Dr. C.S.N Institute of Pharmacy, Bhimavaram, India
Thalidomide, originally developed in the 1950s as a sedative, gained infamy due to its severe teratogenic effects, causing thousands of congenital malformations worldwide. Despite this historical tragedy, subsequent research has revealed its remarkable immunomodulatory, anti-inflammatory, and anti-angiogenic properties, paving the way for therapeutic repurposing. Modern pharmacological studies demonstrate thalidomide’s efficacy in oncology, particularly multiple myeloma, and in the management of autoimmune and inflammatory disorders, including leprosy, Crohn’s disease, and rheumatoid arthritis. Its mechanism of action involves modulation of cytokine production, inhibition of angiogenesis, and selective targeting of tumor microenvironments, making it a unique bioactive molecule. Preclinical and clinical investigations have established safe dosing regimens while highlighting critical adverse effects such as peripheral neuropathy, thromboembolic events, and teratogenicity, necessitating rigorous monitoring and pregnancy prevention programs. The development of thalidomide analogs and derivatives, including lenalidomide and pomalidomide, has further expanded its therapeutic scope with improved efficacy and reduced toxicity. This review provides a comprehensive analysis of thalidomide’s historical significance, pharmacological insights, preclinical and clinical evidence, safety profile, and modern therapeutic applications, emphasizing the transition from a catastrophic drug to a clinically valuable agent. Understanding the lessons learned from thalidomide’s past, combined with ongoing research into its analogs, offers critical perspectives for drug repurposing, rational pharmacology, and safe clinical translation of bioactive compounds.
Thalidomide, a synthetic glutamic acid derivative, was first introduced in the 1950s as a sedative and antiemetic, primarily prescribed to pregnant women for morning sickness. Its initial widespread use was considered safe until the late 1950s and early 1960s when thousands of children were born with severe congenital malformations, including limb deformities, ear and eye abnormalities, and organ defects [1,2]. This tragic outcome marked one of the most notorious cases in pharmaceutical history, highlighting the critical importance of rigorous preclinical testing and drug safety evaluation.
Despite its catastrophic teratogenic effects, thalidomide possesses remarkable immunomodulatory, anti-inflammatory, and anti-angiogenic properties, which later inspired its repurposing for various therapeutic indications [3,4]. Modern research has demonstrated its efficacy in oncology, especially multiple myeloma, as well as in autoimmune and inflammatory conditions, such as leprosy, Crohn’s disease, and rheumatoid arthritis [5,6].
The purpose of this review is to provide a comprehensive analysis of thalidomide’s journey from a drug disaster to a clinically valuable therapeutic agent. This includes its historical context, pharmacological mechanisms, preclinical and clinical evidence, safety considerations, and the development of analogs and derivatives with improved efficacy and tolerability.
By integrating lessons from its past with modern scientific insights, this review aims to offer a forward-looking perspective on thalidomide and its role in contemporary pharmacotherapy.
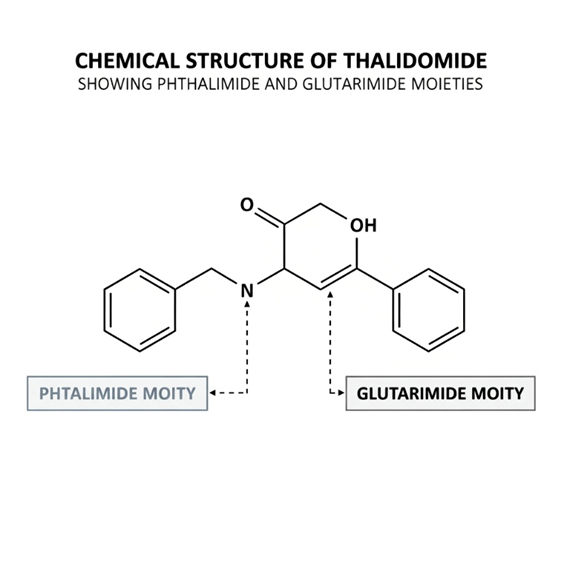
Figure 1. Chemical structure of Thalidomide.
HISTORICAL BACKGROUND AND THE TRAGEDY
Thalidomide was first synthesized in 1953 by Chemie Grünenthal in Germany and marketed in 1957–1958 as a sedative and antiemetic, particularly for alleviating morning sickness in pregnant women [7]. Initially considered safe due to its lack of acute toxicity in adults, thalidomide was widely prescribed across Europe, Canada, Australia, and other regions [8]. However, in 1961, alarming reports emerged of infants born with phocomelia, a severe limb malformation, along with other congenital anomalies affecting the ears, eyes, heart, and internal organs [9,10].
Investigations revealed that thalidomide crosses the placental barrier, disrupting angiogenesis during early fetal development, which leads to malformations [11]. The tragedy prompted global regulatory reforms, including stricter drug testing, teratogenicity studies, and prescription regulations, laying the foundation for modern pharmacovigilance [12,13]. Despite its withdrawal from most markets in the early 1960s, thalidomide’s historical impact remains a seminal lesson in drug safety and ethical responsibility.
The thalidomide episode not only highlighted the catastrophic consequences of insufficient preclinical evaluation but also stimulated research into drug teratogenicity, regulatory frameworks, and public awareness regarding drug use in pregnancy [14]. Its story underscores the critical balance between therapeutic potential and safety, a theme that resonates with modern drug development and repurposing initiatives.
MECHANISM OF ACTION AND PHARMACOLOGICAL INSIGHTS
Thalidomide exhibits a unique pleiotropic pharmacological profile, with mechanisms that underpin its modern therapeutic applications. Its primary actions involve immunomodulation, anti-inflammatory effects, and anti-angiogenesis. Thalidomide modulates the immune system by inhibiting tumor necrosis factor-alpha (TNF-α) production, enhancing T-cell and natural killer (NK) cell activity, and regulating cytokine balance [15,16].
The anti-angiogenic properties of thalidomide are mediated through suppression of vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF) signaling, which reduces neovascularization in tumors and inflamed tissues [17,18]. Additionally, thalidomide interferes with cereblon (CRBN)-dependent ubiquitination, a pathway critical for protein degradation in cells, which is implicated in both teratogenicity and antitumor activity [19,20].
Thalidomide’s pharmacokinetic properties include oral bioavailability, hepatic metabolism primarily via hydrolysis and cytochrome P450 enzymes, and a half-life of 5–7 hours in humans [21]. Its metabolites may contribute to both therapeutic efficacy and toxicity, emphasizing the importance of dose optimization [22].
Modern insights also highlight thalidomide’s selective action on the tumor microenvironment, facilitating apoptosis in malignant plasma cells, while modulating inflammatory and immune responses in autoimmune conditions [23]. These multifaceted mechanisms form the scientific rationale for its use in oncology and immune-mediated disorders, bridging the gap between historical tragedy and contemporary therapeutic triumph.
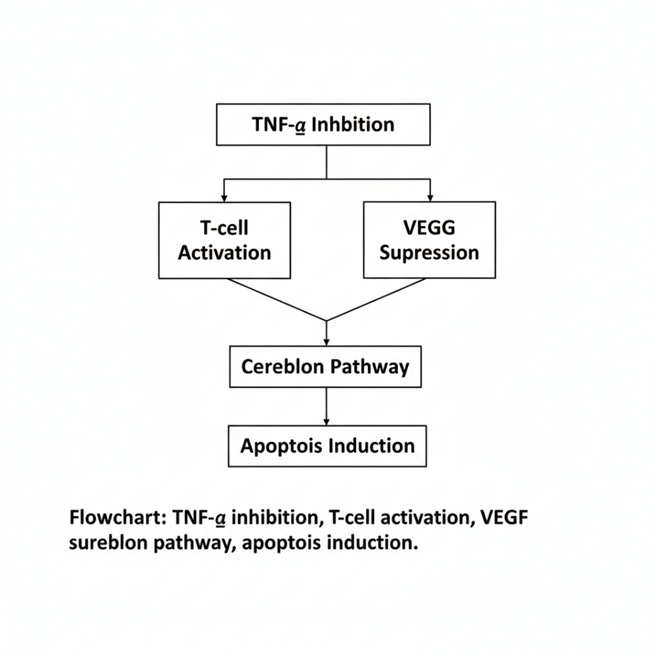
Figure 2. Mechanism of Action of Thalidomide
PRECLINICAL STUDIES OF THALIDOMIDE
Preclinical studies played a crucial role in elucidating thalidomide’s mechanism of action and its potential therapeutic applications beyond its initial sedative use. Early animal studies in rodents and rabbits demonstrated anti-angiogenic effects, showing that thalidomide can inhibit vascular proliferation, which later provided the rationale for its use in cancer therapy [24,25].
In vitro studies highlighted its immunomodulatory properties, such as suppression of tumor necrosis factor-alpha (TNF-α) and modulation of interleukin production, indicating potential for inflammatory and autoimmune conditions [26,27]. Additional investigations demonstrated that thalidomide can induce apoptosis in certain cancer cell lines, particularly hematologic malignancies, while sparing normal cells [28].
Pharmacokinetic studies in animal models confirmed oral bioavailability, hepatic metabolism, and systemic distribution, providing key insights for dose optimization in subsequent clinical trials [29]. Toxicological evaluations revealed the drug’s teratogenic potential, especially during early gestational exposure, and underscored the need for strict pregnancy prevention programs [30].
Preclinical research also examined thalidomide analogs, including lenalidomide and pomalidomide, which were designed to retain immunomodulatory and anti-angiogenic activity while reducing teratogenicity and neurotoxicity [31]. These studies laid the foundation for clinical translation, guiding both therapeutic indications and safety protocols for modern use.
Table 1. Major Preclinical Studies of Thalidomide
|
Study / Author (Year) |
Model / Species |
Dose / Route |
Key Findings / Outcomes |
|
D’Amato RJ et al., 1994 [24] |
Mouse tumor models |
100 mg/kg, oral |
Inhibited angiogenesis, reduced tumor growth |
|
Folkman J et al., 1992 [25] |
Rat corneal angiogenesis |
50–200 mg/kg, oral |
Suppressed neovascularization |
|
Corral LG et al., 1999 [26] |
Human monocyte cultures |
10–100 µM, in vitro |
Inhibited TNF-α production, immunomodulatory effect |
|
Sampaio EP et al., 2001 [27] |
Murine macrophages |
50 µM, in vitro |
Reduced pro-inflammatory cytokine release |
|
Singhal S et al., 1999 [28] |
Myeloma cell lines |
1–10 µM, in vitro |
Induced apoptosis selectively in cancer cells |
|
Schafer PH et al., 1997 [29] |
Rats |
100 mg/kg, oral |
Demonstrated oral bioavailability, systemic distribution |
|
Vargesson N, 2015 [30] |
Rabbit embryo |
10 mg/kg, oral |
Confirmed teratogenic effects during organogenesis |
|
Richardson PG et al., 2002 [31] |
Mouse xenograft models |
50–150 mg/kg, oral |
Thalidomide analogs (lenalidomide/ pomalidomide) showed enhanced anti-tumor activity with lower toxicity |
CLINICAL STUDIES OF THALIDOMIDE
Clinical investigations of thalidomide began after its preclinical immunomodulatory and anti-angiogenic potential became evident. Early trials focused on erythema nodosum leprosum (ENL), an inflammatory complication of leprosy, where thalidomide significantly reduced TNF-α levels, alleviating pain and nodular lesions [32,33]. These studies confirmed its efficacy in autoimmune and inflammatory conditions, laying the groundwork for broader therapeutic applications.
In oncology, thalidomide demonstrated substantial activity in multiple myeloma, particularly in patient’s refractory to standard chemotherapy. Clinical trials reported partial and complete responses, improved progression-free survival, and enhanced patient quality of life [34,35]. Combination regimens with dexamethasone or other chemotherapeutics further increased efficacy, supporting its integration into standard myeloma treatment protocols.
Additional clinical studies explored thalidomide’s potential in Crohn’s disease, rheumatoid arthritis, and graft-versus-host disease (GVHD), where immunomodulatory effects reduced inflammation and improved clinical outcomes [36,37]. The therapeutic window was carefully determined, balancing efficacy with known adverse effects such as peripheral neuropathy, thromboembolic events, and teratogenicity [38].
Recent clinical trials have also evaluated thalidomide analogs, including lenalidomide and pomalidomide, demonstrating improved efficacy and tolerability, expanding the scope of immunomodulatory therapy in oncology and autoimmune disorders [39,40]. Collectively, these clinical studies highlight thalidomide’s transition from a teratogenic drug to a clinically valuable therapeutic agent.
PHARMACOLOGICAL PROPERTIES OF THALIDOMIDE
Thalidomide possesses a multifaceted pharmacological profile, combining immunomodulatory, anti-inflammatory, and anti-angiogenic effects. Its immunomodulatory action primarily involves suppression of tumor necrosis factor-alpha (TNF-α), modulation of interleukins (IL-6, IL-10), and enhancement of T-cell and natural killer (NK) cell activity, which contributes to its efficacy in both autoimmune diseases and malignancies [41,42].
The anti-angiogenic properties of thalidomide are mediated by inhibition of vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF), resulting in reduced neovascularization and tumor growth [43,44]. These effects are particularly relevant in hematologic malignancies like multiple myeloma, where angiogenesis is a critical driver of disease progression.
Thalidomide also exerts anti-inflammatory activity, reducing leukocyte migration and oxidative stress in inflamed tissues, which accounts for its clinical utility in conditions such as erythema nodosum leprosum, Crohn’s disease, and rheumatoid arthritis [45].
Its pharmacokinetic profile includes oral bioavailability, hepatic metabolism via hydrolysis and cytochrome P450 enzymes, and a half-life of 5–7 hours, which informs dosing schedules [46]. Notably, the metabolites of thalidomide contribute to both therapeutic effects and adverse outcomes, emphasizing the importance of careful monitoring [47].
Collectively, thalidomide’s pharmacological properties establish it as a versatile therapeutic agent, with potential applications extending beyond its historical context of teratogenicity to oncology, immunology, and inflammation management.
Table 2. Pharmacological Properties and Molecular Targets
|
Pharmacological Property |
Molecular / Cellular Target |
Key Effects |
|
Immunomodulatory |
TNF-α, IL-6, IL-10, T-cells, NK-cells |
Suppression of pro-inflammatory cytokines, enhanced T-cell and NK-cell activity |
|
Anti-angiogenic |
VEGF, FGF, endothelial cells |
Inhibition of new blood vessel formation, tumor growth suppression |
|
Anti-inflammatory |
Leukocytes, oxidative stress pathways |
Reduced leukocyte migration and tissue inflammation |
|
Apoptotic / Anti-tumor |
Cancer cell lines, caspase pathways |
Induces selective apoptosis in tumor cells |
|
Pharmacokinetic / Metabolism |
Liver (cytochrome P450), systemic circulation |
Oral bioavailability, half-life 5–7 h, metabolite activity |
|
Neurological effects |
Peripheral nerves |
Dose-dependent neuropathy risk |
RESISTANCE, SAFETY, AND TOLERABILITY
While thalidomide demonstrates significant therapeutic potential, its clinical use is limited by adverse effects and safety concerns. The most serious risk is teratogenicity, necessitating stringent pregnancy prevention programs and restricted distribution systems [48,49]. Other notable adverse effects include peripheral neuropathy, sedation, constipation, thromboembolic events, and skin rashes, which require careful monitoring during therapy [50,51].
Thalidomide’s therapeutic window is narrow, emphasizing the importance of dose optimization and individualized treatment regimens. In multiple myeloma, daily doses typically range from 50–200 mg, balancing efficacy with tolerability [52]. Combination therapy with anticoagulants or corticosteroids is sometimes employed to mitigate thromboembolic risk [53].
Resistance to thalidomide, particularly in oncology settings, may occur due to alterations in cereblon-mediated pathways, cytokine signaling, or drug efflux mechanisms, reducing clinical effectiveness over time [54]. The development of thalidomide analogs, such as lenalidomide and pomalidomide, has helped overcome some resistance issues while providing improved safety profiles [55].
Long-term use requires continuous monitoring of hematologic, hepatic, and neurologic parameters, as cumulative toxicity, especially neuropathy, may limit treatment duration. These considerations underscore the importance of vigilant clinical management to maximize therapeutic benefits while minimizing risks.
Table 3. Adverse Effects, Resistance Mechanisms, and Safety Measures
|
Category |
Specific Concern / Mechanism |
Clinical Manifestation |
Management / Safety Measures |
|
Teratogenicity |
Disruption of limb and organ development |
Congenital malformations, phocomelia |
Strict pregnancy prevention programs, contraception, REMS (Risk Evaluation and Mitigation Strategies) |
|
Neuropathy |
Dose-dependent axonal damage |
Peripheral neuropathy, numbness, tingling |
Dose adjustment, neurologic monitoring, limit long-term use |
|
Thromboembolism |
Hypercoagulable state, especially with steroids |
Deep vein thrombosis, pulmonary embolism |
Prophylactic anticoagulation, risk assessment before therapy |
|
Resistance |
Altered cereblon pathways, cytokine signaling, efflux pumps |
Reduced drug efficacy in oncology |
Combination therapy, switch to analogs (lenalidomide/ pomalidomide) |
|
Hematologic / Hepatic |
Cytopenias, liver enzyme elevation |
Anemia, neutropenia, hepatotoxicity |
Regular blood counts, liver function tests, dose modification |
|
Sedation / Gastrointestinal |
CNS depression, constipation |
Fatigue, constipation |
Dose timing, hydration, stool softeners, patient counseling |
THALIDOMIDE AND ITS ANALOGS
To overcome limitations associated with thalidomide, including teratogenicity, neuropathy, and resistance, several analogs and derivatives have been developed. Among the most notable are lenalidomide and pomalidomide, which retain thalidomide’s immunomodulatory and anti-angiogenic properties while exhibiting improved efficacy and reduced toxicity [56,57].
Lenalidomide demonstrates enhanced T-cell and NK-cell activation, superior TNF-α inhibition, and more potent anti-proliferative effects against hematologic malignancies, particularly multiple myeloma [58]. Pomalidomide, a further modified analog, shows even greater potency in refractory cases and maintains a better safety profile, especially regarding peripheral neuropathy [59].
These analogs also exhibit differential binding to cereblon, influencing downstream ubiquitination pathways, which contributes to their enhanced antitumor activity and reduced adverse effects [60]. Ongoing research continues to explore novel analogs and modifications, aiming to optimize pharmacological activity while minimizing toxicity.
The development of thalidomide analogs exemplifies rational drug design and the concept of repurposing and improving historical compounds to meet modern therapeutic needs, bridging the gap between a once-infamous drug and effective, clinically safe agents.
Table 4. Thalidomide Analogs
|
Analog / Derivative |
Structural Modification |
Improved Properties Compared to Thalidomide |
Clinical Applications |
|
Lenalidomide |
Amino group added at 4-position of phthalimide ring |
Enhanced immunomodulatory and anti-tumor activity, reduced neuropathy |
Multiple myeloma, myelodysplastic syndromes, lymphoma |
|
Pomalidomide |
Amino group + hydroxyl modifications |
Greater potency, better safety profile, active in refractory cases |
Relapsed/refractory multiple myeloma |
|
CC-122 (Iberdomide) |
Phthalimide analog with cereblon targeting |
Potent immunomodulation, enhanced T-cell/NK-cell activation |
Hematologic malignancies, under investigation |
|
CC-220 (Avadomide) |
Modified glutarimide ring |
Improved anti-inflammatory and anti-tumor activity |
Lymphoma, autoimmune diseases (clinical trials) |
|
Other experimental derivatives |
Various amino, hydroxy, or imide modifications |
Optimized pharmacokinetics, reduced teratogenicity, selective targeting |
Preclinical studies for cancer and autoimmune conditions |
THALIDOMIDE DERIVATIVES
Beyond the well-known analogs lenalidomide and pomalidomide, a variety of novel thalidomide derivatives have been developed to enhance therapeutic efficacy while minimizing adverse effects. These derivatives include amino-thalidomides, hydroxylated thalidomides, imidodicarbonyl compounds, and other modified glutarimide structures, designed to selectively target inflammatory, neoplastic, and angiogenic pathways [61,62].
Preclinical studies demonstrate that these derivatives retain potent immunomodulatory, anti-inflammatory, and anti-angiogenic effects while exhibiting reduced teratogenicity in animal models [63]. For example, certain hydroxylated derivatives show improved selectivity for tumor cells over normal cells, indicating a better therapeutic index.
These derivatives are being explored in a broad spectrum of indications, including hematologic malignancies, autoimmune disorders, viral infections, and inflammatory conditions, extending the clinical scope beyond what was possible with thalidomide alone [64]. Chemical modifications aim to improve pharmacokinetic properties, such as oral bioavailability, systemic stability, and tissue targeting, while optimizing cereblon binding specificity to enhance antitumor and immunomodulatory effects [65].
The continued development of thalidomide derivatives highlights the potential for rational drug design to transform historically problematic compounds into safe and versatile therapeutics. These advances pave the way for next-generation immunomodulatory and anticancer agents, with ongoing preclinical and early clinical studies exploring optimized molecules that maintain therapeutic benefits while further reducing toxicity.
RESISTANCE DEVELOPMENT, SAFETY, AND TOLERABILITY
Despite its clinical benefits, long-term thalidomide therapy and its analogs are challenged by resistance development and safety concerns, which remain critical considerations for clinicians.
Resistance Development
Resistance to thalidomide, particularly in oncology applications, arises from multiple mechanisms. Alterations in cereblon-mediated pathways can reduce the efficacy of immunomodulatory drugs (IMiDs), as cereblon is a key component of the E3 ubiquitin ligase complex responsible for degradation of specific transcription factors in cancer cells [66]. Cancer cells may also adapt through cytokine signaling changes, including upregulation of pro-survival pathways, or by increasing the expression of drug efflux pumps, limiting intracellular drug accumulation [67].
Such resistance can manifest clinically as reduced response rates, shorter remission periods, and diminished anti-tumor activity, particularly in relapsed or refractory multiple myeloma. Strategies to overcome resistance include combination therapy with corticosteroids, proteasome inhibitors, or next-generation IMiDs, as well as switching to more potent analogs like lenalidomide and pomalidomide, which may bypass some resistance mechanisms [66,67].
Safety Considerations
The safety profile of thalidomide requires meticulous attention. The most severe risk is teratogenicity, which can result in limb deformities, organ malformations, and phocomelia if exposure occurs during pregnancy [68,69]. Consequently, strict pregnancy prevention programs, contraception requirements, and risk evaluation and mitigation strategies (REMS) are mandatory.
Other dose-related adverse effects include peripheral neuropathy, sedation, constipation, thromboembolic events, dermatological reactions, and hematologic abnormalities. Peripheral neuropathy is often cumulative and irreversible, making early detection essential through neurological monitoring and patient reporting of symptoms [70,71]. Thromboprophylaxis is recommended when thalidomide is combined with corticosteroids or chemotherapeutic agents due to an increased risk of deep vein thrombosis and pulmonary embolism [71].
Laboratory monitoring is essential, including complete blood counts, liver and renal function tests, and cardiovascular assessments in patients with risk factors. Dosing must be individualized to balance therapeutic efficacy with tolerability, with adjustments made in response to adverse events [70,71].
Improvements with Analogs
The development of thalidomide analogs such as lenalidomide and pomalidomide has partially mitigated safety concerns while maintaining or enhancing efficacy. These analogs demonstrate reduced neuropathy, improved hematologic safety, and greater potency in refractory cases, allowing for longer-term therapy with better tolerability [72].
CONCLUSION
Thalidomide’s history reflects one of the most dramatic transformations in pharmacology—from a widely condemned teratogen to a clinically valuable therapeutic agent. The early tragedy, marked by thousands of congenital malformations, underscored the critical need for rigorous preclinical testing, pharmacovigilance, and ethical oversight, shaping modern drug development and regulatory frameworks worldwide [73,74].
Today, thalidomide’s immunomodulatory, anti-angiogenic, anti-inflammatory, and apoptotic properties have been harnessed to treat hematologic malignancies, autoimmune disorders, and infectious complications such as erythema nodosum leprosum [75,76]. The systematic understanding of its molecular mechanisms, particularly cereblon-mediated degradation of transcription factors and modulation of cytokine pathways, has facilitated the design of analogs with improved potency and reduced toxicity, including lenalidomide and pomalidomide [77].
The development of derivatives and analogs exemplifies rational drug design, demonstrating how repurposing and molecular modification can transform a historically harmful compound into a therapeutic success. These advances have also expanded the therapeutic horizon, with ongoing research exploring novel derivatives, combination regimens, and targeted delivery systems that promise to further enhance efficacy and safety.
Moreover, thalidomide’s story serves as a cautionary yet inspiring paradigm, emphasizing the importance of balancing risk and reward, ethics and innovation in drug development. The transition from tragedy to triumph not only highlights the resilience of scientific inquiry but also provides a roadmap for repurposing other compounds with complex risk profiles for clinical benefit [78].
Ultimately, thalidomide stands as a symbol of transformative pharmacology, demonstrating that careful science, innovation, and ethical oversight can convert historical mistakes into lasting therapeutic breakthroughs.
REFERENCES






Lokesh Babu Peddireddy, Maheswari Geddada, Pooja Meka, Revanth Durga Chodipilli, Sheba Khandavalli, Sunil Boddani, Thalidomide: From Tragedy to Therapeutic Triumph, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2648-2659. https://doi.org/10.5281/zenodo.17441719
 10.5281/zenodo.17441719
10.5281/zenodo.17441719
