Department of Pharmacology, RBVRR Women’s College of Pharmacy, Affiliated to Osmania University, Hyderabad-500027, Telangana, India
Skin disorders represent one of the most frequent clinical concerns globally, affecting individuals across all age groups and significantly influencing physical, psychological, and social well-being. Due to the skin’s constant interaction with external and internal stimuli, dermatological diseases arise through complex interactions involving microbial invasion, inflammatory and immune dysregulation, environmental exposure, genetic predisposition, structural abnormalities, and biochemical imbalances. This review provides a comprehensive and mechanistic understanding of major categories of skin disorders, including infectious, inflammatory, autoimmune, pigmentary, adnexal, wound-related, and neoplastic conditions. The review begins with a detailed exploration of skin structure—particularly the epidermis and dermis—to establish the functional basis upon which pathological changes occur. The etiology and pathophysiology of a wide spectrum of dermatological conditions such as bacterial, viral, fungal, and parasitic infections; eczema; psoriasis; acne vulgaris; vitiligo; melasma; atopic dermatitis; alopecia; periorificial dermatitis; ichthyosis; wound healing impairments; traditional medical conditions such as Kushtha; and skin cancers including melanoma and non-melanoma malignancies are examined extensively. Emphasis is placed on molecular, cellular, immunological, and environmental mechanisms that initiate and perpetuate each disease. By integrating clinical and mechanistic insights, this review aims to enhance the understanding of skin disease progression and support the development of targeted therapeutic strategies, advanced diagnostic methods, and improved patient management approaches.
The skin is the body’s largest and one of its most functionally complex organ, covering an average surface area of approximately 2 square meters, with a thickness of about 1.2 mm and contributing nearly 16% of total body weight. Its structural organization enables it to perform multiple essential functions that preserve homeostasis and protect the body from environmental hazards. As a defensive barrier, the skin shields internal tissues from harmful physical, mechanical, and chemical insults while limiting the entry of microbes, allergens, and irritants. Beyond its protective role as a physical and chemical barrier, the skin also regulates transepidermal water loss, prevents dehydration, participates in thermoregulation through sweat production and vasomotor responses, synthesizes vitamin D upon ultraviolet (UV) exposure, and houses sensory receptors that facilitate tactile, thermal, and pain perception.
A remarkable characteristic of the skin is its innate ability to regenerate and repair itself due to the continuous proliferation of epidermal keratinocytes. However, despite its resilience, the skin remains highly vulnerable to a wide variety of disorders because of its constant exposure to environmental factors, infectious agents, allergens, toxins, and ultraviolet radiation. Internal factors such as genetic susceptibility, hormonal imbalances, immune system alterations, and metabolic dysfunction further contribute to the development of numerous dermatological diseases [1,2,3].
Skin is categorized into two distinct types:
Infectious skin and soft-tissue diseases constitute one of the most commonly encountered conditions in clinical practice. These include bacterial infections such as cellulitis, erysipelas, impetigo, and deeper conditions such as necrotizing fasciitis; viral infections such as herpes simplex and herpes zoster; fungal infections like dermatophytosis and candidiasis; and parasitic infestations such as scabies. These conditions vary considerably in presentation, severity, and underlying pathology, with some infections associated with systemic symptoms such as fever. The incidence of several skin infections has significantly increased over recent decades, placing a substantial burden on healthcare systems [5-12].
The differential diagnosis of skin lesions is often complex because many infectious and non-infectious conditions can produce similar presentations, and a single disorder may manifest with multiple lesion types. Accurate identification of the underlying cause is therefore crucial for appropriate management [13, 14, 15, 16, 17].
Dermatological therapy encompasses a wide spectrum of approaches, including topical treatments, systemic medications, physical and light-based therapies, and surgical interventions. As the skin serves as the initial barrier against ultraviolet radiation, pathogens, chemicals, and allergens, many conditions are linked to disruptions in epidermal function. The epidermis comprises keratinocytes, melanocytes, Langerhans cells, gamma delta T-lymphocytes, and Merkel cells, each contributing uniquely to structural integrity, pigmentation, immune defence, and sensation [11,12].
SKIN ANATOMY [16-19]
Skin anatomy forms the structural and functional foundation for understanding dermatological disorders. The architectural organization of the skin determines how it responds to external stimuli, withstands mechanical forces, and maintains internal physiological balance. A clear understanding of this structure is crucial to interpreting how abnormalities or dysfunctions in specific layers contribute to disease development. With this perspective, the following section provides a detailed explanation of the two primary layers central to most skin conditions: the epidermis and the dermis.
EPIDERMIS
The epidermis is the outermost protective layer of the skin. It forms the body's primary barrier against the external environment and is the first tissue encountered in most dermatological conditions. This layer is responsible not only for providing physical protection but also for determining visible skin characteristics, including complexion and pigmentation.
The epidermis is approximately 0.01 cm thick, though this thickness varies across body regions. Despite its relatively small thickness, the epidermis plays a critical role in maintaining skin integrity through a highly organized system of cell types and layers.
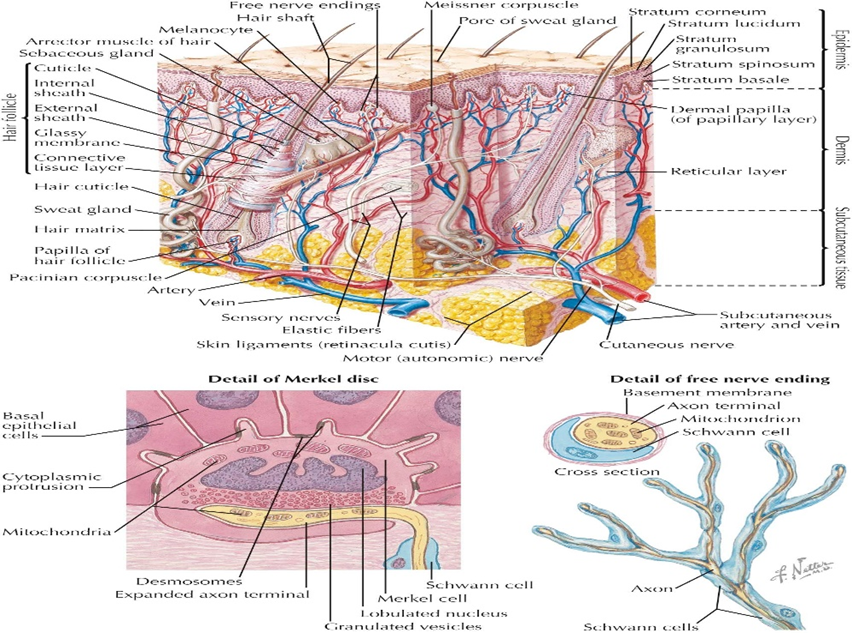
Figure 1: An anatomy of human skin layers
Cellular Composition of the Epidermis
The epidermis comprises a specialized arrangement of cells, each contributing to barrier function, pigmentation, immunity, and sensation. These include:
1. Keratinocytes
Keratinocytes make up 90–95% of the epidermal population. Their primary role is to synthesize keratin, a fibrous structural protein that provides strength and resilience. These cells originate in the basal layer and gradually migrate upward through the epidermal layers. During this journey, keratinocytes undergo morphological and biochemical changes, culminating in the formation of flattened, dead corneocytes in the stratum corneum.
2. Melanocytes
Melanocytes originate from the neural crest and reside predominantly in the basal layer. Their main function is to produce melanin, the pigment responsible for skin color. Melanin is synthesized within specialized organelles called melanosomes and transferred to surrounding keratinocytes. Two major forms of melanin—eumelanin (dark pigment) and pheomelanin (light pigment)—contribute to individual skin tone variation and UV protection.
3. Langerhans Cells
These dendritic immune cells function as antigen-presenting cells. They play a key defensive role by recognizing and internalizing foreign antigens encountered at the epidermal surface and initiating immune responses when pathogenic organisms or irritants penetrate the skin barrier.
4. Merkel Cells
Merkel cells are mechanoreceptors located within the basal layer. They interact with nerve endings to mediate tactile stimuli and are particularly important for fine-touch sensitivity.
Layered Organization of the Epidermis
The epidermis is composed of five distinct layers arranged from superficial to deep:
1. Stratum Corneum
The outermost layer consisting of dead, flattened corneocytes embedded in a lipid matrix. This layer serves as the main barrier against water loss and external chemical or microbial attack.
2. Stratum Lucidum
A thin, translucent layer found primarily in thick skin areas such as the palms and soles.
3. Stratum Granulosum
Characterized by keratinocytes containing keratohyalin granules, which are essential for keratin formation and barrier function.
4. Stratum Spinosum
Composed of polygonal keratinocytes connected by desmosomes, contributing to skin strength and flexibility.
5. Stratum Basale
The deepest layer containing proliferative keratinocytes, melanocytes, Merkel cells, and early-stage Langerhans cells. This is the regenerative zone responsible for replenishing the epidermal layers.
Keratinocytes continuously transition from the basal layer to the stratum corneum, undergoing differentiation processes that include lipid formation, protein synthesis, and eventually programmed cell death. This epidermal turnover cycle varies among individuals and can be influenced by age, disease, environmental exposure, and skincare practices.
DERMIS [20,21]
The dermis is the middle and structurally robust layer of the skin. It lies beneath the epidermis and above the hypodermis (subcutaneous tissue). The dermis provides the skin with strength, elasticity, and mechanical resistance due to its extensive network of collagen fibers, elastic fibers, and extracellular matrix.
Structural Components of the Dermis
1. Collagen Fibers
Collagen, particularly type I and III, is the main structural protein in the dermis. Its abundance provides tensile strength, preventing the skin from tearing under pressure or stretching forces.
2. Elastic Fibers
Elastic fibers contribute to the skin’s flexibility and allow it to return to its original shape after deformation. Although present in smaller quantities compared to collagen, elastin is essential for maintaining youthful skin properties.
3. Extrafibrillar Matrix
This matrix includes proteoglycans and glycosaminoglycans that attract and retain water, contributing to skin hydration and turgor.
4. Vascular and Neural Networks
The dermis contains an extensive system of blood vessels that supply nutrients to both the dermis and epidermis. It also houses nerve endings involved in sensations such as touch, pain, heat, and vibration.
5. Immune Cells
Fibroblasts, mast cells, macrophages, and other immune components reside in the dermis, contributing to wound healing, inflammatory responses, and defense mechanisms.
Dermal Subdivisions
The dermis is divided into two main layers:
1. Papillary Dermis
2. Reticular Dermis
Biomechanical Properties
Research on dermal biomechanics demonstrates that the skin exhibits nonlinear elastic behaviour, meaning it stretches easily under low tension but becomes increasingly resistant under higher stress. Collagen fibers realign and straighten during stretching, accounting for this pattern. Studies have shown that the Young’s modulus of human dermis is significantly lower than that of materials such as rubber, highlighting its compliant nature.
INFECTIOUS SKIN DISEASES
Infectious skin diseases represent a major portion of dermatological conditions encountered in clinical practice. They are caused by a diverse range of microorganisms including bacteria, viruses, fungi, and parasites. These infections may remain superficial or spread deeper into the dermis and subcutaneous tissues, occasionally becoming systemic. Their clinical presentation varies widely—from localized lesions to generalized rashes accompanied by fever—making diagnosis and management both crucial and challenging.
In recent decades, the incidence of skin and soft tissue infections (SSTIs) has risen significantly, with some studies reporting an increase of up to 65%, partly due to changes in pathogen resistance patterns, lifestyle behaviors, and comorbid conditions such as diabetes and immunosuppression. SSTIs encompass a broad spectrum of conditions, including cellulitis, erysipelas, impetigo, abscesses, necrotizing fasciitis, and infections following trauma or bites.
A major diagnostic challenge is that infectious and non-infectious dermatological conditions often share similar visual features, making clinical differentiation difficult. Additionally, a single disorder may present with multiple types of lesions due to the limited range of morphological manifestations the skin can produce in response to stimuli.
Below, each category of infectious disease is discussed in detail.
A. BACTERIAL INFECTIONS
Bacterial infections of the skin vary in depth, severity, and etiological agents. Common bacterial pathogens include Staphylococcus aureus, including methicillin-resistant strains (MRSA), and Streptococcus pyogenes.
1. Impetigo
A highly contagious superficial infection characterized by honey-colored crusts, most commonly affecting children. It often arises following minor skin trauma or insect bites.
2. Cellulitis
A deeper infection involving the dermis and subcutaneous tissue, typically presenting with warmth, swelling, pain, and erythema. Fever is common, and rapid progression may occur. Cellulitis frequently results from breaches in the skin barrier, such as wounds or fissures.
3. Erysipelas
A form of cellulitis involving the upper dermis and superficial lymphatics, characterized by sharply demarcated erythematous plaques. It is commonly associated with Streptococcus species.
4. Folliculitis
Inflammation and infection of the hair follicles, presenting as small pustules. It may progress to deeper infections.
5. Furuncles and Carbuncles
6. Abscesses
Localized collections of pus within the dermis or deeper tissue layers, typically requiring drainage.
7. Traumatic or Bite-Related Infections
Human or animal bites frequently introduce polymicrobial flora, leading to complicated infections involving both aerobic and anaerobic organisms.
8. Necrotizing Fasciitis & Fournier Gangrene
Severe, rapidly progressive infections involving the fascia, associated with high mortality. Early recognition and aggressive intervention are essential.
9. Leprosy (Hansen’s Disease)
A chronic granulomatous infection caused by Mycobacterium leprae. It affects skin, peripheral nerves, and mucosal surfaces. Manifestations range from hypopigmented patches with sensory loss to nodular and diffuse skin thickening. Disease type depends on host immune response.
B. VIRAL INFECTIONS
Viral pathogens commonly affect the skin and may cause localized or widespread manifestations.
1. Herpes Simplex Virus (HSV)
Both viruses establish latency in sensory ganglia and may reactivate during stress, illness, or immunosuppression.
2. Herpes Zoster (Shingles)
Reactivation of varicella-zoster virus (VZV) produces painful vesicles distributed along a dermatome. Post-herpetic neuralgia is a common complication.
3. Warts
Caused by human papillomavirus (HPV), warts may appear on hands, feet, face, or genital areas. Over 100 HPV types exist, each associated with distinct lesion morphologies.
4. Molluscum Contagiosum
A poxvirus infection presenting as small dome-shaped papules with central umbilication. It spreads through direct contact and is common in children and immunocompromised individuals.
C. FUNGAL INFECTIONS
Fungal infections are classified as superficial, cutaneous, or systemic, depending on tissue depth.
1. Dermatophytosis (Ringworm)
Caused by fungi of the genera Trichophyton, Microsporum, or Epidermophyton.
Common types include:
These infections thrive in warm, moist environments and frequently recur.
2. Yeast Infections (Candidiasis)
Candida species cause intertrigo, oral thrush, and genital infections. They particularly affect individuals with diabetes, obesity, or compromised immunity.
D. PARASITIC SKIN DISEASES
Parasitic organisms can invade or reside on the skin, causing intense inflammation, itching, and sometimes secondary infections.
1. Scabies
Caused by the mite Sarcoptes scabiei, which burrows into the skin to lay eggs. This results in severe itching, especially at night, and characteristic burrow lines.
2. Pediculosis (Lice Infestations)
Includes infestation of:
Lice feed on human blood and cause itching, irritation, and excoriations.
3. Cutaneous Larva Migrans
A condition caused by hookworm larvae penetrating the skin. It presents with serpiginous, migrating tracks and intense itchiness.
E. DIAGNOSTIC COMPLEXITY IN INFECTIOUS DISEASES
Because many infectious and non-infectious disorders share overlapping clinical signs—such as rashes, papules, vesicles, or erythema—accurate diagnosis requires careful evaluation. Diagnostic difficulty arises from:
Certain febrile illnesses, for instance, present with exanthems where rash + fever may indicate viral infections, drug reactions, or autoimmune flare-ups.
INFLAMMATORY AND AUTOIMMUNE SKIN DISEASES
Inflammatory and autoimmune skin diseases are among the most prevalent chronic dermatological conditions. They arise from complex interactions involving genetic predisposition, epidermal barrier defects, environmental triggers, microbial imbalance, and dysregulated immune responses. These disorders are often characterized by recurrent or persistent inflammation, altered keratinocyte activity, and immune cell infiltration, which together produce visible skin changes such as redness, scaling, thickening, itching, and pigmentary alterations.
A notable feature of inflammatory skin diseases is that the clinical manifestations often overlap, making differential diagnosis challenging. Many disorders exhibit combinations of erythema, papules, vesicles, plaques, scaling, or excoriations. Additionally, these diseases frequently worsen in response to triggers such as stress, allergens, infections, hormonal fluctuations, and climatic changes.
Below is a detailed discussion of major inflammatory and autoimmune conditions.
A. ECZEMA / ATOPIC DERMATITIS (AD) [22]
Atopic dermatitis is a chronic, relapsing inflammatory skin disorder characterized by intense pruritus, xerosis, and eczematous lesions. It is commonly associated with other atopic conditions such as allergic rhinitis and asthma.

Figure 2: Atopic dermatitis
Etiology
AD is multifactorial and involves:
Clinical Features
B. ALOPACIA [23]
One of the more common dermatologic complaints seen by dermatologists and primary care physicians is alopecia or hair loss. The term pattern hair loss (PHL). Coverup techniques can be effective and there are many nonmedical treatments for PHL such as platelet-rich plasma injection, hair transplantation, or laser/light treatment.

Figure 3: Alopecia
C. PSORIASIS
Psoriasis is an immune-mediated disorder characterized by hyperproliferation of keratinocytes and chronic inflammation. It is driven primarily by Th1 and Th17 pathways, with TNF-α playing a major role.
Pathophysiology
Types of Psoriasis
Triggers
C. SEBORRHEIC DERMATITIS
A chronic inflammatory disease affecting sebaceous gland-rich areas (scalp, face, chest). It is associated with:
Features
D. CONTACT DERMATITIS
Occurs when skin comes into contact with substances that cause irritation or allergy.
Types
E. AUTOIMMUNE SKIN DISEASES
These conditions occur when the immune system mistakenly targets skin components.
1. Lupus Erythematosus (Cutaneous Lupus)
Characterized by:
2. Dermatomyositis
An inflammatory myopathy with distinctive cutaneous manifestations.
Cutaneous signs
Often associated with muscle weakness and systemic abnormalities.
3. Scleroderma
A connective tissue disorder involving excessive collagen deposition.
Cutaneous features
4. Vitiligo (Autoimmune Melanocyte Destruction)
Vitiligo is a pigmentary autoimmune condition, but your text places it partly under inflammatory disorders so it is included here as well.
Pathogenesis
Clinical Presentation
F. PERIORIFICIAL DERMATITIS
A chronic inflammatory facial condition affecting the perioral, perinasal, and periocular areas.
Etiology
Often triggered by:
Clinical Features

Figure 4: Periorificial dermatitis
Management
“Zero therapy” — stopping all irritants, especially topical steroids — is a core part of treatment.
ACNE VULGARIS [24-29]
Acne vulgaris is one of the most common dermatological disorders, affecting adolescents, young adults, and in many cases, persisting into adulthood. Although traditionally viewed as a self-limited condition of puberty, acne is now recognized as a chronic inflammatory disorder of the pilosebaceous unit. Its development is influenced by a combination of hormonal, microbial, genetic, environmental, and immunological factors. Acne often involves the face, chest, shoulders, back, and upper arms—regions with high densities of sebaceous glands.
The condition has a significant impact on psychological well-being, social functioning, and self-esteem. Persistent or severe acne can lead to permanent scarring, making early recognition and intervention essential.
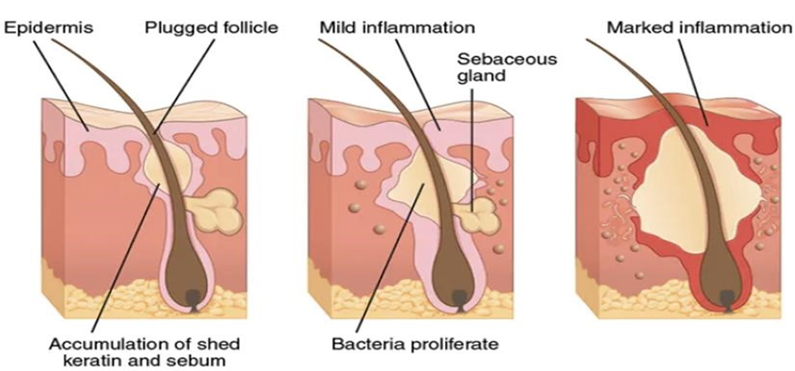
Figure 2: The process of acne formation on the skin
A. ETIOLOGY OF ACNE
Acne results from a coordinated sequence of events affecting the pilosebaceous unit:
1. Increased Sebum Production
One of the earliest changes in acne pathogenesis is androgen-driven sebum overproduction. During puberty, elevated levels of androgens stimulate the sebaceous glands to enlarge and produce excessive sebum.
Key points:
2. Follicular Hyperkeratinisation
The normal shedding of keratinocytes at the follicular opening becomes disrupted. Instead of exfoliating, keratinocytes accumulate and mix with sebum, forming a keratinous plug (microcomedone).
This process includes:
3. Microbial Colonization by Cutibacterium acnes (C. acnes)
Formerly known as Propionibacterium acnes, this anaerobic bacterium flourishes in lipid-rich environments. Although part of normal skin flora, it becomes pathogenic when conditions inside the follicle change.
C. acnes contribute to acne through:
Different phylotypes of C. acnes may vary in inflammatory potential.
4. Inflammation
Inflammation is now understood to be present at every stage of acne, even before visible lesions appear. The inflammatory cascade is amplified by:
Inflammatory lesions include papules, pustules, nodules, and cysts. Severe inflammation often leads to post-inflammatory hyperpigmentation (PIH) and scarring.
B. TYPES OF ACNE LESIONS
Acne lesions are classified into non-inflammatory and inflammatory types.
1. Non-inflammatory Lesions
These lesions form the foundation of acne and indicate abnormal keratinization.
2. Inflammatory Lesions
Inflammatory lesions result from microbial proliferation, immune activation, and follicular rupture:
C. FACTORS THAT CONTRIBUTE TO ACNE DEVELOPMENT
1. Hormonal Influences: Puberty-associated androgens, polycystic ovarian syndrome (PCOS), menstrual cycle fluctuations, exogenous hormones or anabolic steroids.
2. Diet: Gradually, scientific evidence supports associations between acne and: High-glycaemic foods (sugary and processed foods), dairy products, whey protein, diets high in saturated fats.
These substances stimulate IGF-1 pathways, enhancing sebum production and keratinocyte proliferation.
3. Stress: Stress increases cortisol secretion, which can exacerbate inflammation and sebum production.
4. Genetics: A strong familial tendency exists. Multiple genes regulate sebum production, inflammatory pathways, and keratinization.
5. Cosmetic and Occupational Factors: Heavy, oily cosmetics (“comedogenic” products), Exposure to greasy environments (mechanics, cooks), occlusive clothing or helmets.
6. Medications: Certain drugs can trigger or worsen acne, including: Corticosteroids, lithium, isoniazid, phenytoin, vitamin B12 (high doses).
D. COMPLICATIONS OF ACNE
1. Scarring
Severe inflammatory acne leads to permanent scars:
2. Pigmentary Changes
3. Psychological Effects
Acne significantly impacts:
PIGMENTATION DISORDERS [30-33]
Pigmentation disorders represent a group of conditions in which the production, distribution, or survival of melanocytes or melanin is disrupted. Melanin, synthesized by melanocytes in the basal epidermal layer, plays a vital role in determining skin, hair, and eye color and provides protection against ultraviolet (UV) radiation.
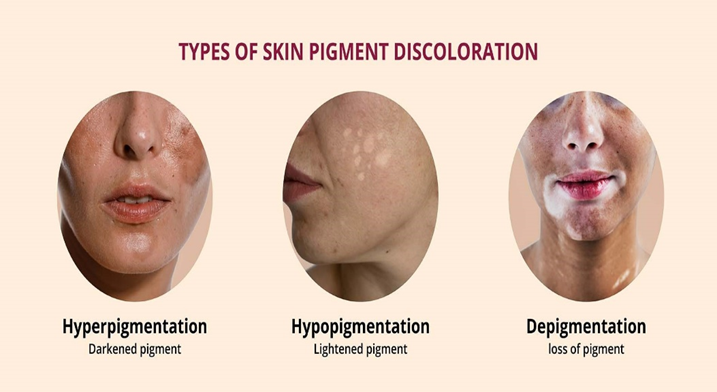
Figure 5: Types of pigmented skin
These disorders may arise from:
Pigmentation disorders are broadly classified into hypopigmentation (loss or reduction of pigment) and hyperpigmentation (increased pigmentation).
Among the most common and clinically significant pigmentary conditions are Vitiligo, Melasma, and Post-Inflammatory Hyperpigmentation (PIH), each of which is discussed in detail below.
A. VITILIGO [34-36]
Vitiligo is a chronic pigmentary disorder characterized by the development of well-defined depigmented macules and patches. It results from the selective destruction or dysfunction of melanocytes, leading to complete absence of melanin in affected areas.
It affects individuals of all ages and ethnicities, with significant psychosocial impact due to changes in appearance.
Etiology and Pathogenesis
Vitiligo arises through a multifactorial process involving:
1. Autoimmune Mechanisms
2. Genetic Predisposition
3. Oxidative Stress
4. Neural Hypothesis
5. Environmental and Triggering Factors
Clinical Features
Vitiligo often shows unpredictable progression, with periods of stability alternating with rapid spread.
B. MELASMA [37]
Melasma is a chronic acquired hyperpigmentation characterized by light-to-dark brown patches, typically occurring on sun-exposed areas such as the face (cheeks, forehead, upper lip). It is more common in women and individuals with darker skin types.
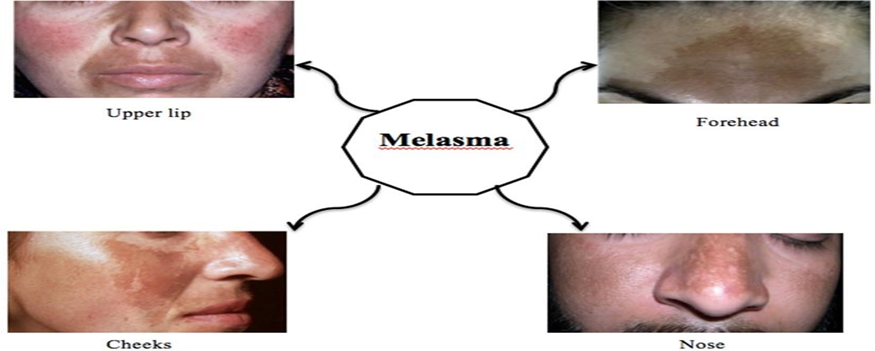
Figure 6: Irregular brown macules of melasma on common parts of the face: upper lip, forehead, cheeks and nose.
Etiology
Melasma results from increased melanin production and deposition. Key contributing factors include:
1. Ultraviolet Exposure
2. Hormonal Influences
3. Genetic Predisposition
4. Phototoxic and Cosmetic Products
Some perfumes, oils, and skin-care products irritate the skin, worsening pigmentation.
5. Thyroid Disorder Associations
Hypothyroidism or autoimmune thyroid disease may influence melanocyte sensitivity.
Clinical Presentation
Melasma appears as:
The condition is chronic, often exacerbated by sunlight and heat, and has a tendency to relapse.
C. POST-INFLAMMATORY HYPERPIGMENTATION (PIH)
PIH is an acquired condition where inflammation or injury to the skin triggers excess melanin production, leading to dark discoloration.
Causes
PIH can follow:
In darker skin types (IV–VI), PIH is especially common and often more intense.
Pathogenesis
Inflammatory mediators—such as prostaglandins, leukotrienes, and cytokines—stimulate melanocytes to increase melanin production. Depending on the depth of melanin deposition:
The condition worsens with UV exposure because inflammation increases melanocyte sensitivity to sunlight.
Clinical Features
WOUND HEALING AND IMPAIRED WOUND REPAIR [38,39]
Wound healing is a vital biological process that restores the structural and functional integrity of skin after injury. This complex sequence involves coordinated interactions among cells, extracellular matrix components, cytokines, chemokines, growth factors, and the vascular system. A normal wound-healing response progresses through four well-defined phases: haemostasis, inflammation, proliferation, and remodelling. Disruption in any of these stages can result in chronic non-healing wounds, abnormal scarring, or delayed tissue repair.
Wound healing can be influenced by systemic conditions (such as diabetes, age, nutritional status, vascular insufficiency, and immune disorders) as well as local factors (infection, repeated trauma, skin tension, and improper wound care).
A. PHASES OF NORMAL WOUND HEALING
Wound healing follows a highly regulated, overlapping sequence of events.
1. Haemostasis Phase
This phase begins immediately after injury.
The hemostatic plug also acts as a reservoir of cytokines that regulate later stages.
2. Inflammatory Phase
This phase clears pathogens and debris from the wound bed.
Key events:
This phase typically lasts 2–3 days, but can extend longer in infected or chronic wounds.
3. Proliferative Phase
The proliferative phase restores tissue continuity and involves:
A. Fibroblast Activation
B. Angiogenesis
C. Granulation Tissue Formation
D. Re-epithelialization
4. Remodelling (Maturation) Phase
This final phase may last months to years.
Major changes include:
Replacement of type III collagen with type I collagen, cross-linking and alignment of collagen fibers, increase in wound tensile strength (though healed wounds reach only ~80% of original strength), reduction in blood vessels and cellularity as scar matures, abnormalities during this phase can lead to hypertrophic scars or keloids.
B. IMPAIRED WOUND HEALING
When any component of the healing cascade is disrupted, wounds may heal slowly or incompletely, leading to chronic non-healing wounds.
Impaired wound healing may result from:
1. Systemic Factors
Diabetes Mellitus: High glucose levels impair neutrophil activity, reduced collagen synthesis, poor microcirculation, increased susceptibility to infection.
Advanced Age: Slower keratinocyte migration, reduced fibroblast activity, lower angiogenic response
Malnutrition: Deficiencies in proteins, vitamins (A, C, E), and minerals (zinc, iron) delay repair.
Immunosuppression: Due to medications, HIV, or systemic disease → decreases inflammatory response.
2. Local Factors
Repetitive Trauma or Pressure: Seen in pressure ulcers or wounds over bony prominences.
Hypoxia: Poor oxygenation impairs fibroblast function and collagen synthesis.
Excessive Wound Exudate: Breaks down the extracellular matrix and delays re-epithelialization.
C. ROLE OF PEPTIDES IN WOUND HEALING (FROM YOUR ORIGINAL TEXT)
Recent research highlights the promising role of therapeutic peptides in accelerating wound repair. These peptides may:
Examples include:
Their capabilities make them potential candidates for new wound care treatments.
Figure 7: Cyclic peptides as wound healing compounds
D. CLINICAL SIGNIFICANCE
Understanding wound healing is essential because:
Chronic wounds are major health burdens, diabetic ulcers, venous ulcers, and pressure sores lead to high morbidity, early identification of impaired healing improves outcomes, advanced therapies (peptides, growth factors, biomaterials) rely on a clear grasp of underlying mechanisms.
KUSHTHA (AYURVEDIC PERSPECTIVE ON SKIN DISORDERS)
In Ayurveda, skin diseases are collectively described under the umbrella term “Kushtha.” This term encompasses a wide spectrum of dermatological conditions, ranging from mild discolorations to chronic, deeply seated, and debilitating skin disorders. Classical Ayurvedic texts describe Kushtha as a pathological state arising from vitiation of the three fundamental doshas—Vata, Pitta, and Kapha—along with disturbances in essential body tissues (Dhatus) and waste products (Malas).
Ayurvedic literature identifies Mahakushta (major skin disorders) and Kshudra Kushtha (minor skin disorders), based on severity, chronicity, and involvement of tissues. Although the exact correlation between Ayurvedic descriptions and modern dermatological conditions varies, the fundamental principles emphasize internal imbalance, lifestyle factors, diet, and environmental exposures as key triggers for skin disease.

Figure 8: Kustha
A. ETIOLOGY OF KUSHTHA [40,41]
Ayurveda attributes the origin of Kushtha to a combination of dietary, behavioral, environmental, and constitutional factors. These causative elements disturb the normal functioning of doshas and dhatus, leading to pathological skin manifestations.
1. Dietary Causes (Ahara)
Certain foods and dietary habits are considered potent triggers for Kushtha:
These dietary practices impair metabolism and digestion, leading to toxin accumulation (Ama) in the body.
2. Behavioral Causes (Vihara)
Such behaviors disrupt doshic balance and affect skin integrity.
3. Psychological Factors
Emotional disturbances, particularly chronic stress, fear, grief, and anger, are believed to aggravate doshas and weaken immune defenses, contributing to the onset and persistence of skin diseases.
4. Environmental Contributors
Exposure to extremes of climate, polluted surroundings, or contaminated water and soil are recognized as aggravating elements that disturb the skin’s natural protective functions.
B. PATHOGENESIS OF KUSHTHA (SAMPRAPTI)
The pathogenesis involves:
A combination of these events results in chronic, recurrent skin conditions that are difficult to treat without addressing the root imbalance.
C. TYPES OF KUSHTHA
Ayurvedic classics categorize Kushtha into two broad divisions:
1. Mahakushta (Major Skin Disorders): These are severe, deeper, and chronic disorders involving multiple tissues and intense doshic imbalance.
2. Kshudra Kushtha (Minor Skin Disorders): These are milder and more superficial conditions with less systemic involvement.
Although the texts describe 18 types of Kushtha, specific classification varies among classical treatises.
D. CLINICAL FEATURES OF KUSHTHA
A wide variety of symptoms may appear depending on doshic dominance:
Vata-dominant Kushtha
Pitta-dominant Kushtha
Kapha-dominant Kushtha
Most skin disorders in Kushtha manifest as combinations of these features, reflecting mixed dosha involvement.
E. MANAGEMENT OF KUSHTHA
Ayurvedic management emphasizes treating both the root cause and clinical manifestations through internal purification, external applications, and sustainable lifestyle modifications.
1. Nidan Parivarjana (Avoidance of Causative Factors):
Avoid incompatible foods, reduce oily, heavy meals, avoid day-time sleeping, correct sedentary habits, minimize exposure to irritants.
Eliminating such triggers supports restoration of normal doshic balance.
2. Shodhana (Purification Therapy)
These detoxification procedures remove toxins and deeply seated doshic imbalances:
These therapies are performed under professional supervision.
3. Shamana (Palliative Therapy)
Aim to balance doshas without intense purification:
Popular formulations include:
4. External Therapies (Bahya Chikitsa)
Ayurvedic external therapies help reduce inflammation, itching, and scaling:
These treatments soothe the skin and improve circulation.
SKIN CANCERS [42-43]
Skin cancer refers to the abnormal, uncontrolled growth of skin cells, primarily triggered by DNA damage and mutations—most commonly caused by ultraviolet (UV) radiation from sunlight or artificial sources. It represents one of the most common malignancies worldwide. Skin cancer is broadly classified into melanoma and non-melanoma skin cancers (NMSCs), each with distinct biological behavior, risk factors, molecular pathways, and prognosis.
Melanoma is the most aggressive form, arising from melanocytes, whereas non-melanoma cancers—mainly basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)—originate from keratinocytes. Each type involves different molecular mechanisms, with several signaling pathways implicated in tumor initiation, proliferation, angiogenesis, and metastasis.
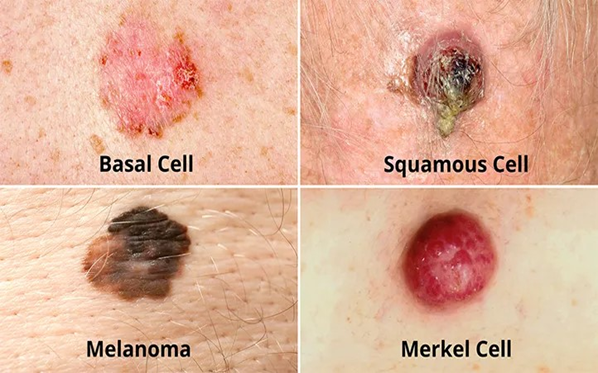
Figure 9: Types of skin cancer
A. MELANOMA
Melanoma is a malignant tumor that develops from melanocytes, the pigment-producing cells located in the basal layer of the epidermis.
1. Etiology and Risk Factors
A. UV Radiation
B. Genetic Predisposition
C. Phenotypic Factors
D. Immunosuppression
Individuals with compromised immune function (e.g., transplant patients) show higher incidence rates.
2. Molecular Pathogenesis
Multiple pathways are implicated in melanoma progression:
A. Wnt Signaling Pathway
B. TGF-β (Transforming Growth Factor-β) Pathway
C. Role of lncRNAs (Long Non-Coding RNAs)
D. EMT (Epithelial–Mesenchymal Transition) Proteins
3. Clinical Features
Melanoma may present as:
The ABCDE rule (Asymmetry, Border, Color, Diameter, Evolution) helps identify suspicious lesions.
B. NON-MELANOMA SKIN CANCERS (NMSCs)
Non-melanoma cancers include basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). They are more common but generally less aggressive compared to melanoma.
1. Basal Cell Carcinoma (BCC)
BCC arises from basal keratinocytes of the epidermis.
Etiology
Clinical Features
2. Squamous Cell Carcinoma (SCC)
SCC develops from atypical keratinocytes in the epidermis.
Risk Factors
Clinical Features
C. NICOTINIC ACETYLCHOLINE RECEPTORS IN SKIN CANCER (Referenced in Your Text)
Your original text highlighted the role of α7-nAChR (alpha-7 nicotinic acetylcholine receptor). This receptor:
Abnormal activation of α7-nAChR pathways promotes aggressive tumor behavior.
D. ONCOTAG: A NOVEL PEPTIDE THERAPY (From Your Original Text)
Your content referenced Oncotag, an innovative peptide designed to inhibit tumor progression.
Key Points:
This highlights the growing interest in peptide-based anticancer therapies.
E. CLINICAL IMPORTANCE
Understanding the molecular basis of melanoma and NMSCs is vital because:
CONCLUSION
Skin disorders encompass a remarkably broad spectrum of conditions that differ in their causes, clinical patterns, severity, and long-term implications, largely because the skin functions as a dynamic interface between the body and the external environment and is therefore vulnerable to microbial invasion, immune disturbances, chemical and physical insults, hormonal influences, and genetic factors. This review highlighted the structural and functional organization of the skin and explained how disruptions in keratinocytes, melanocytes, immune components, collagen, elastin, and barrier integrity contribute to disease development. The major groups of dermatological disorders—including infections, inflammatory and autoimmune diseases, acneiform conditions, pigmentation anomalies, impaired wound repair, Ayurvedic concepts such as Kushtha, and skin cancers—each arise through distinct yet overlapping biological mechanisms. Infectious diseases emerge from microbial entry, whereas inflammatory disorders reflect immune dysregulation; pigmentation conditions result from altered melanocyte behavior; wound-healing problems follow disturbances in tissue repair or microcirculation; and cancers evolve from accumulated genetic and molecular abnormalities. Understanding processes such as keratinocyte overproliferation, oxidative stress, T-cell activation, cytokine shifts, melanocyte loss, collagen degradation, and oncogenic mutations—as well as pathways like Wnt signaling, TGF-β modulation, α7-nicotinic acetylcholine receptor activity, and long non-coding RNA regulation—provides deeper insight into the complexity of these diseases. Recent progress in peptide-based therapeutics, including wound-repair peptides and targeted anticancer agents like Oncotag, further expands treatment possibilities. As dermatological disorders continue to rise globally due to environmental changes, lifestyle factors, and increasing microbial resistance, early diagnosis, accurate classification, and integrated management strategies have become increasingly important. Combining modern dermatological science with traditional approaches such as Ayurveda may offer added value, especially for chronic and recurrent conditions. Ultimately, continued progress in understanding the molecular, cellular, and immunological foundations of skin diseases will support the development of more effective therapies and improve outcomes and quality of life for affected individuals.
REFERENCE


Aparna Kante, Dr. Sudha Parimala, A Comprehensive Review of Major Skin Disorders: Etiology, Pathophysiology and Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 3958-3982. https://doi.org/10.5281/zenodo.17711276
 10.5281/zenodo.17711276
10.5281/zenodo.17711276
