Department of Pharmacy Practice, Shivlingeshwar College of Pharmacy, Almala, Latur
Stroke is a leading cause of morbidity and mortality worldwide, necessitating timely and effective diagnosis and treatment. Recent advancements in imaging technologies, novel thrombolytic agents, and emerging nanotechnologies have transformed the landscape of stroke care. This comprehensive review aims to provide an overview of the current state-of-the-art techniques for stroke diagnosis and treatment. We discuss the role of diffusion-weighted MRI, novel thrombolytic agents, anticoagulation therapy, and emerging nanotechnologies in improving patient outcomes. Our findings highlight the need for a multidisciplinary approach to optimize stroke care, incorporating cutting-edge imaging technologies, effective thrombolytic agents, and innovative nanotechnologies. This review provides a valuable resource for clinicians, researchers, and healthcare professionals seeking to stay up-to-date with the latest advancements in stroke diagnosis and treatment, ultimately aiming to improve patient outcomes and reduce the global burden of stroke.
Stroke is a cerebrovascular disease, is a condition occurs where blood flow to the brain is disrupted, causing sudden neurological deficits due to either an ischemic stroke or haemorrhagic stroke and that causes lack of oxygen to the brain cell that may leads to brain damage, disability or death [1]. Stroke is a term used to describe an abrupt onset of focal neurologic deficit that lasts at least 24 hours and is presumed to be of vascular origin. Transient ischemic attacks (TIAs) are focal ischemic neurologic deficits lasting less than 24 hours and usually less than 30 minutes [2]. Types of Strokes: There are three primary categories of stroke, each with distinct characteristics:
1. Ischemic Stroke (87% of all cases): This is the most common type of stroke. It occurs when a blood clot forms, blocking blood flow to a specific area of the brain or when oxygen and nutrients are unable to reach the affected brain tissue, leading to damage.
2. Haemorrhagic Stroke: This type of stroke occurs when a blood vessel in the brain ruptures, causing bleeding, the bleeding puts pressure on surrounding brain tissue, leading to damage. Haemorrhagic strokes are often caused by aneurysms (weaknesses in blood vessel walls) or arteriovenous malformations (abnormal connections between blood vessels).
3. Transient Ischemic Attack (TIA) also known as a "Ministroke". A TIA is a temporary disruption in blood flow to the brain, lasting only a short period. During a TIA the blood flow to a part of the brain is inadequate, symptoms appear, but then resolve on their own without treatment, normal blood flow resumes, and the symptoms disappear
Stroke is a potentially life-threatening condition. According to the American Heart Association (AHA), the mortality rate for stroke patients in 2017 was alarming where 37.6 out of every 100,000 people diagnosed with stroke did not survive. However, there is a silver lining. Thanks to significant advancements in medical care and stroke management, the mortality rate has decreased substantially over the years: Between 2007 and 2017, the mortality rate dropped by 13.6%, indicating a notable improvement in stroke treatment and patient outcomes. These statistics highlight the importance of seeking immediate medical attention if stroke symptoms occur, as timely treatment can greatly improve survival rates and outcomes [3].
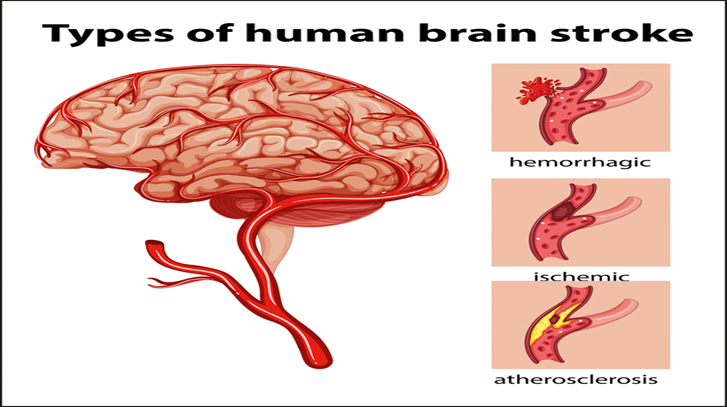
Figure.1: Stroke types
As World Health Organisation (WHO) reveals very year, 15 million people around the world experience a stroke. Sadly, 5 million of these people will die, and another 5 million will be left with permanent disabilities. This not only affects the individuals but also puts a huge burden on their families and communities. Strokes are relatively rare in people under the age of 40. However, when they do occur in younger people, high blood pressure is usually the main cause. Interestingly, children with sickle cell disease are also at risk, with about 8% of them experiencing a stroke. There are several risk factors that increase the likelihood of having a stroke. The two most significant ones are high blood pressure and tobacco use. In fact, if people controlled their blood pressure, four out of every 10 stroke deaths could be prevented. Similarly, smoking is responsible for two-fifths of stroke deaths in people under the age of 65. Other important risk factors include atrial fibrillation (an irregular heartbeat), heart failure, and heart attacks, other includes diabetes mellitus, high cholesterol, smoking, obesity, family history of stroke, age, excessive alcohol consumption, sleep apnoea. Fortunately, many developed countries have seen a decline in the number of strokes in recent years. This is largely due to better management of high blood pressure and reduced smoking rates. However, despite this decline, the total number of strokes is still increasing. This is because the population is aging, and older people are more likely to experience a stroke. Overall, it's essential to be aware of the risks and take steps to prevent strokes from occurring [4].
LITERATURE REVIEW:
Most strokes, about 85%, are called ischemic strokes. This type of stroke happens when the blood flow to the brain is blocked. There are three main reasons why this blockage occurs:
1. Small vessel disease: This is when the tiny blood vessels in the brain become damaged and narrow.
2. Cardio embolism: This is when a blood clot forms in the heart and travels to the brain, causing a blockage.
3. Large artery disease: This is when the bigger blood vessels in the neck and head become damaged and narrow.
However, when younger people have an ischemic stroke, it's often due to different reasons, such as extracranial dissection is when there's a tear in the blood vessels outside the skull. Bleeding in the Brain (Intracerebral Haemorrhage) where about 15% of strokes are caused by bleeding in the brain, known as intracerebral haemorrhage. This type of stroke can occur in different parts of the brain:
1. Deep bleeding: This occurs in the deeper parts of the brain, such as the basal ganglia and brainstem.
2.Cerebellar bleeding: This occurs in the cerebellum, which is the part of the brain that controls coordination and balance.
3. Lobar bleeding: This occurs in the outer parts of the brain, known as the lobes.
The main causes of deep bleeding are high blood pressure which can damage the tiny blood vessels in the brain, leading to bleeding. Small vessel disease: This can also cause bleeding in the deeper parts of the brain. On the other hand, lobar bleeding is often caused by:
- Cerebral amyloid angiopathy: This is a condition where abnormal proteins build up in the blood vessels of the brain.
- Small vessel disease: This can also cause lobar bleeding.
Rare Causes of Bleeding in the Brain is about 20% of intracerebral haemorrhages are caused by less common factors, such as:
- Abnormal blood vessels: This includes conditions like vascular malformations, aneurysms, and cavernomas.
- Blood clots in the sinuses: This is known as venous sinus thrombosis.
- Rare genetic conditions: These can increase the risk of bleeding in the brain [5].
Risk Factor:
Modifiable Risk Factor: Modifiable risk factors are crucial because stroke risk can be decreased by intervention strategies that target these factors. Risk factors must be identified and changed as soon as possible. Medical conditions and behavioural risk factors are two more categories of modifiable risk factors. It is commonly known that a number of conventional risk factors, including smoking, diabetes mellitus, hypertension, and hyperlipidaemia, contribute to stroke. Research is still being conducted to examine new or developing risk factors.
Non-modifiable Risk Factor: There are several indicators of stroke risk, including age, gender, race, ethnicity, and heredity. Despite the fact that these factors are unchangeable, their existence aids in identifying the most vulnerable, allowing for the aggressive management of risk factors that are changeable. The most significant risk factor for stroke is age. The stroke rate more than doubles for both men and women for every ten years after the age of 55. Although men are 1.25 times more likely than women to have a stroke, more women than men lose their lives to stroke each year because women typically outlive men [6]. Stroke Genetic Risk Factor: Although it is still difficult to distinguish between risk resulting from genetic mutations and risk resulting from common familial exposures, hereditary factors do contribute to stroke risk. Stroke's heterogeneity, the wide range of traditional risk factors that contribute to stroke, and the variation across populations and research have all made the task more difficult. However, there are a number of possible ways that genetic variability could increase the risk of stroke. First, certain familial syndromes for which stroke is the primary or unique manifestation may be caused by particular rare single gene disorders (e.g., cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy, or CADASIL). Second, single gene disorders (e.g., sickle cell anaemia) can result in a multisystem disorder, of which stroke is only one manifestation [6].
Pathogenesis:
Energy failure, loss of cell ion homeostasis, acidosis, elevated intracellular calcium levels, excitotoxicity, free radical-mediated toxicity, production of arachidonic acid products, cytokine-mediated cytotoxicity, complement activation, disruption of the blood-brain barrier (BBB), activation of glial cells, and leukocyte infiltration are just a few of the many processes that contribute to the complex pathophysiology of stroke. The severely impacted ischemic-core regions may experience ischemic necrosis as a result of these coordinated and interconnected events. The core of the brain tissue that experiences the most severe reduction in blood flow is fatally damaged within a few minutes of a cerebral ischemia, and necrotic cell death follows. A zone of less severely damaged tissue surrounds this necrotic core and is rendered functionally silent by decreased blood flow, but keeps up its metabolic activity. Initial cellular and organelle swelling, followed by nuclear, organelle, and plasma membrane disruption, nuclear structure and cytoplasmic organelle disintegration, and extrusion of cell contents into the extracellular space are morphological characteristics of necrosis. Up to half of the entire lesion volume during the early
Table 1- Most Common Symptoms and Signs of Ischemic Stroke
|
Symptom |
Prevalence (%) |
Agreement between examiners (kappa) |
|
Acute onset |
96 |
Good (0.63) |
|
Subjective arm weakness |
63 |
Moderate (0.59) |
|
Subjective leg weakness |
54 |
Moderate (0.59) |
|
Self-reported speech disturbance |
53 |
Good (0.64) |
|
Subjective facial weakness |
23 |
– |
|
Arm paraesthesia |
20 |
Good (0.62) |
|
Leg paraesthesia |
17 |
Good (0.62) |
|
Headache |
14 |
Good (0.62) |
|
No orthostatic dizziness |
13 |
– |
|
Signs |
||
|
Arm paresis |
69 |
Moderate to excellent (0.42 to 1.00) |
|
Leg paresis |
61 |
Fair to excellent (0.40 to 0.84) |
|
Dysphasia or dysarthria |
57 |
Moderate to excellent (0.54 to 0.84) |
|
Hemiparetic/ataxic gait |
53 |
Excellent (0.91) |
|
Facial paresis |
45 |
Poor to excellent (0.13 to 1.00) |
|
Eye movement abnormality |
27 |
Fair to excellent (0.33 to 1.00) |
|
Visual field deficit |
24 |
Poor to excellent (0.16 to 0.81) |
stages of ischemia are made up of the ischemic penumbra, which is the area that borders the infarct core and is where post-stroke therapy may be used to salvage. The penumbra region of a focal
ischemic infarct is an example of less severe ischemia, which develops more slowly, relies on the activation of particular genes, and may eventually lead to apoptosis. According to recent studies, numerous neurons in the ischemic [7].
Diagnosis of Stroke:
On the basis of medical history, physical examination and tests, stroke can be diagnosed. When assessing a stroke, the history is crucial and should highlight symptoms and indicators of focal neurologic injury, such as facial droop, unilateral weakness or sensory deficit, dysarthria, or aphasia (Table 1). A vascular territory is consistent with a sudden and maximal focal neurologic deficit in most patients. Assessing and choosing a course of treatment depend heavily on the timing of events or the onset of symptoms, particularly the last known state or baseline condition. A stroke requires immediate medical attention. Recognizing the symptoms of a stroke in someone can play an important role 7in improving their outcome. Experts recommend you BE-FAST Trusted Source:
• Balance: Are they having trouble with balance or coordination?
• Eyes: Are they experiencing visual symptoms, like double vision or blurry vision?
• Face: Does one side of their face droop if they try to smile?
• Arms: Can they lift both arms or
• is one arm weak or numb?
• Speech: Is their speech slurred or difficult to understand?
• Time: If any of the above symptoms are present, time to call 911 or your local emergency services [8].
Standardized stroke scoring systems should be used to determine severity of injury and prognosis. The National Institutes of Health Stroke Scale (NIHSS) is the most widely used clinical tool. NIHSS scores generally reflect the degree of stroke severity: mild (8 or less), moderate (9 to 15), and severe (16 or more). Stroke scales allow for standardization of communication between clinicians, hospitals, and health care systems to provide an objective means of monitoring for evolving changes in clinical presentation [9].
Current State-of-the-Art Techniques for Stroke Assessment:
• The current gold-standard approach to assessment of stroke requires brain and neurovascular imaging, in addition to the clinical assessment of stroke severity using National Institute of Health Stroke Scale (NIHSS). ICA, internal carotid artery; MCA, middle cerebral artery; EVT, endovascular therapy; CBF, cerebral blood flow; CBV, cerebral blood volume; MTT, mean transit time; CC, collateral circulation; ADC, apparent diffusion coefficient; IVIM, intravoxel incoherent motion imaging.
• Non-contrast computed tomography (NCCT) is quick, accessible, and reasonably priced. In order to rule out acute haemorrhage in patients with suspected AIS, it serves as the primary imaging modality. The Alberta Stroke Program Early CT Score (ASPECTS) is frequently used to evaluate the location and severity of AIS using NCCT images. An expert's interpretation of NCCT images can identify major strokes, but it is noticeably insensitive when it comes to minor strokes. Additionally, NCCT's sensitivity for detecting AIS is low (<20%) in the first three hours and 57–71% in the 24 hours following the onset of a stroke.
• CTP uses information from multiple cerebral CT scans to evaluate blood flow at the capillary tissue level.
• Digital subtraction angiography (DSA) is an outdated technique that is not commonly used today and necessitates invasive action.
• Single phase CT angiography (sCTA) is useful for the rapid evaluation of LVO, and is also useful for evaluation of collateral circulation. Good collaterals on sCTA correlate with reduced ischemic core growth, although no correlation between collateral status and clinical outcome was observed. NCCT is relatively insensitive in detecting early ischemic change in the vertebrobasilar region, so additional CTA is essential for diagnosing vertebrobasilar ischemia.
• Multiphase CTA (mCTA) gives three time-resolved grey-scale images of the cerebral vasculature, with 8 and 16 s delays.
• CT perfusion (CTP) provides comparable diagnosis and prognosis capabilities to mCTA and is often preferred as the colour maps used are easier.
• Digital subtraction angiography (DSA) is an old technology that requires invasive action and is not widely used today. In DSA pre-contrast images taken on fluoroscope are subtracted from the contrast images for better visualization of vasculature. DSA can also be used to determine occlusion location and evaluate collateral circulation, most commonly during EVT. DSA is more invasive than CTA and the interrater reliability of CTA-determined occlusion type has been reported to be better than DSA-determined occlusion type, so CTA is more widely used.
• Magnetic resonance imaging (MRI) has greater sensitivity than any other imaging techniques for AIS detection.
• Diffusion MRI or diffusion-weighted imaging (DWI) is the gold standard for the imaging diagnosis of AIS, detecting it as early as 30 min after the beginning of symptoms. In DWI, diffusion of protons in the tissue is shown and tissues with delayed or restricted proton movement with a low apparent diffusion coefficient (ADC) appear.
• Susceptibility-weighted imaging (SWI), fluid attenuated inversion recovery (FLAIR) and T2-weighted MRI, can be utilized for accurate identification of haemorrhage and other stroke mimics.
• Magnetic resonance angiography (MRA) can be used as an alternative tool to CTA to assess brain perfusion, although it is not as widely used as CTA. Both sCTA and MRA permit quick detection of large vessel occlusion (LVO
• The 2018 Guidelines for Management of Acute Ischemic Stroke from the American Heart Association/ American Stroke Association now recommends that CTP, diffusion-weighted imaging (DWI)- MRI, and/or MRI perfusion (MRP) be included as part of a standard imaging evaluation for patients within 6–24 h of symptom onset. Diagnosis of stroke mimics requires use of MRI or CTP [10].
Recent Advances in diagnosis of stroke:
Magnetic Resonance Imaging (MRI) plays a growing role in acute stroke diagnosis. Despite cost and logistical limitations, MRI is useful for delineating small infarcts and hyperacute events. It can evaluate Intracerebral Haemorrhage (ICH), but is more challenging to interpret than CT. MRI's sensitivity to acute blood detection has improved with gradient recalled echo scans (GRE) and hemosiderin-sensitive sequences. MRI is particularly useful for demonstrating brainstem and cerebellar infarcts, identifying 90% of infarcts at 24 hours, compared to 60% with CT.
Magnetic resonance angiography:
Magnetic resonance angiography (MRA) is a non-invasive imaging technique that uses magnetic resonance technology to produce detailed images of blood vessels. It works by detecting the contrast between flowing blood and stationary tissue, allowing for the visualization of vascular structures without the need for contrast agents or invasive procedures.
Magnetic Resonance Angiography (MRA) Limitations: MRA can detect arterial narrowing, but tends to overestimate the degree of stenosis, especially in severe cases. This is due to turbulence, which reduces signal intensity and can create a "flow gap" where the vessel appears blocked. Combining MRA with duplex ultrasound improves sensitivity and specificity, but 3% of patients with negative non-invasive tests may still have significant lesions. Additionally, 9% of patients with suspected complete occlusion may have some luminal patency on carotid angiography. Therefore, cerebral angiography may still be necessary for some patients with recurrent symptoms and ambiguous non-invasive test results
Diffusion-Weighted MRI (DWI) in Stroke Imaging:
DWI detects ischemic changes by measuring water molecule diffusion in brain tissue. In ischemic areas, water accumulates intracellularly due to cytotoxic edema, appearing bright on DWI. DWI changes correlate with the "ischemic core" and can detect ischemic changes as early as 2 hours after symptom onset. DWI also differentiates between acute and chronic lesions, helping identify new lesions in patients with extensive old ischemic lesions. This technique provides valuable insights into stroke diagnosis and treatment.
• Diffusion-Weighted Imaging (DWI) Sensitivity, DWI has higher sensitivity than standard MRI techniques, detecting:
- 98% of early ischemic lesions (<60 hours) vs. 91% with FLAIR and 71% with T2 imaging
- Hyperacute stroke with increased accuracy
• A study by Gonzalez et al. demonstrated:
- DWI correctly identified stroke in 14 patients within 6 hours of symptom onset
- 8 patients with normal diffusion imaging were discharged without stroke diagnosis and had no infarcts on follow-up imaging
• Recent data emphasize the clinical importance of DWI's increased sensitivity, highlighting its value in:
- Accurately localizing infarcts.
- Identifying acutely symptomatic lesions in unexpected vascular territories (18% of patients).
- Detecting lesions in multiple vascular territories (13% of patients).
• Diffusion-Weighted Imaging (DWI) and MR Perfusion Imaging (MRPI) in Stroke. DWI detects permanently ischemic tissue, while MRPI evaluates tissue perfusion. Combining DWI and MRPI helps identify:
- Infarct core and ischemic penumbra.
- Tissue at risk for continued ischemia.
- Perfusion-diffusion mismatch, indicative of infarct growth.
• Studies show that:
- Larger perfusion defects correlate with infarct expansion.
- DWI and MRPI lesion volumes correlate with neurological outcome.
These imaging techniques may help select patients for aggressive reperfusion measures, but further studies are needed to confirm their effectiveness [11].
Developments in stroke neuroimaging:
In addition to improving our understanding of the structural and functional anatomy of the brain, neuroimaging has significantly aided in the diagnosis of stroke. The application of various pulse sequences and intravenous contrast agents are two examples of technological advancements that have advanced the use of neuroimaging in medical diagnostics over the past few decades. In this section, we talk about emerging technological developments. Computed Tomography (CT) and Magnetic resonance imaging (MRI) plays crucial role in the diagnosis
1. Neuroimaging techniques: CT and MRI are widely used for stroke diagnosis.
2. CT vs. MRI: CT is faster and more widely available, while MRI provides higher resolution images of soft tissues.
3. Advances in CT: Dynamic contrast-enhanced CT, CT angiography (CTA), and CT perfusion (CTP) enhance image resolution and assess microvasculature.
Future Directions
1.Artificial intelligence and machine learning: May improve image analysis and diagnosis.
2.Imaging with contrast agents: Enhances image resolution and provides more detailed information.
3.Thrombus imaging and resonance fingerprinting: May aid in rapid and accurate visualization of stroke [12].
Pharmacotherapy of stroke:
Thrombolysis-
Intravenous alteplase is the only FDA-approved treatment for acute ischemic stroke, improving outcomes for many patients. Recent trials extended the treatment window to 4.5 hours for selected patients. Alteplase promotes thrombolysis by converting plasminogen to plasmin, breaking down blood clots. Fibrin-bound plasmin is protected from inactivation, minimizing systemic effects. Other thrombolytic agents, like streptokinase and urokinase, have systemic effects due to indiscriminate plasminogen activation. Early treatment with alteplase is crucial for favourable outcomes The ECASS III trial and SITS-ISTR registry demonstrated the efficacy and safety of alteplase 3-4.5 hours after ischemic stroke onset. Alteplase administered within this time frame showed improved outcomes (52.4% vs 45.2%) without increasing mortality, despite a higher risk of intracranial haemorrhage.
Anticoagulants-
Heparin: Urgent anticoagulation in acute ischemic stroke patients may lead to intracranial haemorrhage, outweighing potential benefits. The timing of long-term anticoagulation for secondary stroke prevention is debated. Specific circumstances, such as extracranial arterial dissection or high-risk cardiac thrombus, may warrant early anticoagulation. Heparin, with a mean molecular weight of 15,000 Daltons, inactivates thrombin and factor X. However, trials have shown that heparin's benefits are counteracted by increased bleeding, and its use in atrial fibrillation patients did not show a benefit.
• Low Molecular Weight Heparin (LMWH) and Danaparoid:
- LMWHs have a more predictable dose-response relationship and lower risk of heparin-induced thrombocytopenia.
- Trials showed no benefit in using LMWHs or danaparoid in acute ischemic stroke.
• Warfarin:
- A vitamin K antagonist that inhibits factors II, VII, IX, and X.
- No data shows urgent anticoagulation with warfarin provides an acute benefit in AIS.
• Dabigatran:
- An oral anticoagulant that acts as a direct thrombin inhibitor.
- FDA-approved for stroke prevention in non-valvular atrial fibrillation.
- Studies showed dabigatran was effective in reducing stroke occurrence, with lower rates of major haemorrhage.
• Rivaroxaban:
- An oral anticoagulant that inhibits factor Xa.
- FDA-approved for stroke prevention in atrial fibrillation.
- Shown to be non-interactive to war pod in preventing stroke and systemic embolism.
• Apixaban:
- A direct thrombin inhibitor.
- Shown to decrease stroke occurrences and bleeding compared to warped in the Aristotle trial.
- Submitted for FDA approval.
• Antiplatelet Agents:
- Aspirin: irreversibly inhibits cyclooxygenase, preventing platelet aggregation.
- Reduces stroke recurrence and death when initiated within 48 hours of acute ischemic stroke.
- Clopidogrel: irreversibly blocks ADP receptors on platelets.
- Tested against aspirin in the CAPRIE trial for preventing cardiovascular and cerebrovascular events.
• Clopidogrel:
- Irreversibly blocks ADP receptors on platelets.
- Compared to aspirin in the CAPRIE trial, clopidogrel showed a relative risk reduction of 8.7%.
• Combination Antiplatelet Therapy:
- MATCH and CHARISMA trials showed no benefit in combining clopidogrel with aspirin for long-term stroke prevention.
- Increased risk of major bleeding complications.
• Dipyridamole:
- Inhibits adenosine uptake, preventing platelet aggregation.
- Combination with aspirin showed better risk reduction in ESPS II and ESPRIT trials.
• Newer Antiplatelet Agents:
- Tirofiban and eptifibatide (glycoprotein IIb/IIIa inhibitors).
- Ticagrelor, cangrelor, and prasugrel (ADP inhibitors).
- Further studies needed to determine efficacy in acute ischemic stroke [13].
Advances in the pharmacotherapy of stroke:
Currently, conventional therapies for managing stroke and associated complications primarily focus on pharmacological interventions aimed at removing the thrombus and minimizing ischemic injuries to neurons through intravascular therapy or intravenous thrombolysis. Until recently, intravenous administration of recombinant tissue plasminogen activator (rtPA) was considered the sole commercially available treatment for acute ischemic stroke. However, its efficacy is time-dependent, and it carries a risk of intracerebral haemorrhages. Recent advancements have led to the development of novel thrombolytic agents, including fibrin-specific tissue plasminogen activators and chimeric plasminogen activators. Additionally, antiplatelet therapy and anticoagulants are commonly prescribed for secondary stroke prevention. While antiplatelet drugs can help prevent further injuries, they are limited in their ability to repair or shield the affected region. The literature suggests that combining antiplatelet and anticoagulant drugs with neuroprotective agents may offer a promising therapeutic approach. However, the low permeability of neuroprotectants across the blood-brain barrier (BBB) can hinder their clinical translation. Therefore, strategies to enhance neuroprotectant accumulation in ischemic sites are crucial for improving therapeutic efficacy and facilitating clinical translation. Besides overcoming physiological barriers, site-specific drug release and co-delivery to ischemic areas, as well as minimizing side effects on other parts of the body, are significant challenges in stroke treatment. The next generation of stroke therapeutics aims to address these challenges by leveraging nanotechnology to downsize drug carriers, enabling targeted and on-site delivery while effectively crossing the BBB. Nanoscience, which emerged in 1959, is a relatively new field of study focused on the formation of materials at the nanoscale. This innovative technology has opened up new avenues for the diagnosis and treatment of various diseases. Nano-scaled materials have demonstrated rapid and accurate diagnosis, as well as precise treatments with significantly reduced therapeutic doses and side effects. Furthermore, nanotechnology enables the delivery of drugs to targeted and desired regions. The application of nanomaterials in the diagnosis and treatment of stroke is a promising area of research. By harnessing the potential of nanotechnology, researchers aim to develop more effective and targeted therapeutic strategies for stroke management [14].
METHODOLOGY:
Literature review and analysis of current state-of-the-art techniques for stroke assessment and treatment. Data Sources is taken from Peer-reviewed articles, clinical trials, and review papers from reputable scientific databases (e.g., PubMed, Scopus). Inclusion Criteria includes studies published in English, focusing on stroke diagnosis, treatment, and management. Exclusion Criteria includes case reports. Thematic analysis and synthesis of findings to identify key trends, advancements, and challenges in stroke care.
RESULT:
The results of this study highlight significant advancements in stroke diagnosis and treatment. Diffusion-weighted MRI (DWI) has emerged as a crucial diagnostic tool, enabling early detection of ischemic changes. Novel thrombolytic agents, such as fibrin-specific tissue plasminogen activators, have shown improved outcomes and reduced risk of intracerebral haemorrhages. Anticoagulation therapy, including warfarin, dabigatran, rivaroxaban, and apixaban, has been established as effective for secondary stroke prevention. Furthermore, emerging nanotechnologies have demonstrated potential in improving blood-brain barrier permeability and delivering targeted treatments. The combination of these advancements has transformed the landscape of stroke care, enabling more effective diagnosis, treatment, and management. These findings have significant implications for clinical practice, highlighting the need for a multidisciplinary approach to optimize stroke care and improve patient outcomes. Overall, the results of this study provide a comprehensive overview of the current state-of-the-art techniques for stroke diagnosis and treatment.
DISCUSSION:
The results highlight significant advancements in stroke diagnosis and treatment. Diffusion-weighted MRI (DWI) has improved diagnosis, while novel thrombolytic agents and anticoagulation therapy have enhanced treatment options. Nanotechnology has also shown promise in improving blood-brain barrier permeability and delivering targeted treatments. These findings suggest that a multidisciplinary approach, combining cutting-edge imaging techniques, novel thrombolytic agents, and emerging nanotechnologies, may optimize stroke care and improve patient outcomes. However, further research is needed to address remaining challenges and improve access to effective treatments.
CONCLUSION:
In conclusion, the current state-of-the-art techniques for stroke assessment and treatment have significantly improved patient outcomes. Advances in imaging technologies, novel thrombolytic agents, and emerging nanotechnologies have transformed the landscape of stroke care. However, despite these advancements, challenges persist, and further research is needed to optimize stroke care, improve access to effective treatments, and reduce the global burden of stroke
REFERENCES





Jayshri Sawarkar*, Onkar Ramanshetti, Shivani Rathod, Yogesh Shendage, Dr. Ashok Giri, Recent Trends in The Diagnosis and Pharmacotherapy of Stroke, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 398-408. https://doi.org/10.5281/zenodo.14989606
 10.5281/zenodo.14989606
10.5281/zenodo.14989606
