1 Kashi Institute of Pharmacy, Varanasi, India 221307
2 Dr. MC Saxena College of Pharmacy, Lucknow
Wound is any injury of the body specially skin which will disturb the normal functioning and anatomy of body. The wound healing occurs by hemostasis, inflammation, proliferation and maturation. Due to wound complexity its healing is a therapeutic challenge. There are different types of formulations for wound healing present in the market which include hydrofibers, foam dressing, hydrogel dressing, hydrocolloid dressings, biodegradable patches, alginate dressings and liposomal gels. But they are having various drawback such as drug penetration is poor, toxicity, it is difficult to cover large wound surface area and various solubility problems Recent studies shows that statins (HMG-Co A reductase inhibitor) which are lipid lowering agent has potential to treat wound healing as they can modulate various cell processes such as apoptosis, proliferation and inflammation. The ongoing research indicate that the statins can induce viability, placement, mobilization and differentiation of stem cells in the tissue. Due to this reason, there is increase in the healing effect of statin in different types of tissue injuries like bone fracture, myocardial infraction, chronic wound and vasculature lesions. According to the literature review there were many studies conducted to find out the effect of different stains in wound healing. These all-reported studies conclude the use of statins which is a antihyperlipidemic drug in wound healing.
Skin is the largest organ of human body with an effective surface area of 2m2 and has self-renewable power33. It has crucial role in temperature regulation, defense against microbial and environmental harm as well as work as a sensory organ24. The three layers of the skin are epidermis which is the superficial layer, dermis which is deep layer and hypodermis which is the deepest layer of the skin 19,46. According to some evidence various layers of skin play essential role during wound healing process. Keratinocyte (which is about 95% of epidermis) is derived from basal layer43. In wound healing epidermal response is controlled by keratinocytes which are present in basal layer. Basal cells are continuously divided. New cells are pushed by old cells at the surface of skin when the old cells shed. The dermis which is second layer of the skin have elastic fibres that is responsible for recoiling of skin 8,14,15.
A wound can be defined as any injury of the body specially skin (epidermis) which disturb the normal functioning and anatomy of body. On the basis of cause of wound formation, it can be closed wound or open wound. On the basis of healing physiology of wound it can be acute wound or chronic wound40,42. Acute wound can be surgical wound (excisions, incisions) or accidental wound (thermal injuries, electrical injuries, burn wounds). Due to local infection and slow progression stage, it takes long time for chronic wound to recover. The common etiologies for chronic wound are diabetes mellitus, autoimmune diseases, trauma, hypoxia, lack of proper care at the earlier stage of wound. There is increased risk of complication like amputation and infection in case of diabetic wound. The infection and impaired in glucose metabolism are the factors for delayed wound healing in diabetic patients9,4,23. The wound infection is due to growth of some bacteria such as p. aeruginosa, s. aureus and some fungi such as candida albicans, Malesezzia restricta and candida parapsilosis48.
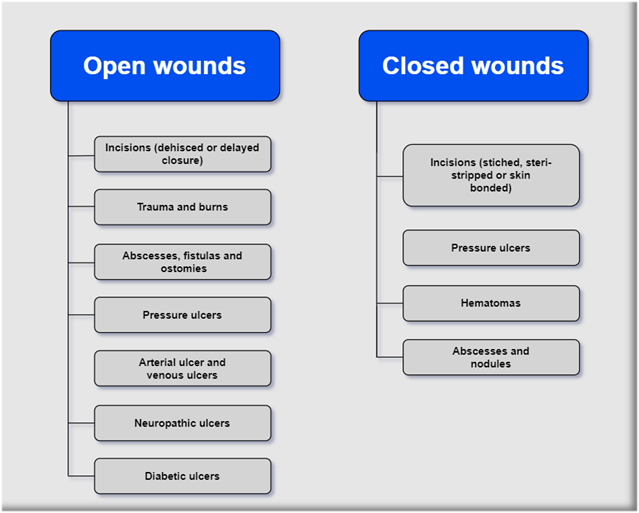
Figure 1. Types of wounds
The four stages of wound healing are haemostasis, inflammation, proliferation and maturation. Haemostasis is the first stage and it involves vasoconstriction; formation of platelet plugs and platelet plug surrounded by fibrin clot. The growth factors and cytokines which also participate in wound healing are secreted by platelets during this stage12,42,20,44,11.
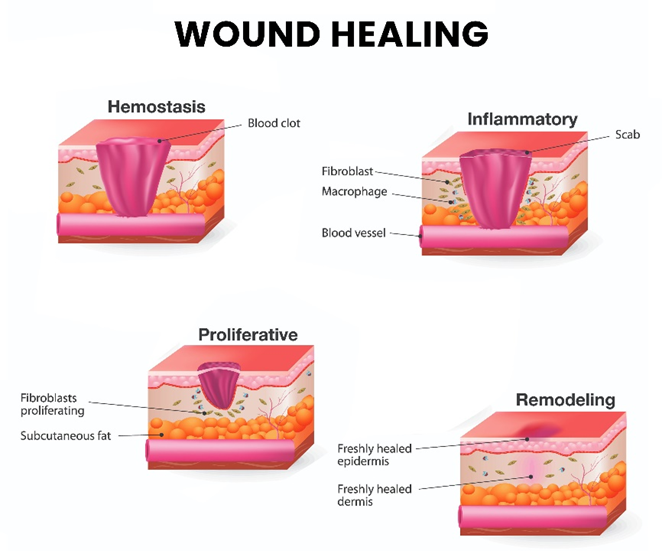
Figure 2. Stages of wound healing
The second stage is inflammation stage in which local inflammation occurs and there is leakage of their content. It last for about 24-48 hours and may extend to one week. The bleeding is controlled, prevented from bacterial infection and the cell debris are removed from wound. This stage provides various growth factor which stimulate angiogenesis and fibroplasia. This stage releases various kind of growth factors as well as eliminate bacteria and the damaged tissues by phagocytosis. The third stage is proliferation stage in which tissue granulation and from pre-existing vessels formation of new blood vessels occur. It starts from day two after injury last up to twenty days depending on the size in acute wounds. The fibroblasts and keratinocytes produce growth factor -β which will lead to myofibroblasts differentiation and tissue formation granulation. The final stage is maturation stage which is also called remodelling phase. In this process wound closure followed by formation of scar occur. It last from twenty-one day to a year after the injury. The wound closure and scar formation occur due to substitution of collagen type III with type I in process48,21.
To restore the normal functioning and structure of the tissue is the aim of wound healing which takes place in haemostasis, inflammation, maturation and proliferation and tissue remodelling. In the stages of haemostasis as well as inflammation human body acts to stop the bleeding. It also tries to initiate the inflammatory response for promoting wound healing. There is release of proinflammatory cytokines, growth factors and reactive oxygen species2,38.
Due to wound complexity its healing is a therapeutic challenge18 ,39. Different kind of wound cause serious physiological trauma and bring economic as well as social burden to the patient. The pathogen such as bacteria, virus and fungus can cause infection at the wound site which can lead to delayed wound healing and inflammation. Because of susceptibility to infection the use of bandages and gauze are limited. The impaired immune response slow down wound healing process. The excess inflammation can cause tissue damage and can slow down the healing process. The deficiency in protein, vitamins and minerals can lead to inability to repair tissues. People with older age are having weak immune system which can delay in wound healing. Some medicines like corticosteroids can delay the wound healing. If there is dry wound then it will cause cell death and too much moisture level is an environment for bacterial growth. The presence of foreign bodies in the wound can stimulate immune response causing inflammation which will hinder the healing process26,27.
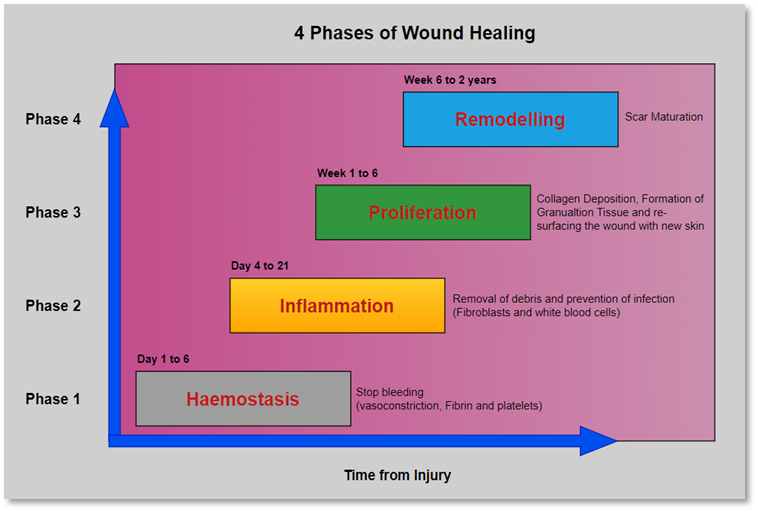
Figure 3. The four phases of wound healing
Epithelialization and angiogenesis impair chronic wound environment which cause delayed healing45. Wounds related to cancer and diabetes create greater challenge for managing and treating because of molecular complexity25.
There are different types of formulations for wound healing present in the market which include hydrofibers, foam dressing, hydrogel dressing, hydrocolloid dressings, biodegradable patches, alginate dressings and liposomal gels. But they are having various drawback such as drug penetration is poor, toxicity, it is difficult to cover large wound surface area and various solubility problems5, 29,32. For accelerated wound healing many antimicrobial agents have been used since ancient times. These include doxycycline, deferoxamine, mupirocin, retapamulin, bacitracin, neomycin, gentamycin and polymyxin B. These antibiotics when delivered locally can deliver a very high concentration of drug to the desired site31. Apart from drugs many metals such silver has been proven as a great antimicrobial and employed for wound healing dressing. Ionized silver (antibacterial agent) is capable of attacking the three bacterial cell component which is cytoplasmic organelles, DNA and cell membrane. Iodine is a natural, non-metallic element which has antimicrobial property. It denatures protein, causes structure change in DNA. Iodine used in low concentration improves the healing rate10. Recent studies shows that statins (HMG-Co A reductase inhibitor) which are lipid lowering agent has potential to treat wound healing as they can modulate various cell processes such as apoptosis, proliferation and inflammation28.
The ongoing research indicate that the statins can induce viability, placement, mobilization and differentiation of stem cells in the tissue. Due to this reason, there is increase in the healing effect of statin in different types of tissue injuries like bone fracture, myocardial infraction, chronic wound and vasculature lesions. Stem cells are responsible for treating the mechanism of abnormal healing in diabetic wound. These cells support the secretion of growth factor and chemokine in injured tissues by improving angiogenesis and extracellular matrix rearrangement, hence a proper environment for wound healing is developed. During different wound healing phases mesenchymal type of stem cells has been found in tissues and their use for the treatment of diabetic wound is due to high proliferation, differentiation capacity and easily production30.
Pleiotropic effects of statins are Anti-inflammatory effect, Antioxidant, decrease oxidative stress, Stabilization of atherosclerotic plaque, diminish blood viscosity and thrombin generation, inhibit proliferation and migration of vascular smooth muscle cells, Improve endothelial function, Immunomodulatory effect, Antiapoptotic features, Antithrombotic effect, antimicrobial effect22.
The statins have shown potential for treatment ranging from inflammatory disease, chronic wounds and bone fracture. The statins also block the synthesis of cortisol and farnesyl pyrophosphate. Both of them inhibit epithelization by acting on glucocorticoid receptors. The pleiotropic effect of statins is related to binding to some nuclear hormone receptor and reduced isoprenylation of mevalonate pathway. Statin exert anti-inflammatory effect as well as they have potential to heal chronic type of wounds due to reduction of farnesyl pyrophosphate (FPP), promote neovascularization, reduce bacterial load and facilitate vascular relaxation. Statins reduce IL-1, IL-6, IL-α and they increase the level of anti-inflammatory mediators IL-10, IL-12. They also control the metabolism of bone17.
Proinflammatory cytokines such as IL-1, IL-6, IL-8 and TNF-α are upregulated after barrier disruption. IL-1 and TNF-α from disrupted endothelial cells and keratinocytes are released immediately. Approximately after 24-hour IL-6 and IL-8 reach to their optimum peak and attract neutrophils. The wound healing proinflammatory phase can be distinguished by release of IL-1. However, there can be detrimental effect on wound healing due to excess of inflammation underscoring spatiotemporal regulation and balance during wound healing process due to these factors. IL-10 inhibits the macrophages toward site of injury and also the infiltration of macrophage. Thus, inflammatory phase is terminated. Extracellular signal is ruled by epithelialization. IL-1 contributes to reepithelialisation through expression of keratin 6/16(k6/k16) to support proliferation and migration in keratinocytes.
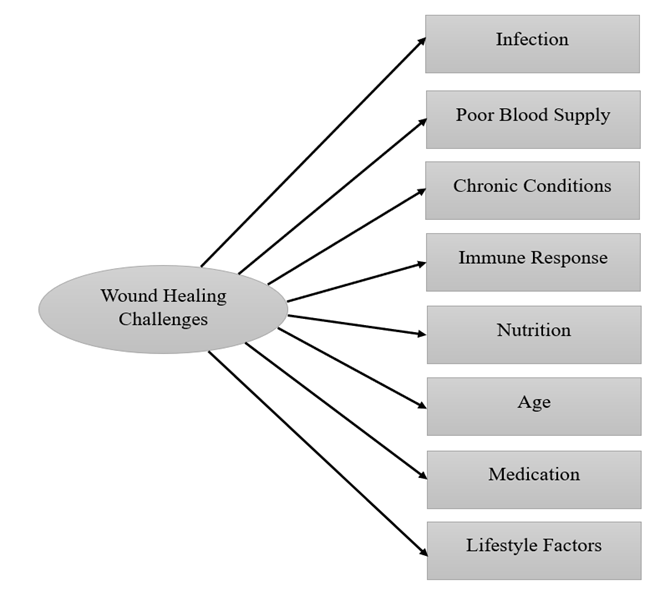
Figure 4. Wound healing challenges
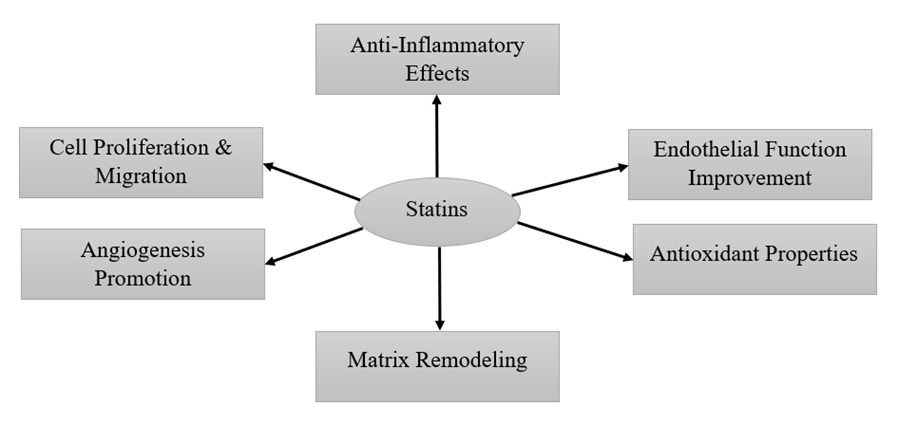
Figure 5. The statins action in wound healing
The IL-1, IL-6, IL-8, TNF-α are upregulated in case of short injury. The anti-inflammatory effect of statins is obtained by reduction of release of chemokines, cytokines, adhesion molecules and C-reactive peptide. By inhibition of Th1- type of chemokine receptors and chemokine release the statins prevent inflammation. The healing time is improved by statins. The process through which statins are involved in wound healing is by regulation of FPP. The FPP is involved in sterol synthesis. For many nuclear receptors which are involved in statins pleiotropic effects FPP may act as ligand. FPP act as anti-inflammatory when it binds to glucocorticoid receptor. The statins which are HMG-CoA reductase inhibitor decrease the formation of mevalonate and downstream farnesyl pyrophosphate. This will induce k6 expression and increased keratinocyte migration and lead to enhanced epithelization. The effect of statin on ischemic wound oxygenation and on perfusion is in such a way that it decreases angiotensin-2, causes vasodilation, causes neovascularization and increase endothelial progenitor cell activity. The anabolic action of statin on bone metabolism is in such a way that bone morphogenic protein is increased and decreased osteoblast apoptosis53.
Simvastatin has shown the repairing of tissue by promotion of neovascularization, increase in proliferation, survival, endothelial precursor cell mobilization through the bone marrow. Simvastatin has antiapoptotic effect so it promotes limphangiogenesis especially favourable for those patients who have defective microcirculation like in diabetic patients, The lovastatin increases the effect of skin blood flow and eNOS (endothelial nitric oxide synthase) in and around the wound skin, so it is capable to increase wound healing. Atorvastatin inhibits the proinflammatory cytokines and reduces the inflammation. The TNF- alpha, IL-6, IL-6 are the proinflammatory cytokines which promote inflammation in response to any kind of injury. The new blood vessels formation is increased by atorvastatin due to increase in expression of vascular endothelial growth factor which is a protein and it stimulate the new blood vessel formation. Atorvastatin helps in improving endothelial function. The functions include prevent the formation of platelet clot, blood flow, facilitate tissue repair and wound healing. Atorvastatin helps in collagen synthesis which helps in the closure of the wound and it also support tissue growth. It helps in restoring the damaged tissue function. Atorvastatin helps in migration and proliferation which helps in tissue generation, new blood vessel formation and re-epithelialization. Statins such as mevastatin, pravastatin have the same effect on wound healing50.
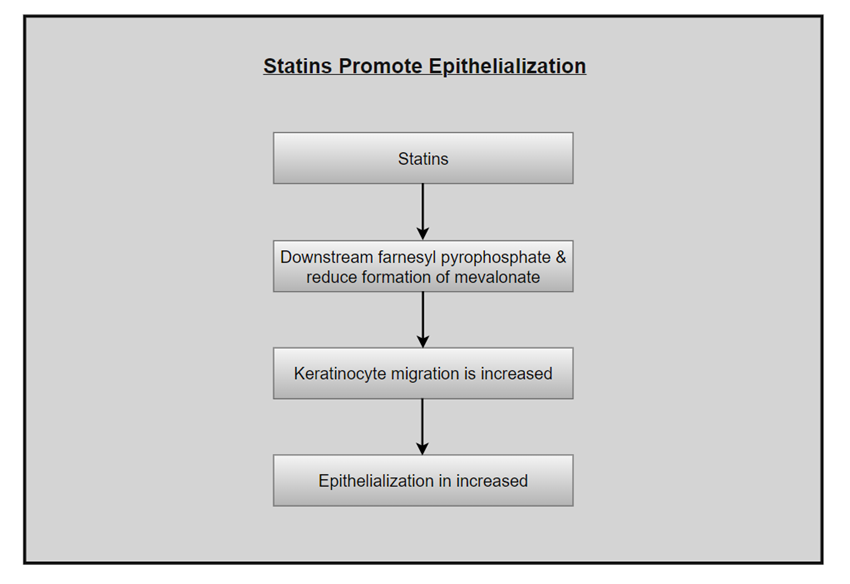
Figure 6. Statins promote epithelialization
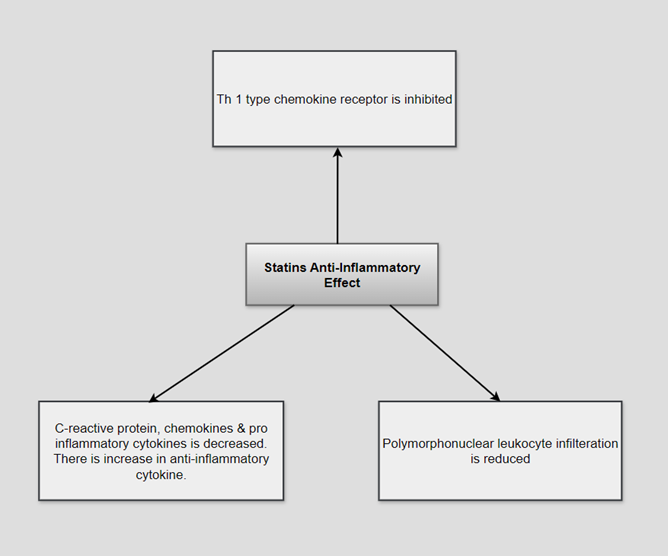
Figure 7. Statins anti-inflammatory effect
Table 1. Effect of Statins on wound healing51
|
Statin |
Topical effect |
Systemic effect |
|
Atorvastatin |
Wound healing rate faster, adhesion formation is small |
Wound healing rate is faster and epithealization, scar area is small, reduced migration of neutrophil, wound breaking strength is increased. |
|
Simvastatin |
Low neutrophil infiltration, low expression of TNF-α and IL-1β |
Higher nitric oxide level, wound healing rate is faster and epithelization, scar area is small, reduced migration of neutrophil, wound breaking strength is increased |
|
Lovastatin |
Wound breaking strength is high, adhesion formation is reduced |
TNF-α level and neutrophil migration is reduced |
|
Pravastatin |
|
Wound breaking strength is high, neutrophil migration is reduced |
|
Rosuvastatin |
|
Free radical scavenger superoxide |
Table 2. Clinical and animal study on the wound healing effect of statins17
|
Study |
Subject / Number |
Intervention |
Statin therapy duration |
Topical statin effect |
|
Statin wound healing effect animal study Rego et.al. 2007 |
Rat having open infected wound/14 |
0.2ml simvastatin microemulsion treated topically |
3 days |
Bacteriological, histological, immunohistochemical property were improved. |
|
Bitto et.al. 2008 |
Wound which is incision induced in diabetic mouse/150 |
5mg/kg simvastatin which is given daily through intraperitoneal route |
12 days |
Improve VEGF secretion and production, significantly improve wound healing capacity |
|
Schiefelbein et.al. 2008 |
Incision is induced in skin and the subcutaneous tissue/32 |
Simvastatin 40mg/kg once a day given intraperitoneally |
13 days |
Decrease VEGF expression of protein and proliferation process at the time of skin repair. |
|
Karadeniz et.al. 2009 |
Intestinal wound in rat/32 |
10 mg/kg simvastatin gavaged once a day |
7 days |
Increased collagen level and mechanical strength in anastomosis site. |
|
Toker et.al. 2009 |
Diabetic wound in streptozotocin induced diabetic rat/28 |
Topical atorvastatin 5% and 1 % |
14 days |
Wound surface area was improved, higher healing rate was achieved and better histological results were obtained. |
|
Laing et.al. 2010 |
Diabetic rat induced with streptozotocin/62 |
0.4 mg/kg/day gavaged pravastatin |
5 days |
Breaking strength and collagen content was increased, there was an increase in nitric oxide level |
|
Statin wound healing effect clinical study Johansen et.al. 2009 |
Neuropathic foot ulcer in diabetic patient<4 month/13 |
In one of the groups 10mg of atorvastatin and 80 mg of atorvastatin was given to another group |
6 months |
There was a decrease in the c- reactive |
The tissue repair process and wound healing process are intricate which involve different stages such as inflammation, tissue remodelling and granulation. Atorvastatin potential has been identified for wound healing. A study conducted by Morsy et.al. 2019 which was having aim to develop and assess the efficacy of atorvastatin nanoemulgel which was applied topically for wound healing. The formulations prepared were atorvastatin gel, atorvastatin nanoemulgel and atorvastatin emulgel and they were evaluated for physical appearance, in vitro drug release, rheological properties and ex vivo permeation of the drug. The in vivo activity was performed on rats. The skin permeation potential of atorvastatin was (p<0.05) increased when it was formulated into nanoemulgel. The greater potential of wound contraction was obtained with nanoemulgel in the in vivo studies. The improvement was observed after 21 days of the treatment with atorvastatin nanoemulgel which was shown in skin histological architecture. All data represent the potential for atorvastatin nanoemulgel for the treatment of wound healing. The wound closure was completed followed by epithelialization within twenty-one days28.
Aly et.al. 2019 prepared polymeric nanoparticle of simvastatin using innovative stabilization technique. It was found that simvastatin was promoting the process of wound healing. The formulation was stabilized with the help of glycerol which was then coated with simvastatin nanoparticles, so their wettability was enhanced. This modification was helping in easy incorporation of particles into the polymers. It was observed that the solubility of simvastatin was increased up to 23.4-fold in glycerol-based formulation. There was an improvement in wound healing capacity of the prepared formulation. The study showed the potential of simvastatin nanoparticle in treatment of wound healing16.
Zaki et.al. 2022 conducted a study which was focusing on formulation and statistical optimization of transethosomes formulation of rosuvastatin to increase its effectiveness in case of topical wound healing. The design expert software was used. The variables taken were was surfactant concentration (% w/v), surfactant type (either tween 80 of span 60) and ethanol concentration (%w/v) The entrapment efficiency percentage, zeta potential and vesicle size were the dependent responses. With the help of expert software, the numerical optimization was conducted. The design expert software optimized the formula comprising of 0.819439 (% w/v), span 60, 40 (%w/v) ethanol ,100 mg lecithin. The desirable score achieved was 0.745 with the values predicted for entrapment efficiency % at 66.5517, zeta potential at -33 and vesicle size at 277.703. There were less than 5% deviations from the predicted value. The formula which was optimal were taken for characterization including differential scanning calorimetry, x-ray diffraction, TEM in vitro release studies, aging effects, and wound healing efficiency. The rosuvastatin compatibility with its formulation ingredients were confirmed by DSC thermogram. The XRD results were showing that the rosuvastatin encapsulation was within the vesicles of transethosomes. The TEM results showed that the nanovesicles were spherical in nature, with no aggregation sign. The optimized formula showed that the drug release was increased as compared to the drug suspension and over the one month it showed good stability. The wound healing efficacy was superior as compared to standard silver sulphadiazine (1% w/w) gel loaded with drug. There was improvement because of enhanced nanosized vesicles penetration in the skin, which help in wound healing process. So, this formulation of rosuvastatin can be considered as a promising carrier for wound healing49.
Rizg et.al. 2022 formulated a self-nanoemulsifying system based on geranium oil and loaded the drug pravastatin in it. The geranium oil and pravastatin showed anti-inflammatory and antibacterial properties. The formulation was developed and evaluated for their effect on the burn wound diameter in experimental animal and for their droplet size. The formulation was also tested for its ex-vivo permeation study, antimicrobial efficacy, wound healing capabilities. The droplet size obtained was from 61nm to 138nm. The synergistic effect was obtained to promote burn wound healing from both geranium oil and pravastatin. It showed enhanced wound closure, anti-inflammatory and antimicrobial properties. There was fourfold reduction in burn wound diameter, a 3.81-fold decrease in interleukin-6 serum levels compared to the negative control, a fourfold increase in the inhibition zone against Staphylococcus aureus compared to the nano emulsion with geranium oil, and a 7.6-fold increase in the skin permeation of pravastatin. The created nano emulsion which was containing both geranium oil as well as pravastatin could be considered as promising model for burn wound treatment37.
The study conducted by Bagheri et.al. 2021 in which chitosan–carboxymethyl cellulose was utilized to encapsulate Nigella sativa oil, thus forming oil nanogel. Then atorvastatin was loaded in it to form oil nanogel. In the analysis of particle size there was average size of 172nm and 193nm of oil nanogel and atorvastatin oil nanogel. The surface charge of oil nanogel and atorvastatin oil nanogel was 32.2 Mv and 34.7 Mv. The TEM images were showing that particles were uniformly distributed and were spherical in shape. The release profile, atorvastatin oil nanogel stability, drug loading efficiency demonstrating satisfactory atorvastatin loading and release characteristics. The cytotoxicity test was showing that the atorvastatin oil nanogel can release atorvastatin in fibroblasts safely. The study of in vitro permeation for both oil nanogel as well as atorvastatin oil nanogel were indicating that there was good penetration from different layers of skin. The in vitro wound closure assay confirmed that atorvastatin oil nanogel promoted fibroblast proliferation and migration, highlighting its potential for wound-healing applications. In a fibroblast scratch model, atorvastatin oil nanogel treatment resulted in increased expression of FGF2, TGF-β1, and VEGF genes, which are crucial for fibroblast proliferation and migration, aimed at wound healing (p < .001). The oil nanogel of atorvastatin showed bactericidal activity against S. aureus, S. epidermidis and Staphylococcus. These all findings suggested that oil nanogel and atorvastatin oil nanogel can be a promising carrier in transdermal drug delivery system for skin wound healing6.
Top of FormThe aim of the study conducted by Orgul et.al. 2017 was to develop 3D and biodegradable tissue scaffold which is composed of biological polymer and nanostructured lipid carriers loaded with simvastatin for the treatment of diabetic wound healing. Nanostructured lipid carriers were synthesized through high-shear homogenization, and freeze-drying was utilized for the integration of nanostructured lipid carriers into the tissue scaffolds. The resultant nanostructured lipid carrier suspension was having spherical and nanosized particles ranging from 110-158 nm, The particles were uniformly distributed (PDI<0.16) and the encapsulation efficiency was exceeding up to 99%. The characterization was performed using differential scanning calorimetry and FTIR. The tissue scaffolds exhibited a 3D highly porous architecture (74.38%) with adequately large pore sizes (~100-200 µm), low weight loss (57.7%), high absorption capacity (710.88%), and robust mechanical strength. Incorporation of nanostructured lipid carrier into the tissue scaffolds delayed the initial release of simvastatin, resulting in a more controlled release profile. The biocompatibility of the tissue scaffolds was confirmed via MTT assay. The findings indicate that tissue scaffolds hold potential as effective candidates for the treatment of diabetic wounds30. Top of Form
Masry et.al. 2024 conducted research whose aim was to create biodegradable oleic acid and eco-friendly based ufasomes which was coated with chitosan for rosuvastatin topical delivery for the treatment of diabetic wound healing. The thin film hydration technique was used for the preparation of ufasomes by varying oleic acid concentration, with the most promising formulation being coated with chitosan. There was impact of chitosan and oleic acid concentration on zeta potential, vesicle size, polydispersity index, entrapment efficiency and in vitro drug release was evaluated. The characterization of chitosan coated ufasomes were done by TEM, FTIR, in vitro drug release broth microdilution susceptibility test, storage effect, ex-vivo skin permeability study, and wound healing efficiency in rats. The coated ufasomes were incorporated into the chitosan gel and the wound healing efficiency was evaluated in rat. The uncoated ufasomes sowed the highest entrapment efficiency (79.48%), small vesicle size (149.6nm), zeta potential (-35.78), polydispersity index of 0.18. Coated ufasomes FTIR analysis showed that there was effective chitosan coating as corroborated by TEM imaging. The cumulative percentage of drug permeated across rat skin after 24 hours for coated ufasomal dispersion and coated ufasomal in chitosan gel were 11.21% and 10.48%, respectively, compared to 2.97% for the control gel, as confirmed by flux and permeability coefficient results. CUF 3 in chitosan gel achieved maximum skin retention and a controlled release effect with reduced risk of systemic absorption of rosuvastatin. Rosuvastatin encapsulated in ufasomal vesicles enhanced antimicrobial activity against Gram-negative and Gram-positive bacteria. Morphological and histopathological studies confirmed the remarkable wound healing efficacy of CUF 3 in chitosan gel. Oleic acid-based ufasomes coated with chitosan could serve as a promising eco-friendly carrier for rosuvastatin, providing a triple effect formulation for diabetic wound healing13.
Abootorabi et.al. 2022 conducted research in which there was development of atorvastatin loaded noisome by using ultrasonic method and evaluated its effect on wound healing in an animal model. The formulation optimized was named as atrosome which was stable at four degrees Celsius for three months. Differential Scanning Calorimetry, Attenuated Total Reflectance-Fourier Transform Infrared Spectroscopy, and Powder X-ray Diffraction analysis demonstrated that atorvastatin was effectively encapsulated within the noisome, either in a stabilized amorphous form or a molecularly dispersed state. Scanning Electron Microscopy, Transmission Electron Microscopy, and Atomic Force Microscopy confirmed the spherical shape of the atrosomes. The atrosome spherical shape was confirmed by transmission electron microscopy, scanning electron microscopy and atomic force microscopy. The polydispersity index was found to be 0.457 ± 0.05, particle size of 196.33 ± 6.45 nm, drug encapsulation efficiency of 86.15 ± 0.58%, and a zeta potential of −20.73 ± 0.98 mV. From the atrosome gel atorvastatin was released following first order kinetics. The in vitro studies demonstrated no cytotoxicity with nearly 99% cell viability in a human foreskin fibroblast cell line. The male Wistar rat was selected as excision wound model for assessing the in vivo efficacy of formulation. This was done by examining malondialdehyde, hydroxyproline level, glutathione peroxidase, superoxide dismutase in the sample of skin tissue. The atrosome gel was showing reduction in malondialdehyde levels, while levels of glutathione peroxidase, superoxide dismutase, and hydroxyproline increased after twenty-one days. According to histological analysis the rats which were treated with atrosomes were healing more faster and effectively1.
Recent research by Ahmed et al. (2023) explored simvastatin as a wound healing agent with the potential to surpass current wound therapies. The simvastatin loaded with cubosomes for topical delivery was prepared. Its aim was to increase simvastatin skin permeation so improved wound healing effects will be obtained. The cubosomes were prepared using top-down method and were characterized by different techniques. The most optimal simvastatin cubosomal formulation was incorporated into a cubogel dosage form using different gelling agents. The cubosomes prepared were having average particle size of 113.90 ± 0.58 nm, entrapment efficiency 93.95 ± 0.49%, showed the sustained release of the simvastatin. The rheological behaviour of the optimized simvastatin was pseudoplastic. The formulation increased the drug permeation by passing through excised rat skin when it was compared to free simvastatin hydrogel, which was having flux value of 46.18 ± 2.12 mcg cm−2 h−1 and 25.92 ± 3.45 mcg cm−2 h−1, respectively. In vivo studies on rats confirmed the promising potential of simvastatin cubosomes as a wound healing treatment3.
A study conducted by Rahamathulla et.al. 2024 prepared simvastatin liposomal gel. Its aim was to formulate, evaluate and optimize simvastatin encapsulated liposomal gel for the treatment of wound healing. The formulation was optimized using response surface methodology via the thin-film hydration technique. The influence of formulation variables, including 1,2-dioleoyloxy-3-trimethylammoniumpropane (DOTAP) concentration, span 80 concentration, and cholesterol concentration, on zeta potential, entrapment efficiency (%), and particle size was examined. The optimized formulation of liposome showed a zeta potential value of 16.56 ± 2.51 mV, indicating robust stability and a high simvastatin encapsulation efficiency of 95.6 ± 4.2%. The particle size of 190.3 ± 3.3 nm confirmed its stability and structural integrity. The liposomal gel showed pseudoplastic behaviour which is very important for topical delivery system because of improved spreadability, enhanced penetration, ease of application, leading to prolong simvastatin release. After evaluating the efficacy of wound healing it was found that there was reduction in the wound size in mice by the sixteenth day post-wounding. The result showed that liposomal gel can be a promising delivery strategy for the incorporation of simvastatin34.
In a study conducted by Bitto et.al. 2008 the effect of simvastatin on diabetic wound healing was examined. A wound model which was incised was developed on the back of diabetic mouse(female) as well as their normoglycemic counterparts. The animals were given daily treatment of simvastatin or a vehicle. At various intervals (3, 6 and 12-days post-injury) the mice were sacrificed to measure vascular endothelial growth factor (VEGF) mRNA and protein expression, to histologically evaluate the healing process, and to assess wound breaking strength and angiogenesis via CD31 immunostaining. In case of diabetic mice, the treatment of simvastatin increased the vascular endothelial growth factor mRNA VEGF mRNA (simvastatin = 4.8 ± 0.6 n-fold/β-actin; vehicle = 2.3 ± 0.4 n-fold/β-actin) and protein expression (simvastatin = 5 ± 0.7 integrated intensity; vehicle = 2.2 ± 0.3 integrated intensity) and elevated nitric oxide wound content on day 6. Additionally, the statin improved breaking strength and PECAM-1 immunostaining on day 12 and it restored the impaired wound healing process in diabetic mice. Similar outcomes were observed in normoglycemic mice. Passive immunization with an anti-VEGF antibody (10 µg/mouse) completely negated the beneficial effects of simvastatin on healing in diabetic mice. Simvastatin shows promise for treating diabetes-related wound healing disorders7.
To achieve sustained drug delivery simvastatin chitosan nanoparticle was incorporated into polyvinyl alcohol hydrogel to increase the wound healing efficacy. Yasasvini et.al. 2017 developed the microparticles by using ionic gelation method and varying the composition of surfactant (Tween 80/Pluronic F-127) and chitosan. The formulation was optimized for morphology, entrapment efficiency, drug and polymer interactions. With 0.3% of tween 80 and chitosan to drug ratio was 0.5:5 the microparticles were formulated. The 82% of entrapment efficiency was the highest which was achieved, spherical morphology was found and there was minimum interaction between the chitosan and drug. The 5% of PVA solution was loaded with pure drug or drug-loaded microparticles at three different doses (2.5 mg, 5 mg, and 10 mg equivalents of the drug). They were crosslinked chemically with hydrochloric acid and glutaraldehyde. The optimized hydrogel was for swelling, in vitro release and the efficacy of wound healing. Hydrogels containing a 2.5 mg equivalent dose of Simvastatin microparticles exhibited the highest cumulative drug release of 92% (n = 3) over seven days, supported by a higher swelling index for the low-dose hydrogels. The in vivo wound healing study utilized Wistar rats (n = 30, divided into 5 groups with 6 animals each) to test the formulated hydrogels (at three doses) and compare them with untreated animals and a positive control group treated with conventional 1% Simvastatin ointment. The wound healing effect mirrored the in vitro results, with animals treated with low-dose hydrogels (replaced every 7 days) showing a significant reduction in wound area compared to those treated with medium and high-dose hydrogels. Statistically significant differences (P < 0.05) in wound areas were observed in animals treated with low-dose hydrogels compared to those treated with the 1% ointment and untreated animals, as determined by two-way ANOVA. Histopathological images of the various animal groups further illustrated the comparative changes in the wound healing process. Therefore, the incorporation of Simvastatin-chitosan microparticles into PVA hydrogels has demonstrated substantial wound healing efficiency at an optimal dose47.
Alim et.al. 2020 conducted a study whose objective was to develop evaluate simvastatin loaded elastic provesicular system for the treatment of topical wound healing. The excipients used in the formulation of simvastatin provesicles were span 40, cholesterol and three edge activators (span 80, tween 80, sodium cholate). The vesicles showed that there was high entrapment efficiency of simvastatin which was ranging from 87.25% - 98.15% having vesicle size ranging from 462.3 to 801.5nm. As the size of vesicles were decreasing there was increase in concentration of edge activator. Good stability of the formulation was found with high negative zeta potential. The release profile of simvastatin from the hydrated provesicular carriers exhibited a biphasic nature. There was two-fold increase in simvastatin permeation through the rat skin when compared to the free drug. The wound healing activity of provesicular formulation has shown a decrease in wound size in rats 14 days post wounding. These findings were further corroborated by a notable increase in the expression of vascular endothelial growth factor and collagen type I compared to the free drug. The results were suggesting that the provesicular carriers can be a promising delivery system for simvastatin encapsulation and the effectiveness of enhanced wound healing52.
The study conducted by Rezvanian et.al. 2021 investigated that simvastatin topical application through a hydrogel dressing enhanced as well as regulate the diabetic wound healing by promoting collagen synthesis and angiogenesis. The in-vivo study efficacy was evaluated on type 1 diabetic wound model. Male Wistar rats were taken for the experiments for the period of 21 days. The intraperitoneal injection (streptozotocin, 50mg/kg) were given to the developed diabetes Wistar rats and then randomly assigned various groups. On 7,14 and 21 days of post wounding the rats were euthanized and the tissues of wound were harvested for the purpose of analysis. The healing rate of wound, haematological analysis, histological analysis, Hydroxyproline assay and vascular endothelial growth factor were recorded. The results indicated that the wound dressing significantly (p < 0.05) accelerated wound healing compared to the control after 21 days of treatment, achieving approximately 99% wound closure without any adverse systemic reactions. The histological data were showing that there was enhanced in re-epithelialization as well as collagen deposition. The collagen synthesis rate was increased. The angiogenesis was also increased in those group treated with hydrogel film loaded with simvastatin. So, the study showed that the created film was having the potential for the treatment of diabetic wound healing by fast re-epithelialization, increase in collagen deposition and pro-angiogenic effects36.
Tejaswini et.al. 2020 conducted research whose aim was to create chitosan hydroxyapatite composite bioscaffolds on which atorvastatin was loaded for the treatment of wound healing. The hydroxyapatite was made from the biowaste of eggshell, calcium chloride crosslinked and atorvastatin was loaded. The sample was characterized for physicomechanical property, DSC, morphological assay and the invitro drug release. Agar diffusion method was used assessing antibacterial activity and the in vivo evaluation of performed by using an excised model of wound healing. The results were showing that there was optimal physicomechanical property which included swelling behaviour (68%), tensile strength (0.0283 MPa), thickness (60µm) and burst time (1.9s). The inhibition zone against Bacillus subtilis was found to be 3.2cm, for staphylococcus aureus was 3.0 cm, E. coli was 3.5cm and Pseudomonas aeruginosa was 2.7 cm. The group which was treated with Hcc3 was observed with complete wound closure, which demonstrated 100% contraction of wound. The study concluded that atorvastatin loaded chitosan hydroxyapatite composite bioscaffolds provide a effective way for the treatment of wound healing41.
CONCLUSION
Statins, traditionally known for their lipid-lowering properties, have demonstrated promising potential in enhancing wound healing through their pleiotropic effects. Their ability to modulate inflammation, promote angiogenesis, improve endothelial function, and stimulate collagen synthesis positions them as valuable adjuncts in the management of chronic and acute wounds. While preclinical and clinical studies provide encouraging evidence, further large-scale, controlled trials are required to establish optimal dosing, formulation, and safety profiles for wound healing applications. The integration of statins into wound care strategies may offer a cost-effective and accessible approach to improve patient outcomes and accelerate tissue repair.
ACKNOWLEDGEMENTS
I would like to express sincere gratitude to amity university, my mentor Dr Poonam Parashar and my supervisor Dr Pragya Yadav for their guidance and support throughout the preparation of this review. Special thanks to colleagues and peers who provided valuable insights and constructive feedback. The contribution of various research studies and literature that formed the basis of this article is also gratefully acknowledged.
REFERENCES


Shivangi Verma, Gulafroz Siddiqui, Statins in Wound Healing, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3296-3315. https://doi.org/10.5281/zenodo.18406449
 10.5281/zenodo.18406449
10.5281/zenodo.18406449
