturation, crystal nucleation, development, and aggregation are all steps in the intricate and multistep process of kidney stone formation, regardless of the type [11,14]. Systemic conditions such as diabetes [15], obesity, cardiovascular disease, hypertension, and metabolic syndrome [16,17] are linked to kidney stone formation. On the other hand, individuals with nephrolithiasis, sometimes referred to as kidney stone formers [KSF], are more likely to develop hypertension [18], chronic kidney disease [CKD] [19], and end-stage renal disease [ESRD] [20,21]. Kidney stone formation is significantly influenced by a number of promoting and inhibitory variables. For instance, inter-α-inhibitor [IαI], a member of the protease inhibitor family, has been demonstrated to prevent CaOx crystallisation in vitro [24]; hyperoxaluria, hyperuricosuria, and phosphaturia are common promoting factors connected to kidney stone formation [22, 23]. Kidney stone creation and growth mechanisms remain unclear despite the accumulation of information on human stone formation. In order to help urologists, nephrologists, and primary care physicians better understand kidney stones, the current study offers an update on the mechanics of kidney stone development.
The primary cause of intrarenal crystal precipitation is urinary supersaturation and crystallisation, which is mostly brought on by inherited or acquired disorders linked to impaired renal function. Urine pH and certain concentrations of substance excess, such as CaOx, caP, uric acids and urates, struvite, amino acids [cysteine], purines [2,8-dihydroxyadenine and xanthine], and medications [such as atazanavir, sulfamethoxazole, amoxicillin, and ceftriaxone], also affect urinary supersaturation and crystallisation [25,26]. Additionally, a variety of modulator molecules—known as receptors, promoters, and inhibitors—have an impact on crystal formation and development. Numerous receptors or characteristics that resemble receptors essential for crystal-cell contact, which is acknowledged as the crucial mechanism for renal crystal retention [8,27]. 1,141 differentially expressed proteins [dEPs] were found in cOM-treated HK-2 cells after the authors recently searched for protein changes in a CaOx monohydrate [cOM] crystal-cell interaction model [28]. Heat shock protein 90 [HSP90] [29], CD44, nucleolin, hyaluronan [HA], Annexin II [30], and osteopontin [OPN] [28, 31] are examples of proteins and glycosaminoglycans that have been shown to function as modulators of stone formation [32]. Several molecules and structures also function as receptors in crystal attachments, such as the phosphatidylserine component of the lipid bilayer and the proteins' acidic side chains [33]. The primary crystal formation promoters are calcium, oxalate, urate, and phosphate ions, which can encourage the crystallisation of stone ingredients or their aggregation by activating their pathways. The first- time nephrolithiasis patients had higher blood calcium and 1,25[OH]2d levels than the matching healthy individual serum calcium levels, as shown by Ketha et al. [34]. This suggests that stone production is a sign of altered calcium and vitamin D regulation. Increased blood calcium levels stimulate lithogenesis, which is directly controlled by the calcium-sensing receptor [caSR] via many mechanisms [35]. Urate and phosphate ions have also been shown to facilitate heterogeneous nucleation and improve crystal adhesion to epitheliums [36, 37]. Urine pH is another significant factor that promotes the development of stones [38]. CaOx crystallisation and crystal precipitation can result from low pH urine [39]. Additionally, high-alkaline urine may encourage CaOx crystal nucleation and precipitation [40,41]. Two recently discovered proteins, lysozyme and lactoferrin, accelerate the pace of layer advancement on crystal surfaces, hence promoting COM development [42]. inhibitors of the development of stones. Numerous inhibitors found in normal urine work in both cooperative and competitive ways, which reduces crystallisation and prevents crystals from adhering to tubular epithelial cells or aggregating [43, 44]. Anions, metallic cations, and macromolecules are the three categories into which these inhibitors fall. At concentrations higher than 0.1 mM, anions like citrate can effectively prevent crystal formation [45,46]. Citrate excretion was reduced in most nephrolithiasis patients. In order to restore citrate excretion, patients with hypocitraturic recurrent nephrolithiasis frequently use alkali supplements [47, 48]. A structural analogue of citrate, hydroxycitrate, has been shown to have a comparable ability to form compounds with calcium to prevent crystallisation [49,50]. In acidic settings, citrate works in concert with metallic cations like magnesium to prevent crystal formation and aggregation [51–53]. The most potent crystal formation inhibitors are macromolecules. More precisely, crystal development, aggregation, and/or adherence to tubular cells can be inhibited by OPN, Tamm-Horsfall protein [THP], urine prothrombin fragment 1 [UPTF-1], nephrocalcin [Nc], and certain components of serum IαI [11,38,45]. The pattern of crystalluria in nephrolithiasis patients and healthy persons is ultimately determined by the struggle between supersaturation and inhibitors of crystallisation, as previously indicated [54]. Crystal formation and kidney stone incidence have been noted as a result of the increased promoters and decreased inhibitors.
RPs are areas of subepithelial mineralised tissue near the papillary tip, which Alexander Randall initially postulated in 1937 [55]. around the Bellini duct holes that hold caP [56]. RP are composed of a mixture of tubules with calcified walls and tubules blocked by CaP plugs, according to scanning electron microscopy [SEM] analysis [57]. CaP crystals are combined with an organic matrix rich in different proteins and lipids, which includes collagen fibres, membrane-bound vesicles or exosomes, and other extracellular matrix elements [58]. Renal stones may be caused by RPs, according to a growing number of studies [57–60]. According to Winfree et al. [61], kidney stones form as an overgrowth on RP, which has a distinct organic content [fibrillar collagen] that can be distinguished from the stone overgrowth using certain autofluorescence signatures. Notably, a prior study that used a murine model of RP found that calcium consumption and vitamin D supplementation might significantly speed up RP development [60]. Nevertheless, it is still unknown exactly how RP is formed. According to recent research, the long non-coding RNAs [lncRNAs] MALAT1 and H19 regulated the osteogenic differentiation of human renal interstitial fibroblasts [hRIFs] and took part in the creation of RP [62–64]. It has been demonstrated that lcnRNA H19 is markedly increased in RP, which can stimulate Wnt/β-catenin signalling to encourage the osteogenic differentiation of hRIFs [63]. Through its association with miR-216b, lcnRNA H19 can also facilitate the process of oxidative stress and renal tubular epithelial cell damage caused by CaOx nephrocalcinosis. It does this through the MGB1/TLR4/NF-κB signalling pathway [64]. In order to boost the osteogenic phenotype of hRIFs, lcnRNA MALAT1 can act as a competitive endogenous RNA [ceRNA] that sponges miR-320a-5p and increases Runx2 expression [62]. While further research is desperately needed to examine the processes of RP production as well as additional functions of RP in the setting of stone development, these investigations offer fresh insight into the pathophysiology of RP-mediated kidney stone disease.
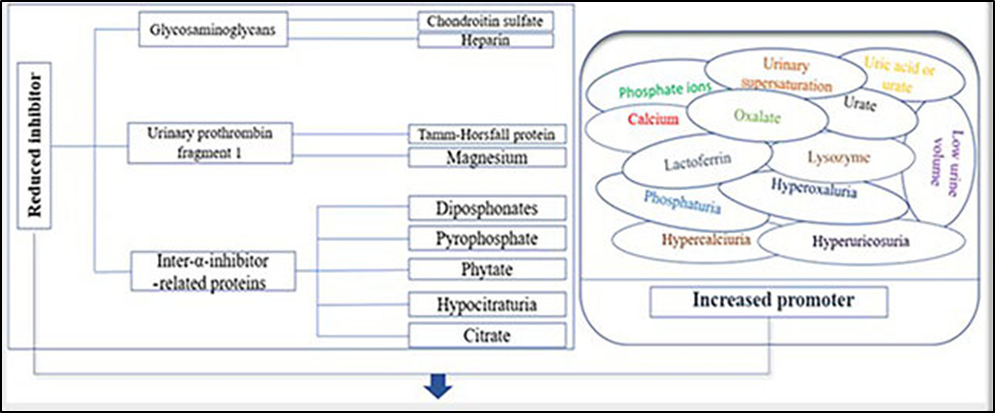
Figure 1. Kidney stone formation's physicochemical processes. Kidney stone formation may be significantly influenced by the increased promoters [right panel] and decreased inhibitors [left panel].
Males are more likely than females to develop CaOx nephrolithiasis at a ratio of 2–3:1, according to statistical investigations [4,65]; however, the precise process is yet unknown.
According to earlier research, oestrogens reduce kidney CaOx crystal deposition, plasma oxalate concentration, and urine oxalate excretion, whereas androgens raise these levels.
Additionally, the link between kidney stone formation and sex may be caused by increased androgen signalling [65–68]. Hepatic glycolate oxidase [69] and kidney epithelial nicotinamide adenine dinucleotide phosphate oxidase [NAPdH], subunit p22-PHOX, can both be directly upregulated by androgen receptor [AR] signalling at the transcriptional level. This increases oxalate biosynthesis, which in turn causes kidney stones [70]. According to Peng et al. [71], testosterone causes renal tubular epithelial cells to undergo apoptosis and necrosis via the HIF-1α/BNIP3 pathway, which leads to the development of nephrolithiasis. According to Changtong et al. [72], testosterone may exacerbate kidney stone disease by increasing surface α-enolase-induced cOM crystal-cell adhesion. Zhu et al. [73] showed that AR can prevent macrophage recruitment and reduce macrophages' capacity to phagocytose cOM crystals by reducing colony-stimulating factor 1 [cSF-1] signals through the overexpression of miR-185-5p. These results imply that the development of nephrolithiasis may be significantly influenced by androgen receptor signalling [Fig. 1]. In theory, AR may be a fresh target that might be tested for innovative treatments to prevent the development of kidney stones. Finasteride, a 5α-reductase inhibitor, has been shown to eliminate testosterone's ability to promote cOM crystallisation [74]. Dimethyl curcumin [ASc-J9], another recently found AR degradation enhancer, has been shown to inhibit oxalate crystal formation by modifying oxalate biosynthesis and kidney tubular epithelial cell damage caused by reactive oxygen species [ROS] in a rat model [73]. On the other hand, oestrogen might act as a defence against the development of kidney stones. An in vitro study showed that oestrogen caused alterations in the cellular proteome of Madin Darby canine kidney [MDCK] renal tubular cells, which resulted in decreased intracellular ATP, increased cell proliferation, and renal tubular cell tissue healing [75]. Evidence suggests that the oestrogen receptor β [ERβ] can prevent oxalate-induced oxidative stress by directly binding to the oestrogen response elements [EREs] on the NOX2 5' promoter [76], thereby suppressing the transcription of the NADPH oxidase subunit 2 [NOX2] and protecting renal CaOx crystal deposition. These results may help explain why nephrolithiasis is more common in men than in women. One possible treatment for kidney stone disease caused by calcium oxalate crystals is to target AR. However, only cells were used in these in vitro and in vivo investigations. drawings or models of animals. Clinical research and more validation are needed. Many AR-mediated illnesses, such as prostate cancer [77,78], liver cancer, and spinal and bulbar muscular atrophy neurone disease [79], are suppressed by finasteride and ASc-J9. However, given the adverse effects, including sexual dysfunction, more research is required before the practical use of finasteride and ASC-J9 in kidney stone prevention [80].
5. The Microbiome's Part in The Production of Stones
Due to their metabolic output and other contributions, bacteria that are part of the human microbiome, particularly those of the kidney and urinary tract, are anticipated to have a significant impact on urological health, both positively and negatively [81]. microorganisms that produce urease. Struvite stone development and recurrence are consistently linked to urease-producing bacteria, including Proteus mirabilis, Klebsiella pneumonia, Staphylococcus aureus, Pseudomonas aeruginosa, Providentia stuartii, Serratia, and Morganella morganii [82,83]. Urine alkalinisation and phosphate salt creation result from the bacterial urease's breakdown of urea and promotion of the production of carbon dioxide and ammonia. Although urease inhibitors and urinary acidification have been suggested and used to prevent and/or dissolve struvite stones and encrustations in patients infected with urea-degrading bacteria, their long-term use is restricted because of their toxicity and inefficiency [84]. Non-urease-producing bacteria, such as Escherichia coli and Enterococcus species, have also been linked to secondary infections in stones [85,86]. It is still mostly unknown, nevertheless, whether kidney stones originate from a nidus of infection that spreads stone formation or if they develop and become secondarily infected. Nanobacteria [NB] For more than 30 years, NB has been isolated from kidney stones [87–89]; nevertheless, the nature and underlying processes are still unknown. According to Ansari et al. [90], cultivated NB may infect individuals with apatite kidney stones and range in size from 60 to 160 nm. NB may adapt to growing in plain dMEM or RPMI-1640 by self-proliferation, according to Kajander et al. [91]. It was shown that NB was present in 70 out of 72 kidney stones [97.2%] in the study by Ciftçioglu et al. [92]. Although kidney stones made of apatite had the greatest immunopositivity, NB was present regardless of the kind of stone [91]. because they may create enough calcium apatite in their cell walls to start pathologic calcifications and stone formation, NB are thought to perform roles in calcium nucleation [93–95]. The idea that NB are living things is substantially supported by this data.
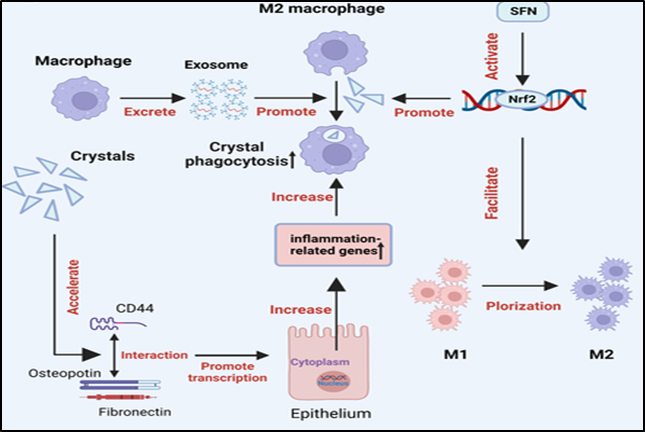
Figure 2: Immune reaction to urine crystals. The primary immune response change linked to kidney stone formation is macrophage accumulation and macrophage-related inflammation or anti-inflammation. While M2 macrophages may use crystal phagocytosis to stop CaOx inflammatory damage, M1 macrophages play a significant role in the development of CaOx stones. CaOx stands for calcium oxalate.
NB, also known as "calcifying nanoparticles [cNPs]," "nanobacteria-like particles," or "Nanobes," are simply mineral protein nanoparticles having biomimetic activities, according to an increasing number of studies [88,89]. The nature and definition of these nanoparticles are still up for debate [96], though their functions in kidney stone disorders have been extensively documented. Renal tubular epithelial cell damage associated with kidney stone formation has been related to cNPs, which have been found in RPs and shown to be cytotoxic to 3T6 fibroblasts and HK-2 cells in vitro [89]. Catalase [cAT] and malonaldehyde [MdA] levels were much greater in cNP-treated HK-2 cells than in the HK-2 control group, according to Hong et al. [97], indicating that cNPs cause lipid peroxidation and harm HK-2 cells. Wu and associates [89] showed that the cNPs may: cause ROS production by activating JNK; lower mitochondrial membrane potential and encourage cell apoptosis by downregulating Bcl-2 expression and upregulating Bax expression; cause autophagy by upregulating microtubule-associated proteins 1A/1B light chain 3B [Lc3-II] and Beclin-1 expression [Fig. 2]. Current research in the literature indicates that NB are separated from RPs and most renal stones, localised in high quantities in the kidneys, eliminated in urine, and act as the initiator by promoting nucleation and crystal formation. To resolve the debate over whether NB are alive or non-living, as well as the methods by which NB cause calcification and stone formation, more research is needed. Microbiome of the intestines. The microbiota in the intestines, which has recently attracted a lot of attention, and it has been said to participate in the development and avoidance of kidney [87,98–100] stone illness. The most common is Oxalobacter formigenes. Gram-negative anaerobic bacteria that have been well investigated and degrade oxalate in the digestive system, and may be a probiotic. Characteristics for preventing the development of kidney stones. Stern et al. [101] conducted a pilot study to examine the unique variations in nephrolithiasis patients' gut microbiomes, in contrast to individuals who do not develop kidney stones. Their findings showed that the Bacteroides genus was 3-4 times more prevalent in the kidney stone category, whereas the Prevotella genus was 2-8 times more prevalent in the non-stone control group. Urine examination over 24 hours showed that the species Oxalate levels were inversely correlated with Eubacterium. And there was a tendency towards an adverse connection with the genus Escherichia with the amount of citrate [101]. However, the possible causal role of pre-existing gut microbiome dysbiosis in kidney stones and the relationship between urinary oxalate and illness is yet unknown. Oxalate-degrading bacteria and excretion are still restricted [87,98,102,103]. Neurohormones that control the net oxalate level have been shown to influence both the absorptive and secretory routes for oxalate in the proximal and distal sections of the colon. Therefore, it has been proposed that the digestive tract plays a major role in oxalate balance and the ensuing oxalate homeostasis [104–106]. Oxalate -degrading bacteria, especially Oxalobacter formigenes, which need a strict anaerobic environment to live, are also often found in the digestive system. One theory regarding the microbiome's role in kidney stone prevention is that certain functional bacteria, like the oxalate-degrading bacteria in the human gut and intestinal tract [such as Oxalobacter formigenes, Bifidobacterium sp., Porphyromonas gingivalis, and Bacillus sp.], which flourish in the presence of the oxalate anion and use oxalate as their carbon energy source, show growth inhibition in the kidney's CaOx crystallisation [102,107,108]. The activity of oxalate-degrading bacteria has a major effect on the homeostatic levels of oxalate in plasma and urine and facilitates the extra-renal clearance of oxalate in the intestines [109]. There is a clear correlation between this activity and the development of CaOx stones.
The primary immune response change seen in kidney stone illness is macrophage accumulation and macrophage-related inflammation or anti-inflammation, which has been well documented to be essential for renal CaOx crystal formation [110]. First, via interacting with OPN and fibronectin [FN] [111], which are increased in renal tubular cells produced by crystals, the recruited macrophages may encourage the formation of cOM crystals. Second, it has been demonstrated that macrophages release a variety of mediators through traditional secretory channels that result in renal interstitial inflammation [112,113]. especially interleukin-8 [IL-8], monocyte chemoattractant protein-1, and macrophage inhibitory protein-1 [112]. As a result, these chemokines improve the recruitment of different immune cells into the inflammatory site, such as monocytes, macrophages, neutrophils, dendritic cells, and T-cells [114,115]. Numerous investigations have shown that kidney stone development is influenced by exosomes generated from macrophages after cOM exposure [112,113,116]. A group of proteins found in cOM-treated macrophage exosomes were previously found to be primarily engaged in immunological functions, such as cell migration, Fcγ receptor-mediated phagocytosis, T-cell activation and homeostasis, and interferon-γ [IFN-γ] control [112]. Furthermore, infiltrating monocytes may exhibit protective or harmful actions in the formation of kidney stones [110] and differentiate into many macrophage subtypes with a broad variety of clinical symptoms, presentations, and histological phenotypes [110,117]. There is growing evidence that renal CaOx crystal formation is significantly influenced by M1/M2-macrophage differentiation [111,115,118–120]. It is still debatable, nevertheless, if M1 macrophage-mediated inflammation that aids in the development of stones will start stone promoters and decrease stone inhibitors. M1 macrophages were shown by Khan et al. [58] to be capable of causing acute tissue damage, which was linked to RP production and crystal deposition. On the other hand, Taguchi et al. [121] found no changes in urine variables in lipopolysaccharide [LPS]-induced M1 macrophage-mediated acute renal damage, leading them to infer that there was no correlation between increased crystal deposition and renal dysfunction. Through a clathrin-dependent process, M2 anti-inflammatory macrophages may phagocytise and break down CaOx kidney stone pieces [110,113,115,120,121] The immunotherapy approach has been suggested to prevent stone recurrences in certain individuals by modulating the immune response in order to degrade CaOx crystals and thereby prevent stones from developing, given the crucial role of the immune response in CaOx crystal formation and development [122]. However, there is an urgent need to look into immunotherapeutic targets for kidney stone disease. [123-134]
CONCLUSION AND OUTLOOK FOR THE FUTURE
The current review article summarised new insights into kidney stone disease-related metabolic risk factors, receptors, promoters, and inhibitors by examining the roles of immune response, microbiome, and sex hormones in stone formation and development. Crystallisation mechanisms are insufficient to fully explain the pathophysiology of kidney stone disease. However, several kidney stone production study topics are still poorly known and were not included here owing to current research constraints. In order to create new preventative and therapeutic strategies, more thorough research is required to clarify the processes of the microbiome and immune response in kidney stone development.
Conflicts of interest:
There are no conflicts of interest or disclosures regarding the manuscript.
Acknowledgment:
The authors sincerely thank Samarth College of Pharmacy, Belhe, University Libraries, and all other sources for their cooperation and advice in writing this review.
REFERENCES





Pratik Bhand, Ajay Bhagwat, Sakshi Shinde*, Dnyaneshwari Nimbalkar, Aditya Patil, Swapnil Auti, A Review: Of Recent Breakthroughs in Kidney Stone Production Mechanisms, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1043-1058. https://doi.org/10.5281/zenodo.17836935
 10.5281/zenodo.17836935
10.5281/zenodo.17836935
