1,2,3,4,5,6,7,8,9 Department of Pharmacy, Seacom Pharmacy College, Dhulagori, Howrah, Jala Dhulagori, West Bengal, India 711313
10 Department of Pharmaceutical Quality Assurance, Guru Nanak Institute of Pharmaceutical Science and Technology, Nilgunj Rd, Sahid Colony, Panihati, Khardaha, West Bengal, India 700114
Naegleria fowleri is a free-living, heat loving amoeba mostly originate in freshwater environment like lakes, hot springs and poorly maintained swimming pools. Although it usually survives harmlessly in nature, it can become highly dangerous when it accidently enters the human body through the nose. This organism is responsible for a rare but fatal brain infection known as Primary Amoebic Meningoencephalitis (PAM). Infection typically occurs during swimming or diving activities when contaminated water is forced into nasal cavity. The amoeba moves through the olfactory nerves to the brain, where it rapidly multiplies and causes critical inflammation, tissue destruction and neurological damage. This review provides an overview of the biology, life cycle, transmission and pathogenesis of naegleria fowleri. It also discusses the major virulence factors such as tissue damaging enzymes and host immune responses that contributes the rapid progression of PAM. In addition, current diagnostic approaches including microscopy, culture techniques, PCR based methods and advance molecular techniques. Treatments options such as amphotericin B, miltefosine and other therapies are reviewed, along with current research in nanomedicine and future preventive strategies. Due to high mortality rate and challenges in early diagnosis, increased awareness, improved surveillance and development of effective therapies are essential to reduce the impact of this deadly pathogen.
Free- living amoebae are small living beings set up in soil and water that can thrive without demanding a host. Primarily, free-living amoeba attend with humans without causing any detriment. In fact, a many species of free-living amoeba retains the eventuality to induce serious sickness when they accidentally find their way inside the mortal body. Naegleria fowleri, a type of free- living amoeba, was set up to be one of the most dangerous amoebae due to its energy to resettle to the mortal central nervous system to induce primary amoebic meningoencephalitis (PAM). Despite its oddity, its rapid-fire development and massive death rate brought N. fowleri under growing scientific concern.
Naegleria fowleri is known to be a heat-loving protozoan and grows well in warm brackish surroundings similar as lakes, gutters, hot springs, and also in inadequately chlorinated swimming pools. These environmental conditions are largely conducive for recreation, hence adding the chances of mortal contact. nonetheless, infection with the protozoan appears to be rare, which could be related to the interplay of colourful environmental and host factors for the development of PAM.(1) The largest number of PAM infections has been reported under conditions of high temperatures. The complaint that has come to be known as primary amoebic meningoencephalitis was linked in themid-1960s as a result of unexplained and fatal outbreaks of meningitis in Australia. posterior exploration has shown that the causative agent in this complaint is the organism Naegleria fowleri, and there has now been a periodic appearance of this complaint in other corridor of the world, including North America, Asia, and Australia. While the complaint has been rare, the fact that it has appeared regularly has maintained the significance of this organism in the professional literature. Infection in humans takes place when polluted water containing the N. fowleri sponger enters the nasal passages, generally during diving and swimming conditioning. still, the sponger, on ingestion, doesn’t beget detriment since it dies due to the acidity of the stomach contents. The sponger takes a fascinating route of entry into the mortal tissues by clinging to the mucous membranes of the nose and progressing through the olfactory jitters. Through this route, the sponger avoids all the vulnerable defences in the tissues and infects the brain.(2) After infecting the central nervous system, the sponger proliferates fleetly, causing immense damage to the brain tissues by destroying the tissues and converting violent inflammation in the tissues.
The clinical symptoms presented by cases suffering from PAM can be relatively deceptive, especially during the early stages. For illustration, symptoms like headache, fever, puking, and stiffness of the neck act those presented in meningitis cases. still, as the condition progresses to full-bloated neurological damage due to impairment of the central nervous system, cases suffer from confusion, seizures, and ultimately death. The oddity of this condition coupled with the parallels in symptoms displayed when cases suffer from central nervous system infections mean that this condition is always diagnosed late in utmost cases. From a natural perspective, Naegleria fowleri has shown a vast capacity for conforming itself in different circumstances. Naegleria fowleri has three different life forms trophozoite, flagellate, and cysts.(3) While the trophozoite form can beget an infection, the main niche for the organism is the neural tissues. Recent exploration has shown the significance of the commerce between the vulnerable system of the host and the pathogen, Naegleria fowleri, in understanding the part played by the seditious responses and the dislocation of the blood- brain hedge.
In the recent history, there have been rising enterprises about the implicit goods of climate change on the epidemiology of Naegleria fowleri. With the rising global warming and the growing application of natural freshwater coffers, there could be favourable environmental determinants for the organism. Cases of infection have been recorded in areas preliminarily regarded as non-endemic; hence the significance of continued surveillance and exploration. This review aims at collecting being information regarding the environmental ecology, natural parcels, and pathophysiology of Naegleria fowleri.
OBJECTIVES
This paper focuses on various aspects of the organism, including its biology, mode of adaptation, pathogenesis and the cellular mechanism involved in disease progression.
BIOLOGY AND LIFE CYCLE OF NAEGLERIA FOWLERI
Naegleria fowleri is a free-living, thermophilic amoeba flagellate belonging to the phylum percolozoa and family Vahlkampfiid. It is widely distributed in warm freshwater environments such as lakes, rivers, hot springs, poorly maintained swimming pools and soil. It normally exists as a free- living organism, N. fowleri becomes an opportunistic human pathogen when it enters the nasal cavity, leading to Primary Amoebic Meningoencephalitis (PAM).
Life cycle and Morphological stages:
It exhibits three different morphological stages during its life cycle:
Trophozoites stage (infective stage): The Trophozoites is the active, feeding, reproducing, and infective stage of Naegleria Fowleri. This stage predominant in both the environment and the human host. They are typically 10-25μm in size, although larger forms may be observed. They exhibit an amoeboid shape with a single nucleus containing a large, centrally located karyosome and no peripheral chromatin.(4) Movement occurs through eruptive pseudopodia, giving the trophozoites a characteristic directional motility. They multiply by binary fission, a process that occurs rapidly under favourable conditions, particularly at temperatures between 35-46?. This thermophilic nature explains the increased risk of infection during summer months and in warm water bodies. In the environment, trophozoites feed on bacteria, algae and organic debris. In the human host, they become highly pathogenic, feeding on neutral tissue, red blood cells and leukocytes. Tissue destruction occurs through direct phagocytosis and the release of cytolytic enzymes such as proteases and phospholipases. Only the trophozoite stage is found in infected human tissues.(5) Rapid multiplication and aggressive tissue invasion by trophozoites lead to severe inflammation, haemorrhage, and necrosis of brain tissue, resulting in the acute and fatal course of PAM.
Flagellate stage (transitional form): The flagellate form is pear-shaped 10-16μm. It possesses two anterior flagella, which allow rapid motility in aquatic environments. The nucleus retains the same basic structure as in the trophozoite stage. Transformation from trophozoite to flagellate form occurs when the amoeba is exposed to low nutrient availability or changes in ionic concentration, such as placement in distilled water. This transformation can occur within a few hours and is reversible. Although the flagellate stage does not feed or replicate, it enhances the organism’s ability to disperse and locate more favourable environments.(6) Once suitable conditions are restored, the flagellate rapidly converts back into the trophozoite stage. They maty enter the nasal cavity, but they do not survive in human tissues and quickly transform back into trophozoites, which then initiate infection.
Cyst stage (resistant form): Cysts are round, double-walled structures measuring approximately 7-15μm in diameter. The cyst wall provides protection against adverse environmental conditions such as low temperatures, desiccation and lack of nutrients. Encystment occurs when environmental conditions become unfavourable, particularly during nutrient depletion or temperature reduction. Cysts can persist in sediments and water for extended periods until conditions again favour excystation.(7) When environmental conditions improve, cysts excyst to release trophozoites, there by continuing the life cycle.
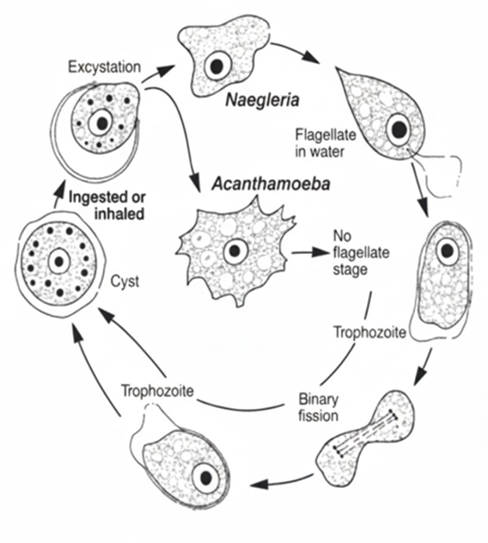
FIG 1- LIFE CYCLE OF NAEGLERIA FOWLERI
HISTORY OF NAEGLERIA FOWLERI:
Naegleria fowleri is a free living, thermophilic amoeba that has gained considered scientific and medical attention due to its ability to cause Primary Amoebic meningoencephalitis (PAM), a rare but almost invariably fatal infection of the central nervous system. Although free living amoeba were recognized long before, their pathogenic potential in humans was not fully understood until the mid-20th century.
The first human cases of PAM were reported in 1965 by Fowler and Carter in Australia. These cases involved previously healthy children’s and young adults who developed acute meningoencephalitis following exposure to warm freshwater during swimming. The rapid progression and fatal outcome of the disease distinguished it from other forms of meningitis into its etiological agent. Subsequent studies revealed that Naegleria fowleri is commonly found in warm freshwater environments, including lakes, ponds, hot springs and poorly chlorinated swimming pools.(8) Its preference for elevated temperatures explained the seasonal occurrence of most cases, particularly during summer time as well as its higher prevalence in tropical and sub-tropical regions. Notably reported cases have emerged in the United Staes, Australia, India, Thailand, Egypt, Brazil, South Africa, Pakistan have also reported cases. This global distribution highlights that N. fowleri is not confined to any single region but is instead present in various warm climates around the globe. Since the initial recognition, N. fowleri infections have been documented in various parts of the world. Although the number of cases remains low, typically numbering just few annually worldwide, the fatality rate is high, often exceeding 95%.(9)
In recent decades, increased awareness, improved diagnostic capabilities and enhanced epidemiological surveillance have contributed significantly to the understanding of naegleria fowleri and PAM. Despite the rarity of infection, the organism remains a serious public health concern due to its extremely high fatality rate and its association with common recreational and domestic water exposure.
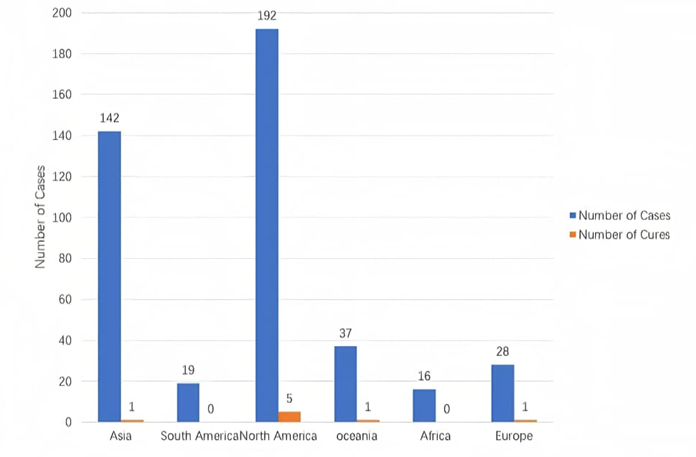
Fig 2 - The number of N. fowleri cases and cure status by continent from 1937 to 2024.
PATHOPHYSIOLOGY OF NAEGLERIA FOWLERI
Nasal Colonization and Olfactory Mucosa Penetration
The journey of Naegleria fowleri from the outside world into the central nervous system (CNS) begins almost exclusively when its active trophozoite form is carried into the nasal cavity by water during activities like swimming, diving, or nasal rinsing with untreated water. The moist mucosa of the upper nasal passages provides the first contact point between human tissue and the amoeba. Once trapped in the nasal mucus, the amoebae use adhesion proteins on their surface to anchor themselves firmly to the olfactory epithelium the specialized tissue high in the nasal cavity that houses olfactory sensory neurons. This anchoring is not passive; molecules such as Nfa1 and other adhesins help the trophozoites cling to the mucosal surface and begin to resist being flushed back out with mucus or water flow.(10) To breach this first barrier, N. fowleri secretes enzymes like proteases, phospholipases, and neuraminidases that weaken the structural integrity of the mucosa and disrupt tight junctions between epithelial cells. These enzymes act like microscopic scalpels and chisels breaking down proteins and lipids that normally protect the nasal lining allowing the amoeba to slip between and through the cells of the olfactory mucosa.(11)
Naegleria fowleri is a free-living amoeba that normally survives in warm freshwater environments such as lakes, rivers, hot springs, and poorly maintained swimming pools. Humans are not its natural host, and infection happens accidentally when water containing the amoeba enters the nose. This usually occurs during swimming or diving, especially when water is forced upward into the nasal cavity. Drinking contaminated water does not cause infection because the organism is destroyed by stomach acid. After entering the nasal cavity, Naegleria fowleri comes into contact with the nasal mucosa, mainly the olfactory epithelium located in the upper part of the nose. This area is important because it contains nerve endings responsible for the sense of smell and provides a direct connection to the brain. The amoeba attaches to the epithelial cells and begins to damage them by releasing enzymes such as proteases and phospholipases. These enzymes break down cell membranes and allow the organism to penetrate deeper tissues. Once the nasal epithelial barrier is breached, the amoeba migrates along the olfactory nerve fibers.(12) It passes through the cribriform plate, a thin bone that separates the nasal cavity from the cranial cavity. This pathway allows N. fowleri to reach the brain without entering the bloodstream, which means it avoids the protection normally provided by the blood–brain barrier. Inside the brain, Naegleria fowleri exists mainly in its trophozoite form, which is the active and feeding stage of the organism. The trophozoites multiply rapidly and spread through brain tissue, especially affecting the olfactory bulbs and frontal lobes first. The amoeba causes direct damage to neurons by phagocytosing neural cells and releasing toxic substances that lead to cell lysis and tissue necrosis. Small areas of hemorrhage may also occur due to destruction of blood vessels.
At the same time, the host’s immune system mounts a strong inflammatory response. Immune cells such as neutrophils and macrophages are recruited to the site of infection, and inflammatory mediators are released. However, this response is not effective in eliminating the amoeba and instead worsens brain damage.(13) The inflammation leads to cerebral edema, increased intracranial pressure, and reduced blood flow to brain tissue, which further contributes to neuronal injury. As the infection progresses, the widespread inflammation of the brain and meninges results in primary amoebic meningoencephalitis (PAM). The rapid destruction of brain tissue explains the sudden onset and fast progression of symptoms, including severe headache, high fever, nausea, vomiting, confusion, and seizures.(14) If the disease is not controlled quickly, increased intracranial pressure can cause brain herniation, leading to coma and death.
Overall, the pathophysiology of Naegleria fowleri infection is marked by rapid nasal entry, direct migration to the brain through the olfactory nerve, aggressive tissue destruction by the amoeba, and a damaging inflammatory response by the host. These combined factors explain why PAM is rare but almost always fatal and why early diagnosis and treatment are extremely difficult.
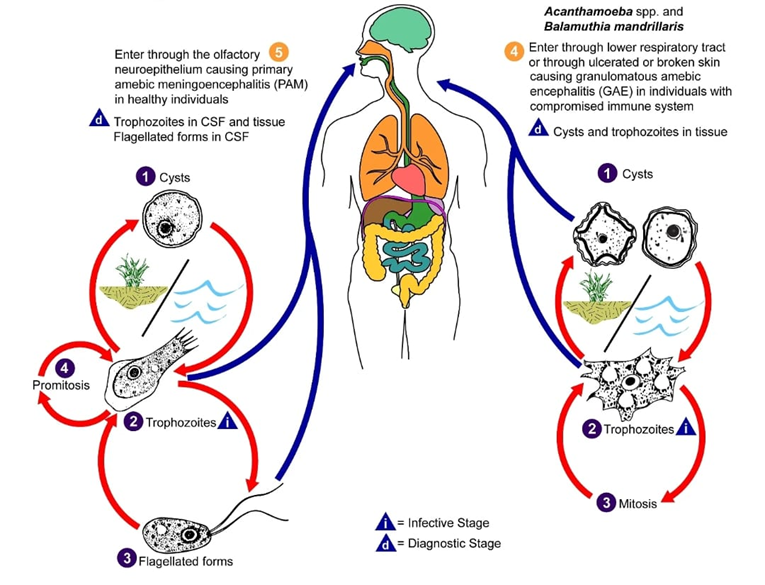
FIG 3- PATHOPHYSIOLOGY OF NAEGLERIA FOWLERI
Pathogenesis of Naegleria fowleri Infection
Naegleria fowleri is a free-living, thermophilic amoeba commonly found in warm freshwater environments. Human infection occurs accidentally and almost exclusively through the nasal route. The organism does not infect through ingestion; instead, disease begins when contaminated water enters the nasal cavity during activities such as swimming or diving.
Once inside the nasal passages, N. fowleri adheres to the olfactory epithelium. Using surface adhesion molecules and active motility, the amoeba penetrates the nasal mucosa and migrates along the olfactory nerve fibres. This direct neural pathway allows the organism to bypass the blood–brain barrier, reaching the olfactory bulbs and frontal lobes of the brain. Within the central nervous system, N. fowleri exists in its trophozoite form, which is responsible for tissue invasion and destruction.(15) The amoeba causes damage through a combination of mechanical disruption and cytotoxic activity. It releases proteases, phospholipases, and pore-forming proteins that degrade host cell membranes, leading to neuronal cell death. Additionally, the amoeba actively phagocytoses neural tissue, erythrocytes, and leukocytes, further contributing to tissue necrosis.
The host immune response, although rapid, is largely ineffective. Neutrophils and macrophages are recruited to the site of infection, resulting in intense inflammation. However, the amoeba’s resistance to complement-mediated lysis and its ability to induce host cell apoptosis allow it to survive. The inflammatory response itself exacerbates cerebral edema, increasing intracranial pressure. The combined effects of direct amoebic cytotoxicity and host-mediated inflammation led to acute haemorrhagic necrosis of brain tissue, a condition known as primary amoebic meningoencephalitis (PAM). The disease progresses rapidly and is typically fatal within days if not treated aggressively.

FIG4-PATHOGENESIS OF NAEGLERIA FOWLERI INFECTION
SYMPTOMS
DIAGNOSTIC APPROCH OF N. FOWLERI
The Primary Amoebic Meningoencephalitis (PAM) is rare and fatal disease, the amoeba mostly found in hot environment like, lake, hot springs & currently grow rapidly due to the undiagnostic condition. The condition is occurred due to almost mimic same symptoms with most of the viral, bacterial meningitis.(16) Due to this most of the time misdiagnosis is occurs. Although there are some processes by which we can detect the N. fowleri amoeba, that we discussing below –
CULTURE METHOD
Cerebrospinal fluid is to be tested in the diagnostic laboratory in room temperature by puncture, the fluid is cultivated at 37 ?C in the presence of antiseptic (Streptomycin & Penicillin) in non-nutrient agar medium in the presence of Escherichia coli. If we observed the CSF, it looks cloudy, turbid sometimes yellowish or pink. The amoeba utilized the nutrient of agar media indirectly through the bacteria E.coli present into the surface of the medium. We have to examine it under inverted light microscope daily by which we can observed the presence and movement of trophozoites & increasing number of WBC cell due to inflammation of and necrosis of brain cell. If we increase the temperature from 37 ?C to 42-45 ?C then we can see the motile trophozoites due to thermophilic nature.(17)
But it is time consuming & had some similarity with bacterial and viral meningitis. So, there is a chance of misdiagnosis due to this method, and most of the cases the test is performed after the death of the patient in the autopsy. There is some limitation like the CSF sample must be fresh, because stale sample may be causing decreasing amount of amoeba.
MICROSCOPIC METHOD
Most of the time we used microscopic examination of CSF due to similarity with other nervous system infection. Despite of using culture method, we used mount wet method to determine the presence of viable amoeba in the CSF. Which consist of turbid fluid, higher concentration of protein, high pressure of fluid, neutrophils, decreasing concentration of glucose. We used trichrome, Giemsa, or Wright stain to make difference between movable amoeba and white blood cell. We used wet mount method rather than gram staining, because if we used gram staining the heat fixation process may cause potential damage on the trophozoite cell. The size of trophozoites that can be observed through this method mostly between 20-30 µm. It’s highlighted the presence of prominent central karyosome containing single nucleus which ensure of N. fowleri. But the accurate result is depended on proper sample handling, and the accuracy of clinician.(16,18)
Patient suffering from PAM often notices a highly presence of leukocytes that signify a elevated cell count of white blood cell into the blood stream. That indicate ongoing infection of body cell. The analysis of CSF observed that cell count of WBC about 300-26000 cell / mm. And many time due to less amount of CSF it’s mostly doesn’t able to distinguish between the amoeba cell and leukocytes.
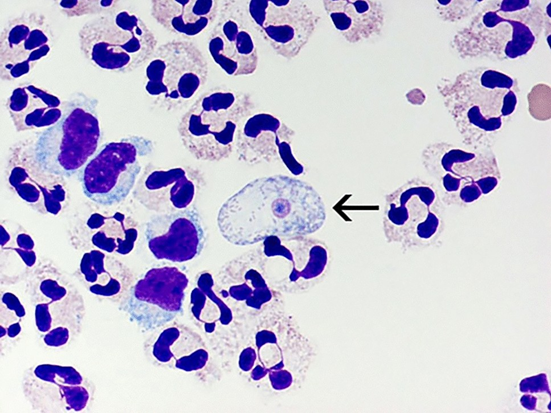
FIG 5 – MICROSCOPIC IMAGE OF N. FOWLERI
RADIOLOGICAL IMAGING
Radiological image helps to detect various abnormality of brain. CT (Computed Tomography) scan, MRI (Magnetic Resonance Imaging) is use to detect various structural abnormality (Like: cell damage, tumour, internal bleeding, stroke) in entire cranial vault such as cerebrum, brainstem, cerebellum etc. But it can’t detect presence of any microorganism like; N. fowleri directly. When the amoeba spread accurately it will detect what kind of damage does the amoeba cause brain cell.(19)
With the CT (Computed Tomography) scan it show normal report on the early stage of scanning, and into the growing stage or moderate it shows some default like diffusion in cerebral edema, hypodense in frontal and temporal lobes areas, decreasing in the Gray-white matter, into the advance stage it show excessive brain swelling and also show brain herniation. That helps us to detect infection in brain cell.
In case of MRI (Magnetic Resonance Imaging) it’s produced better analysis respected to CT scan. It’s helps us by detecting Hypointense/isointense lesions through T1-weighted imaging, hyperintense signals from frontal, temporal lobes through T2-weighted imaging, cytotoxic edema through diffusion-weighted imaging.
Although radiological imaging does not directly helps us to detect N. fowleri amoeba. But still it’s easily available less time consuming and help us to know brain morphological condition.

FIG 6 – MRI IMAGE SHOWING N. FOWLERI
RT-PCR
Real Time Polymerase Chain Reaction (RT-PCR) is one of the sensitive, specific advance laboratory test for the detection of N. fowleri. This method enable rapid diagnosis and very accurate treatment according to the rapid progress of this disease. It identify the DNA of N. fowleri amoeba by targeting non-coding spacers ITS1 & ITS2, 18S rRNA region that make distinguish between N. fowleri and any other free-living amoeba.(20,21)
For the diagnosis of N. fowleri we have to collect CSF from the lumber puncture or nasal discharge, brain tissue may be fresh or preserved under sterile condition. Then extract the DNA genome of the sample and mixed with DNA polymerase enzyme, specific primers, fluorescent dye in a thermal cycles and allow for repeated heating and cooling for the amplification of targeted DNA. If N. fowleri is present then it shows recorded signal as amplification curves and increases of fluorescent dye. And help as for the detection of N. fowleri.
ADVANCED MOLECULAR DIAGNOSIS
In this type of diagnosis we used mNGS (Metagenomic Next-Generation Sequencing), LAMP (Loop-Mediated Isothermal Amplification) assay, IFA (Immunofluorescence Assay), ELISA (Enzyme-Linked Immunosorbent Assay), Immunohistochemical Staining to detect the presence of amoebic antigen – antibody also in a low quantity DNA sample of CSF or tissue culture.
In case of mNGS method we collect the CSF from the patient used to diagnosis it without using a specific primer. Most of the time it’s performs when RT-PCR show negative result. The genetic sequence of the sample is matched with reference database and detect the presence of N. fowleri.
Into the LAMP we don’t need any thermal cycles for the identification. We collect the CSF and mixed it with specific LAMP primer, DNA polymerase, nucleotide buffer and incubate the mixer at 55-65 ?C for 50-60 mins. Then observed the change of colours, turbidity for the detection of N. fowleri amoeba. (22)
In case of IFA assay we used specific fluorescent antibody for the specific amoeba. Take the CSF smear in a clean slide, fixed with alcohol, then add specific antibody, incubate for a specific time, then wash the smear for washed the unbounded antibody. Then observed under microscope, if N. fowleri is present into the sample then the microscopic view shows a green bright trophozoite present onto the sample.
By the ELISA method we take the CSF sample, add coating of microtiter plates, incubate for needed time, wash the sample for wash out unbounded antibody, add secondary enzyme linked antibody and substrate. Observed under microscope positive result shows intense colour of the sample that indicate the present of N. fowleri trophozoite.
In immunohistochemical staining we collect the tissue sample from brain, fixed with 10% formalin for preservation, then collect the thin layer from that and placed into a clean slide. Then add enzyme-induced antigen for the activation of antigen site.(23) Then add some blocking agents for blocking of non-specific blinding site. Then add specific primary antibody for N. fowleri and incubate it. Then add secondary antibody for binding with primary antibody. Then add a substrate called DAB as colouring agent and add counter stain called haematoxylin and observed under microscope, positive result produced bright brown colour trophozoite that confirm presence of N. fowleri amoeba.
DRUGS UDED IN THE TREATMENT OF N. FOWLERI
TABLE 1: Drugs already used for clinical treatment.(24,25)
|
Types of Drugs |
Drugs |
Route of administration |
Mode of Action |
Drawbacks |
|
Antifungal |
Amphotericin B |
Intravenous or intrathecal |
Amphotericin B, a drug in the antifungal agent category, has an ergosterol-binding mechanism that leads to the leakage of monovalent ions and ultimately results in cell death. Studies have shown that amphotericin B is capable of inducing ultrastructural alterations in amoebae, which include nuclear deformation, increase in the endoplasmic reticulum, decrease in food vacuoles, decrease in pseudopodia, mitochondrial damage, increase in autophagic vacuoles, and blebbing of the plasma membrane. |
Amphotericin B has limited ability to cross the blood-brain barrier and needs high doses. Patients receiving Amp B treatment often experience acute infusion reactions and kidney problems related to the dose. These can include kidney injury, anaemia, chills, fever, vomiting, and, in some cases, brain damage. |
|
|
Fluconazole |
Intravenous or oral Duration:28 days |
Another antifungal drug with a different mechanism is fluconazole. It works by inhibiting an enzyme named azole sterol 14α-demethylase (CYP51), which prevents the removal of the C-14 methyl group. This reduces the production of ergosterol in the fungal cell membrane. Fluconazole also easily passes through the blood-brain barrier and reaches many areas of the central nervous system. |
It may cause severe side effects. Chronic use of azole medications has been associated with liver injury and hormone-related issues, including breast enlargement in males (gynecomastia), hair loss, decreased sperm count, sexual dysfunction, and low blood sodium levels (hyponatremia). |
|
|
Azithromycin |
Intravenous or oral Duration:28 days |
It inhibits mRNA from binding to ribosomes, which prevents protein synthesis. It can easily enter tissues. It has a long half-life, can easily enter the brain, is relatively not very toxic, and might be very effective with amphotericin B. |
It has not been able to effectively treat the infection and has little effect on the pathogen. |
|
Antibiotics |
Rifampin |
Intravenous or oral Duration:28 day |
Easily crosses the BBB |
It has poor anti-pathogen efficacy and cannot effectively cure infections. |
|
|
Miltefosine |
Oral Duration:28 days |
Miltefosine is an FDA-approved drug that acts against leishmaniasis. It has been shown to be effective against free-living amoebae in laboratory experiments and in living organisms, and it is also able to pass the blood-brain barrier and concentrate in the brain tissue. |
Miltefosine can cause severe stomach problems such as vomiting, nausea, stomach pain, and diarrhoea. There is also a possibility that the drug may not work anymore in the future. There could also be brain damage or disability. |
|
Corticosteroids |
Dexamethasone |
Intravenous |
Dexamethasone is routinely used to lower intracranial pressure and regulate cerebral edema, effectively reducing brain swelling. |
It mostly treats cerebral edema and has minimal impact on N. fowleri.
|
NANOMEDICINE
Silver nanoparticles (AgNPs) have great potential for the treatment of Naegleria fowleri infections as they possess strong antimicrobial and anti-amoebic properties. Naegleria fowleri is the causative agent of primary amoebic meningoencephalitis (PAM), a rapidly progressing and mostly fatal disease in which the conventional drugs fail due to their toxicity and inability to cross the blood-brain barrier. Silver nanoparticles target the amoebae primarily through the production of reactive oxygen species (ROS). ROS induce oxidative stress within the trophozoites, resulting in the damage of proteins, lipids, and DNA. AgNPs also come into contact with the cell membrane of the amoeba, increasing its permeability and disrupting its integrity, resulting in cell death. Moreover, silver nanoparticles can inhibit mitochondrial activity and disrupt critical enzymatic reactions in N. fowleri.(26) When used as a drug delivery system, silver nanoparticles (AgNPs) can enhance the effectiveness of traditional anti-amoebic drugs. They enhance the stability of the drugs, the release of the drugs, and the utilization of the drugs by the body, while minimizing toxicity. Since they are small, they can penetrate more easily, including the brain tissue where the parasite resides. The antimicrobial properties of silver nanoparticles are broad, and this can reduce the possibility of acquiring additional infections during the treatment process. Even though most of the studies on silver nanoparticles against N. fowleri are still laboratory or experimental-based, the findings suggest that AgNPs can be a useful adjunct or alternative treatment. In general, silver nanoparticles represent a new and effective approach to nanomedicine.(27) They can assist in the treatment of Naegleria fowleri infection by directly injuring the amoeba and by enhancing targeted drug delivery to the central nervous system.
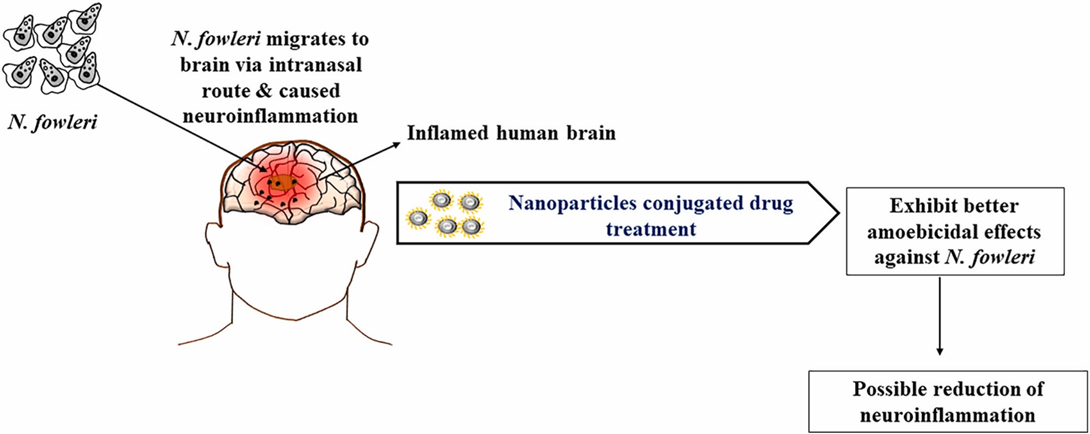
FIG 7 – Show how silver nanoparticle helps out in the treatment of N. FOWLERI
FUTURE ASPECT OF BRAINEATING AMOEBA
Advanced Diagnostic tools development
Rapid molecular diagnostics like PCR-based assays, metagenomic sequencing are being developed for early detection in water supplies and clinical samples which focused on reducing the detection time from days to hours, to improve treatment for Primary Amoebic Meningoencephalitis.
PCR-based assays target specific genetic marker unique to N.fowleri like MP2CL5,18s RNA. Typically, CSF and brain tissue are the clinical sample used in this technique. In this method, first the sample is collected then genomic DNA is extract from the sample by commercial DNA extraction kits then millions of copies are creates using specific primers of the target DNA and results are confirmed via gel electrophoresis or fluorescence.(28) This diagnostic method is gold standard for PAM detection cause results are normally available within 2-3 hours, can detect as little as one amoeba in sample. There is various types of PCR assay is present like, Real time PCR (qPCR) this is preferred for clinical method because it allows simultaneous detection and quantification for the pathogen and also uses TaqMan probes to identify specific genes like MP2CL5, Multiplex PCR, conventional PCR etc.
Artificial intelligence trained to CSF microscopy images, MRI scan, CT scan & other N. fowleri behavior can minimize human errors and speed up diagnosis.(29)
Effective Treatment development
Future research will focus on designing drugs which selectively kills amoeba without harming human brain cells.
Designing nanoparticles that can cross the blood-brain barrier and deliver a high-concentration "payload" of drugs e.g., miltefosine + an antifungal like amphotericin B, directly to the site of infection.(30)
Future research will find antigens for N.fowleri & development of vaccine for N.fowleri.
Future Prevention Strategies
Targeted campaigns in risky areas should promote using filtered or boiled water for nasal irrigation avoiding diving in warm stagnant waters. Educating low-cost protections like nose clips during diving or swimming.(31)
Use synergistic biocides like ozone or chlorine dioxide, in waste water treatment, industrial water system like oil field, to bypass amoeba resistance.
Improved water management & monitoring like controlling water temperature, specialized monitoring in warm fresh water environment, combine chlorine and UV light treatment in public water systems, regularly flush water pipes to reduce biofilm buildup.
CONCLUSION
Naegleria fowleri is a free-living, thermophilic amoeba capable for causing PAM, a rear but almost invariably fatal infection of CNS. Despite its low incidence, the organism poses a serious health treat due to its rapid progression, nonspecific early symptoms, and limited window for effective intervention. Its ability to enter the human body through the nasal cavity and migrate directly to brain via olfactory nerve allow it to bypass BBB, resulting neural death. N.fowleri show three different morphological stages, the trophozoite stage is primarily responsible for pathogenesis through active phagocytosis or nerve tissue, secretion of cytolytic enzymes and induction of a severe inflammatory response that contributes to cerebral edema and increased intracranial pressure. Current diagnostic and therapeutic approaches hindered by delayed detection and poor penetration of drug into brain tissue, leading to very high mortality rate of 95%-99%. However, the future should focus on developing on early detection tools such as PCR based assay, nanomedicine and artificial intelligence assisted detection, which offer promising prospects for early diagnosis and improved treatment outcomes. Enhanced surveillance, public awareness and contaminated research into effective therapies and preventive strategies are essential to reduce to future burden of this deadly pathogen.
REFERENCES








Souvik Kundu, Rahul Patra, Dr. Khokan Bera, Shivansh Tiwari, Krishna Chandra Bag, Ramen Karak, Koustab Pandit, Ayshwarya Purkait, Durgamadhab Das, Goureesh Ghosh, A Detailed Overview from Pathogenesis to Apoptosis of Naegleria Fowleri, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2626-2641. https://doi.org/10.5281/zenodo.18670747
 10.5281/zenodo.18670747
10.5281/zenodo.18670747
