School of Pharmacy, G.H. Raisoni University, Saikheda Dist- Pandhurna, Madhya Pradesh, India 480334
One of the most frequent lesions of the oral mucosa is oral ulcers, which is usually accompanied by pain, inflammation, and poor quality of life. Traditional treatments, in spite of their some level of effectiveness, are usually restrained by the side effects, recurrence, and cost. This has led to an increasing interest on natural agents that have reported therapeutic value. Alum (potassium aluminium sulphate) and turmeric (Curcuma longa) have traditional medical uses in the treatment of the oral cavity, since their pharmacological property range is quite extensive. Alum has astringent effects, microbiocidal effects and haemostatic effects that aid in decreasing inflammation and healing of the ulcers. Curcumin-rich turmeric has strong anti-inflammatory, antioxidant, antimicrobial, and wound-healing effects that are also associated with regenerative action of the mucosal, and analgesic effects. New preclinical and clinical data demonstrate their synergistic effect in the oral ulcer treatment, which offers an alternative to synthetic drugs in the management of oral ulcers, as a naturally-derived, safe, and economical option. This review summarizes the existing scientific evidence on the phytochemistry, pharmacology, formulation, and therapeutic effect of alum and turmeric on the treatment of oral ulcers. It also talks about restrictions and safety with regard to the future research of creating optimized formulations. The results indicate that alum and turmeric, alone or in combination, have great potential as natural therapeutics in the treatment of oral ulcers, and that should be explored further via well-designed clinical trials
Oral ulcer Oral/ mouth ulcers are painful lesions that are open blisters or canker blisters. Gums, lips, inner cheeks, and palate ulcers can develop in the mouth. A mouth ulcer is the loss or corrosion of the mucosal membrane, the fragile towel that lines the mouth. Keep in mind that mouth blisters are distinct from cold blisters, which are brought on by a contagion that manifests itself in the lips. Canker blisters, cold blisters, leucoplakia( a thick white or slate area), and candidiasis are Causes of mouth ulcers.[1]

Figure 1: Mouth Ulcer
One of the most common types of oral ulcers is known as aphthous ulcers otherwise known as canker sore. Such lesions are often associated with systemic complications (stress, nutrition deficiency (vitamin B12, folate, or iron deficiency), and certain autoimmune diseases). Aphthous ulcer can look like small round or oval blisters, lined with a greyish-white tissue with a clear red edge on them. They we commonly found on non-keratinized epithelial surfaces, including the inside of the cheeks, the lips and the tongue. The characteristic of aphthous ulcers is that they can heal independently during 10-14 days without the need to be promptly treated.
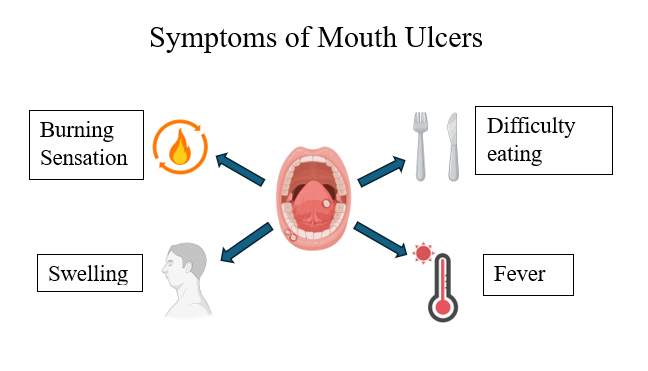
Figure 2: Symptoms of mouth ulcers
Painful lesions in the mouth cavity are the primary symptom of mouth ulcers. The secondary signs may include:
The types of mouth ulcers are categorized below:
Types of oral ulcer:
Based on the lesions:
1. Minor ulcers- These are 2 to 8 mm wide and often go away in 10 to 2 weeks. The discomfort from this ulcer is not severe.
2. Major ulcers- These are broad, deep, and may have an uneven or elevated border.[1]
What causes mouth ulcers?
The etiology of mouth ulcers is unclear. Nevertheless, so many factors can cause the occurrence of these blisters. Moral trauma: Injury of the towels, during dental work, minor, but similar to having a tooth filled.
Signs and symptoms :
Pathophysiology:
The precise pathogenesis is determined by the cause.
Etiology:
The etiology of mouth ulcers has not been clearly defined. It is considered to be multifactorial, with contributing factors including stress, trauma, injury due to biting of the mucosal layer, spicy or highly acidic foods, genetic makeup, poorly fitted dental appliances, etc. It may be due to nutritional deficiencies of riboflavin, niacin, folic acid, cobalamin, ascorbic acid, iron, and calcium. The erosion of the oral mucosal membrane may occur due to rough brushing, a harsh dental care routine, or damage caused by chewing, eating, etc. The oral ulcers may develop as a result of underlying systemic diseases or medications administered to treat those diseases.
Healing mechanisms in oral mucosa:
Wound healing is a complex biological process that is essential to regain tissue integrity and function. Cutaneous wounds, injuries to the skin, and oral mucosal wounds, injuries in the mucous membranes of the oral cavity, follow well-defined phases during wound healing involving coordinated cellular and molecular events. Wound healing in skin and oral mucosa shares many common cellular and molecular processes; however, there are also notable differences due to the distinct characteristics and functions of these two tissue types. Oral mucosal wounds possess some unique characteristics, benefiting from the rapid turnover of cells and the presence of a protective mucus layer that expedites the healing process and protects against further damage.[9]
Conventional approaches to oral ulcer management:
Standard therapies for oral ulcers, especially recurrent aphthous stomatitis (RAS), primarily focus on alleviating pain, accelerating the healing process, minimizing lesion size, and — when feasible — lowering the frequency or intensity of recurrences. Many common treatments are aimed at symptom relief and consist of topical anti-inflammatory agents, antiseptics, pain relievers, and, for more serious cases, systemic immunomodulatory therapy.[10]
If combined treatment with topical anesthetics and anti-inflammatory agents is not effective, then topical corticosteroids should be employed.[10]
Adhesive pastes, gels, or films (such as triamcinolone paste, sucralfate suspension, amlexanox oral adhesive) form a protective layer, alleviate pain, and may speed up the healing process by shielding the ulcer from additional trauma and facilitating local drug absorption. Evidence from small studies suggests that sucralfate suspensions can provide pain relief and shorten healing times. The adhesive form of amlexanox (which acts as an anti-inflammatory and anti-allergic agent) has been utilized to lessen pain and reduce the duration of symptoms.[11]
For recurrent, extensive, or debilitating ulcers, systemic treatment is recommended. Brief courses of systemic corticosteroids can alleviate pain and promote healing. Immunomodulatory medications (such as dapsone, colchicine, azathioprine, and thalidomide) have been employed for severe recurrent aphthous stomatitis or when ulcers are linked to systemic conditions, but many have significant side effects and need specialist management. Recent meta-analyses continue to assess the effectiveness versus risks of medications like thalidomide.[12]
Topical anesthetics like gels containing benzocaine and systemic pain relievers can assist in managing discomfort. Non-pharmacological options include low-level laser therapy or photobiomodulation, which has demonstrated effectiveness in relieving pain and promoting quicker healing in several small studies, as well as cautery and protective splints for ulcers caused by trauma. When deficiencies are detected, it is advisable to correct nutritional imbalances through oral supplements such as iron, folate, and B-vitamins.[13]
Recognizing and addressing local traumatic elements (such as sharp teeth or poorly fitting dental appliances), improving oral hygiene practices, steering clear of known irritants (like specific foods or toothpastes containing sodium lauryl sulfate in sensitive individuals), and educating patients on the importance of prompt topical treatment constitute the fundamental principles of conservative preventive strategies. In cases where systemic conditions or nutritional deficiencies exist, it is crucial to address the root cause.[14]
Numerous traditional therapies offer symptom relief but often fail to consistently prevent future occurrences. There are few large-scale randomized controlled trials directly comparing contemporary bioadhesives, topical immunomodulators, lasers, and systemic therapies, and the long-term safety information, especially concerning systemic immunomodulators, is lacking. New biomaterials and focused local delivery systems are being studied to address these challenges.[14]
Traditional Medicine and Natural Approaches:
History:
Over the past few years, herbal oral health care products have become a trend due to their perceived efficacy and effectiveness, and potential natural and holistic benefits to oral health.[15] This increasing interest is based on the fact that some of these plant extracts have anti-inflammatory, antibacterial and oxidative properties which could combat the bacteria that cause dental plaque as well as reduce the level of inflammation in the gums.[16] Therefore a number of oral care product manufacturers and multinational corporations have incorporated a number of herbal components in their products purporting to imitate the benefits of the plaque, breath freshening, as well as the prevention of gum diseases.[17] These are often a mixture of botanical extract, essential oil and other natural ingredients which have a therapeutic nature. The most common herbal ingredients that are combined into oral care products include: akarkara (Anacyclus pyrethrum), babool (Acacia arabica), haldi (Curcuma longa), sanguinarine, propolis, neem (Azadirachta indica), charcoal, green tea (Camellia sinensis), clove and miswak.[18]
Ayurvedic and Folk practices:
Approximately 3.5 billion individuals throughout the globe are believed to have a vast number of oral illnesses, including dental caries (tooth decay), periodontal (gum) disease, tooth loss, and oral cancers.[19] Since oral diseases are strongly linked to socioeconomic situation (income, education and occupation) and social determinants of health, oral diseases become a very grave problem in the society as the poor, the marginalized and socially disadvantaged get increasingly affected. Moreover, there are some adverse effects to oral disease treatment including teeth stains, oral mucosal peeling and allergic contact stomatitis. Contrary to the above, alternative methods have been reported to be using other traditional methods and herbal products, which can result in forthcoming treatment of oral diseases. Given that traditional medicine is cheap, safe, readily available, and culturally oriented, the use of medicinal plants and herbal drugs is taking the place of primary health care in most regions of the world. To give an example, natural phytochemicals that have been obtained in plants are deemed as good substitutes to synthetic chemicals that are employed in dental issues treatment. The Ayurvedic medical substances are safe and effective by several hundred to several thousand years of application.[20]
Commonly used herbal plants:
Triphala,: Which is an Ayurvedic preparation, is one such panacea to cure the aphthous ulcers since the preparation has a broad range of action in cases of such lesions with virtually no side effects. The case report provides an account of the effectiveness of Triphala oral rinse in treating minor aphthous ulcers on a 21-year-old male patients.[21]
Curcumin: The root of Curcuma longa is a native Asian plant of the Zingiberaceae family and yields curcumin (diferuloylmethane), the most active portion of the turmeric. Carcinogenic has also been known since ancient times to have therapeutic effects (curing, antioxidant, antifungal, anti-inflammatory, antidepressant, adjuvant to chemo and radiation therapy, hypoglycemic) and several scientific studies have substantiated these properties today. Its antioxidant activity is especially relevant in case of oral mucositis, in which curcumin is used to alleviate oxidative stress that is among the major contributors to mucosal damage in chemotherapy and radiation therapy.[22]
Aloe vera: Among the most notable therapeutic plants in folk medicine all over the world is the plant of immortality, aloe vera. Among all the species of aloe, it is the most bioactive one.[23] At least it has an approximate of 75 biologically active ingredients like vitamins, enzymes, minerals, sugars, steroids, hormones, saponins, amino acids and phenolic compounds. It is anti-inflammatory, anti-oxidant, cytoprotective, immunomodulatory, wound healing and anti-tumor. As per these biological processes, Aloe vera may be employed in the GU healing process.[24]
ALUM:
Alum, a traditional Chinese mineral medicine (major component: KAl(SO4)2·12H2O), possesses pharmacological effects including antibacterial, hemostatic, antidiarrheal, and cholagogic properties.[25] For over two thousand years, it has been used to treat conditions in dermatology, anorectal surgery, stomatology, otolaryngology, and burn care.[26]

Figure 3: Alum
Alum In Oral Ulcer Management
RAS, also known as canker sores, affects the oral mucosa and is caused by such factors as trauma, nutritional deficiencies, infections, and systemic conditions. The antimicrobial activity of alum was measured through agar well diffusion where it was found to be inhibitive to both microorganisms such as Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, Bacillus subtilis, Proteus vulgaris, Candida albicans, Penicillium digitatum and Aspergillus niger with the maximum inhibition zones being 20 per cent of Pseudomonas aeruginosa(26mm) and Candida albicans.[27]
Background And Traditional Uses Of Alum
Background:
In the Natural History of Pliny, the term alum is used. Pliny tells us that natural alum was discovered on the earth. He calls it ‘salsugoterrae’. Potassium Aluminium Sulphate (Potash alum) is an inorganic salt. It is colorless, crystalline, massy, or granular powder of a sweetish astringent flavour, odourless, and transparent.[28]
Traditional Uses Of Alum:
Alum is a naturally occurring inorganic chemical which has significant application in both traditional and modern medicine. It possesses extensive medicinal values of alum which include antihemorrhagic, antifungal, antibacterial, anti-obesity, antineoplastic, mosquito larvicidal, hemostatic, contraceptive, and deodorant properties. Alum is placed as a potential candidate in the future development of the industry in terms of both healthcare and industrial uses because of its pharmacological aspects, cheapness, safety profile, and ease of acquisition. Alum is used as a gargle to treat mouth ulcers. Halitosis and stomatitis are safe to treat with the help of alum and honey or vinegar or gargling with alum in honey water. Keratitis and conjunctivitis are treated using alum; toothaches are soothed using the powdered alum as tooth powder. Ten grains of alum in powder taken over the tongue will prevent attack of asthma. Powdered alum is used topically to heal infected wounds and bleeding in abrasions and cuts; it is also a stomach and liver tonic, and is used to get rid of nausea and vomiting when taken orally.[29]
Drug Profile of Alum
Chemical Name and Structure
IUPAC Name: Potassium aluminum sulfate dodecahydrate
Molecular Formula: KAl (SO?) ?·12H?O
Molecular Weight: 474.39 g/mol
Chemical Structure: Alum consists of a double sulfate of potassium and aluminum, forming large octahedral crystals when hydrated.
Melting Point: 92°C
Boiling Point: 330°C
Density: 1.757 g/cm³
Appearance: Colorless cubic crystal, mostly octahedral.
Solubility: Soluble in water, and its solubility rate of 5.90 g per 100 ml is at room temperature.
Figure 4: Chemical structure of alum
CHEMICAL COMPOSITION OF ALUM
The alum has the following chemical composition:
• Sulphate range: 38% to 51.06%
• Aluminium: between 9.9% and 28.16%
• Potassium: some of the samples have it up to 14.6%.
• Trace quantity of iron: 0.016% to 0.52%[29]
MECHANISM OF ACTION
Alum is applicable in the treatment of numerous infections, bleeding and also as an antiseptic. It displays the broad spectrum of activities, including its anti-hemorrhagic, antifungal, antibacterial, anti-obesity, antineoplastic, mosquito larvicidal, hemostatic, contraceptive, and deodorant.
It also depicts the antimicrobial, wound sealing, anti-inflammatory, and antibacterial effect in the treatment of oral ulcers.[29]
Hemostatic Action: It induces vasoconstriction, promoting clot formation and reducing bleeding in wounds.
Antimicrobial Properties: Alum exhibits bacteriostatic and fungistatic activity by disrupting bacterial cell membranes and inhibiting microbial growth.[30]
Astringent Effect: Alum works by joining proteins together on mucosal surfaces, which are the moist linings inside parts of your body, like your mouth and nose. This forms a protective barrier. When this barrier is in place, it helps decrease swelling and soothe irritation, making the affected area feel more comfortable.
Anti-inflammatory Effect: It reduces swelling and pain by modulating inflammatory mediators and oxidative stress.[31]
Therapeutic Uses
Wound Healing: Used in topical formulations to aid in clotting and reduce bacterial contamination.
Oral Ulcers: Applied as a gel or powder for aphthous stomatitis and traumatic ulcers.
Hemostatic Agent: Commonly used in minor bleeding conditions such as cuts, nosebleeds, and post-tooth extraction wounds.
Dermatological Applications: Used in deodorants and antiperspirants due to its sweat-reducing effects.
Water Purification: Employed as a coagulant to remove suspended particles from drinking water.[32]
Types Of Alum
There are many types of alum present; some of these types are as follows:
Potassium Alum (KAl (SO?) ?·12H?O): It is the most frequent and common type of alum. This is mainly applied in medicine, cosmetics, and industrial purposes. In medicine, it is used in wound healing due to its antiseptic and astringent properties to fight against oral ulcers. In cosmetics, potassium alum is mainly used in deodorants to inhibit bacterial growth and consequently decrease the occurrence of body odour.
Ammonium Alum (NH?Al (SO?) ?·12H?O): Chemically, this type of alum is potassium alum but with ammonium ions. One of the common industrial applications is water treatment, and textiles use it as well. Ammonium alum is a coagulant used in water treatment to precipitate suspended particles from water, thus clarifying the water and making it safer. In addition, often applied in the paper industry for the quality and durability of paper.
Sodium Alum (NaAl (SO?) ?·12H?O): The food Additive Form of alum is used in the food industry mostly. Leavener for baking powders, a component in the proper rising of baked goods. Apart from its utility in food processing, sodium alum is also employed as a dyeing and tanning agent for leather where it enables the fixing of dyes to fabrics and stabilizes leather.
Ferric Alum (FeAl (SO?) ?·12H?O): Ferric alum is especially that iron is there in its composition than rest alums. Used in industrial water treatment, it is commonly used in municipal water purification plants. Ferric alum is used as a coagulant, where it works with the impurities in water to help remove those impurities. It is also used in papermaking to increase the strength and quality of paper at the manufacturing.
Chrome Alum (KCr (SO?) ?·12H?O): The type of alum that the used is chromium, which is mostly used for the tanning leather industry. Chrome alum is a thickening agent for the collagen fibers in animal hides, giving them greater strength and resistance to water. It is moreover used in photography, i.e, to harden the photographic gelatin and preparations of certain special dyes, pigments, etc.
Selenate Alum (MAl (SeO?) ?·12H?O): This rare form of alum has selenium in the place of sulfate. This form has a definite industrial applicability to chemical manufacturing. Selenate alum, being a mixed composition, is used mostly in research and experimental studies rather than production on an industrial scale.
TURMERIC:
Turmeric is a perennial herb that has rhizomes. It comes from India and is grown a lot in the tropical and subtropical parts of South and Southeast Asia. Turmeric has been used as a home remedy for many illnesses for a long time. It is also a part of many folk remedies and traditional medical systems like Ayurveda. These compounds give it its yellow colour and medicinal properties, and they have different biological and pharmacological effects. These compounds are what give it its yellow colour and medicinal properties. They show a lot of different biological activities and pharmacological effects. The crop improvement programs have mostly been about clonal selection and induced mutation, which are ways to find genotypes that produce a lot of crops and have a high curing rate.[33]

Figure 5: Turmeric
CHEMICAL COMPOSITION OF TURMERIC:
There are many different compounds in turmeric. Eugenol, curcumin, curcumenol, demethoxycurcumin, curcumol, and bisdemethoxycurcumin are some of these. Turmeric contains sesquiterpenes, including curcumenone, dehydrocurdione, and (4 S, 5 S)-germacrone 4,5-epoxide. Turmeric contains an extremely potent compound called cyclocurcumin.[34]
TRADITIONAL USES OF TURMERIC:
Turmeric is also known as Curcuma longa, a perennial herb in the Zingiberaceae family. It is administered as an antibacterial and wound-healing agent for digestive problems, liver detoxification, and respiratory conditions. Utilised in herbal remedies to balance the doshas of Pitta, Kapha, and Vata. Considered a "warming" plant, it encourages blood flow. It is also used to treat discomfort, irregular menstruation, and inflammation of the joints. When combined with other herbs, it is known to have cleansing and anti-inflammatory effects that promote intestinal and liver health. applied as a paste to skin disorders and wounds. Utilised in decoctions for the respiratory and gastrointestinal systems.[35]
Phytochemistry of turmeric:
Turmeric is known for its bright yellow colour and many medicinal properties. Its chemistry is complicated because it has many phytoconstituents. Turmeric also has important minerals and bioactive chemicals in addition to the ones already mentioned:
The makeup of the food:
Protein: Turmeric is good for you because it has 6.3% protein.
Fat: Turmeric has 5.1% fat, which is a good source of important fatty acids.
Minerals: About 3.5% of turmeric is made up of minerals.
Carbohydrates: Turmeric has a lot of carbohydrates, about 69.4% of which are carbohydrates.
Moisture: Turmeric's 13.1% moisture content affects how it feels and how stable it is.[36]
Mechanism of action:
Anti-Inflammatory activity:
The inflammatory process involves leukocytes, also referred to as inflammatory cells, which include neutrophils, lymphocytes, and macrophages. Following the inflammatory cascade, leukocytes release a variety of chemicals, such as cytokines, acute-phase proteins, vasoactive peptides and amines, and eicosanoids. Curcumin is a drug that is commonly used in Eastern medicine and has demonstrated promise in the treatment of various chronic illnesses and inflammatory conditions, including many airborne diseases. Curcumin reduces hydrogen peroxide-induced damage to yellow keratinocytes and fibroblasts, which speeds up the healing process of wounds.[37]
Anti-oxidant activity:
The antioxidant activity of the turmeric samples was measured in terms of the DPPH radical-scavenging activity and FRAP.[38] Curcumin is one of the potent free radical scavengers of oxygen. Like vitamins C and E, it has antioxidant qualities. It is capable of averting the oxidation of lipids or haemoglobin. It can significantly decrease H2O2, superoxide anions, and nitrite radicals production by activated macrophages. Two of its derivatives such as bisdemethoxycurcumin and dimethoxycurcumin are also antioxidants. Curcumin pre-treatment has been shown to lessen ischemia-induced cardiac changes and oxidative stress.[39]
Anti-Microbial activity:
There has been considerable studies on the antibacterial properties of plants across the globe and a few of them have been used as therapeutic alternatives because of the antimicrobial properties.[40]
Alum Turmeric combination therapy:
Alum and turmeric proved better, and are interesting subjects of future research and development. An appropriate concentration of potassium aluminium sulphate (Vickers Laboratories, Ltd., England) was resoluted in sterile distilled water (w/v). Different concentrations of extracts (ETE and ATE) were mixed with alum in a 1:1 ratio to prepare final concentrations of 100, 200 and 300mg/ ml, respectively.[41]
NOVEL HERBAL FORMULATION:
Herbal formulations are dosage forms that have the advantage of providing nutritional, cosmetic and other benefits where a specific amount of one or more herbs or processed herbs are included. Herbal medicines are made through whole, broken or chopped plants that are processed by the use of extraction, distillation, expression, fractionation, purification, concentration or fermentation. Among the innovative drug delivery methods researchers are developing is mouth-dissolving pills, sustained and extended-release preparations, mucoadhesive systems, transdermal preparations, microparticles, microcapsules, nanoparticles, and implants among others due to their potential. Although some of them have reached the market, a few are at the laboratory. When nanotechnology is compared to the conventional methods of preparing plant ingredients, it is clear that there are numerous benefits and it is a potential new method of delivery of medications. some of the benefits include increased permeability, bioavailability, therapeutic efficacy, stability, increased tissue distribution and increased residence.[42] A novel formulation of herbal paste containing turmeric, tulsi, and honey showed promising results in the treatment of oral infections and disorders as well as relieving symptoms in the patients. This herbal paste can be useful to those patients who seek less invasive approaches to more aggressive treatment. Herbal constituents of the formulation have been used over the years in traditional medicine because they may have immunomodulatory, analgesic, anti-inflammatory, and antioxidant effects.[43]
The change of traditional adjuvants comprising of alum to nanoformulations is an indicator of innovation and promise of oral formulations. Recent progress in adjuvant development, particularly the development of nano- formulations has potential to improve safety and efficacy.[44]
SAFETY AND TOXOCITY OF ALUM AND TURMERIC:
Turmeric is one such product with high safety profile and history of more than 4000 years of use as culinary spice and as the traditional medicine according to the ancient Ayurvedic medicinal system of India. The yellow-coloured polyphenolic compounds referred to as curcuminoids are what make turmeric have the health benefits it has. Preclinical and clinical studies have investigated curcuminoid products and curcuminoids concerning their safety and efficacy. Curcuminoids in preclinical safety studies were reported as being non clastogenic and non mutagenic and none exhibited reproductive toxicity when administered orally. The yellow-coloured polyphenolic compounds referred to as curcuminoids are what make turmeric have the health benefits it has. Preclinical and clinical studies have investigated curcuminoid products and curcuminoids concerning their safety and efficacy. Curcuminoids as preclinical safety agents have been reported to be non-clastogenic, non-mutagenic, and have no reproductive toxicity after oral intake.[45] The extracts of Turmeric rhizome, Alum and their combinations/cocktails inhibit the test microorganisms (bacteria and fungi). The low acidity or adverse impact on bacterial/fungal cell wall has been cited to be the cause of the activity of alum and could also explain the current outcomes. The interaction (between Turmeric extracts and Alum) affected more the Gram-negative bacteria than the Gram-positive bacteria likely because activities of bacteria differ and this could be an indication of differences in cell wall structure and composition. Alum and coal rhizomes extracts, and mixtures of crude Turmeric rhizomes extracts were inhibitory against test bacterial and fungal species and represented a broad spectrum of activity. Alum added to Turmeric extracts increased bioefficacy and this new method of research using safe and natural products would offer an alternative to antibiotic and antifungal treatment. Alum when used alone and in complex with nontoxic natural products indicates a rational preventive/therapeutic method of overcoming bacterial and fungal pathogens in plants, animals and people.[41]
FUTURE PROSPECTIVE:
The fact that nano-loaded polymeric systems have steadily increased in the last few years has brought revelations in knowledge regarding wound skin regeneration. These drug carriers enhance skin retention, reduce duration of drug release and prevent drug damage and enhance therapeutic value of biopolymers and synthetic polymers. It is possible that the clinical trials will prompt professionals to do more studies in regards to formulating curcumin-based formulations. Also, the industrial need to produce cheaper, scaled up nanoencapsulation methods of curcumin to reduce the cost of production and enhance competition with other medications. Therefore, it can be concluded that nanoformulations of curcumin can be useful in the future in the context of numerous bioproducts, but further studies are needed, with the wound healing being primary to give scientists more knowledge. All in all, more research needs to be done in order to ascertain the clinical efficacy of curcumin-based formulations to bring the technology into the laboratory into the bedside.[46]
Besides the nanoformulations, there have been other studies that have clarified various innovative formulations of curcumin that are geared towards improving its bioavailability and therapeutic effects in treating various diseases.
Galactomannan Biopolymer Formulation: the application of natural fiber, namely galactomannan biopolymer of Trigonella foenum-graecum (fenugreek) to improve the pharmacokinetics and efficacy of curcuminoids.
Phytosomal Curcumin: Phytosomes are plant metabolites whose chemistry is complex. Amphipathic molecules in phytosomes allow the molecules to be absorbed well in the gut and thus, they are not degraded easily. Curcerin is phytosomal curcumin that is commercially available with phosphatidylserine, phosphatidylcholine and piperine.
Colloidal Submicron Particles and amorphous Formulation (Theracurmin® and CurcuRougeTM): Theracurmin is a commercial bioavailable curcumin which has now become of interest due to its improved bioavailability and therapeutic capability. Theracurmin is an aqueous dispersible agent, which has enhanced absorption and tissue penetration ability, and is a new method of addressing complications that come with curcumin therapeutics. Comparisons of absorption efficiency of Theracurmin in relation to other curcumin drug delivery systems (DDS) preparations revealed that Theracurmin had much higher absorption efficiency, large plasma curcumin concentration and large area under the product concentration-time curve than the others in the DDS.[47] Future design has two strategies that can be utilized to capitalise on nano alum. First, nano alum can be used to use more binding sites of MPLA to form a complex adjuvant, e.g., AS04 (TLR4 agonist MPLA is absorbed on aluminum microparticles). This is a self-evident measure to enhance the functioning of the existing adjuvant system. Secondly, an adjuvant that is very efficient is needed to address the stealth aspect of tumor-specific antigen and self-antigen identification in creation of anti-tumor therapy. The use of conventional alum adjuvant in the development of anti-tumor vaccine is not appropriate because it fails to stimulate strong cellular immunity response that would be required in destroying tumor cells.[48]
CONCLUSION
Curcumin is a broad-spectrum antibacterial agent to numerous bacteria. One of the most promising antibacterial discoveries is the use of curcumin with or without other already existing antibiotics in treating H. pylori and M. tuberculosis. Based on the in vivo and in vitro research, it is possible to conclude that curcumin turned out to be a broad-spectrum antimicrobial drug, which in addition to other antibiotics had an additive effect when introduced as adjuvant treatment. Nevertheless, clinical studies on the antimicrobial activity of curcumin were not conducted aimed at its possible application as an antibiotic in the clinical practice. Small doses of curcumin have a therapeutic potential, with other results indicating that it may be cytotoxic. In addition to its low bioavailability, toxicity, and low solubility, curcumin usually presents numerous issues when given orally or intravenously due to the complexity of the human body. Other experiments have indicated that curcumin is cytotoxic with a certain dose. Alum-based products have really started to stand out as a promising type of natural product for healing wounds and also soothing sore mouth ulcers. It has astringent qualities, and this helps seal wounds with a protective shield, which can reduce leakage of fluids and speed up healing. Benefits like stopping bleeding and fighting infections, make this something great at dealing with little cuts and sores and fighting off bacteria too. Additionally, its anti-inflammatory action aids in reducing pain and swelling, making it an effective remedy for oral ulcers. Though alum-based products have been widely used for centuries, recent research supports the idea of their therapeutic potential. The advantages of the alum gel application and the availability of this product, along with its low cost, make it a better alternative in the treatment. Still, extensive clinical trials and standardized prescriptions need to be conducted to enhance its usage and confirm its maximum efficacy and safety. It is necessary to be careful when using alum, although it has its advantages because overdosing and long-term use can irritate and, in some cases, even cause toxicity. It is necessary to follow certain instructions and take a given amount to avoid suffering from adverse effects. In conclusion, aluminium and turmeric are used as a way out to low cost and at the same time efficient wound healing and oral ulcer management. Future developments and clinical trials will help to expand the usage, making it an important and safe method of healthcare in modern times.
REFERENCES


Vishwajeet Singh, Lokesh Suryawanshi, Abhilasha Yadav, Therapeutic Potential of Alum and Turmeric in Oral Ulcer Management: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4435--4451. https://doi.org/10.5281/zenodo.18797210
 10.5281/zenodo.18797210
10.5281/zenodo.18797210
