Kamalakshi Pandurangan College of Pharmacy, Ayyapalayam, Tiruvannamalai, Tamil Nadu, India 606603
Quinidine, an alkaloid found naturally in cinchona, has been used extensively in cardiology for more than a century. Since its first isolation as a stereoisomer of quinine from Cinchona bark, it has been extensively utilised in the management and prevention of ventricular and atrial arrhythmias [1,2]. Quinidine, an antiarrhythmic drug that falls under Vaughan-Williams Class Ia, mainly inhibits sodium channels, which lengthens the action potential and refractory period [4,5]. It is still essential in specific situations, such as Brugada syndrome, short QT syndrome, and some hereditary arrhythmias [3,10,15], even though its broad use has decreased because of the risk of proarrhythmia and the availability of safer antiarrhythmic medications [6]. Quinidine's history, pharmacology, clinical use, safety issues, and changing function in contemporary treatment are all well covered in this review.
Quinidine's history starts in South America's tropical jungles, where native people used the bark of the Cinchona plant to cure fevers. The bark's main ingredients, quinine and its stereoisomer quinidine, were first used in Europe as a malaria treatment in the 17th century and have since become essential to contemporary pharmacology [1,2].
Although quinine gained notoriety for its ability to treat malaria, quinidine became a powerful treatment for irregular heartbeats in the early 1900s [3]. It was a vital treatment prior to the development of beta-blockers, calcium channel blockers, and amiodarone because of its capacity to stabilise myocardial excitability.
2. PHARMACOLOGY AND MECHANISM OF ACTION
Quinidine's impact on cardiac ion channels is responsible for its antiarrhythmic actions. By obstructing rapid inward sodium channels, this Class Ia drug slows phase 0 depolarisation and lowers the action potential's rate of increase [4,5]. The atria, ventricles, and Purkinje fibres all experience a decreased conduction velocity as a result. Quinidine also blocks certain potassium channels, which increases the effective refractory time and prolongs repolarisation [6].
Beyond its primary sodium channel-blocking effects, quinidine also exerts:
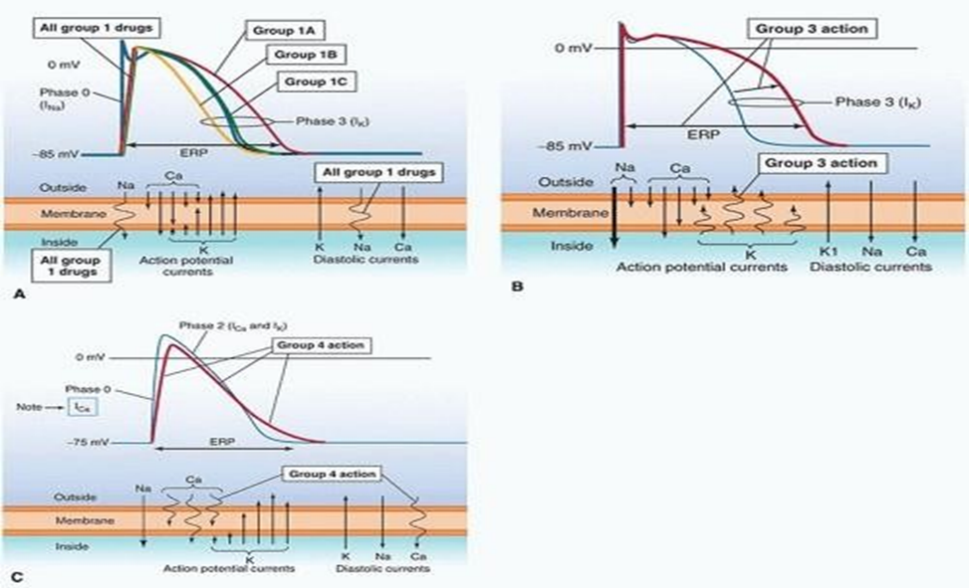
Fig.1 Mechanism of Action in Quinidine
3. CLINICAL APPLICATIONS
3.1 Controlling Ventricular and Atrial Arrhythmias:
Quinidine has long been a first-line treatment for sinus rhythm restoration following a atrial fibrillation or flutter and then for avoiding recurrence [8]. In patients who are not responds to previous treatments, it is also useful in treating potentially fatal ventricular tachycardia [9].
3.2 Role in Brugada Syndrome and Other Channelopathies:
Brugada syndrome Quinidine has been demonstrated to modify repolarisation and hence decrease arrhythmic events in Brugada syndrome, where the transient outward potassium current (Ito) plays a role in arrhythmogenesis [3,10]. Benefits are comparable for idiopathic ventricular fibrillation and short QT syndrome [15].
3.3 Adjunct in Severe Malaria:
While rarely used today for infectious disease, intravenous quinidine remains an option for severe Plasmodium falciparum malaria when quinine or artesunate is unavailable [2,11].
4. ADVERSE EFFECTS AND SAFETY CONSIDERATIONS
Quinidine's limited therapeutic index and potential for severe side effects limit its clinical utilisation [5,6].
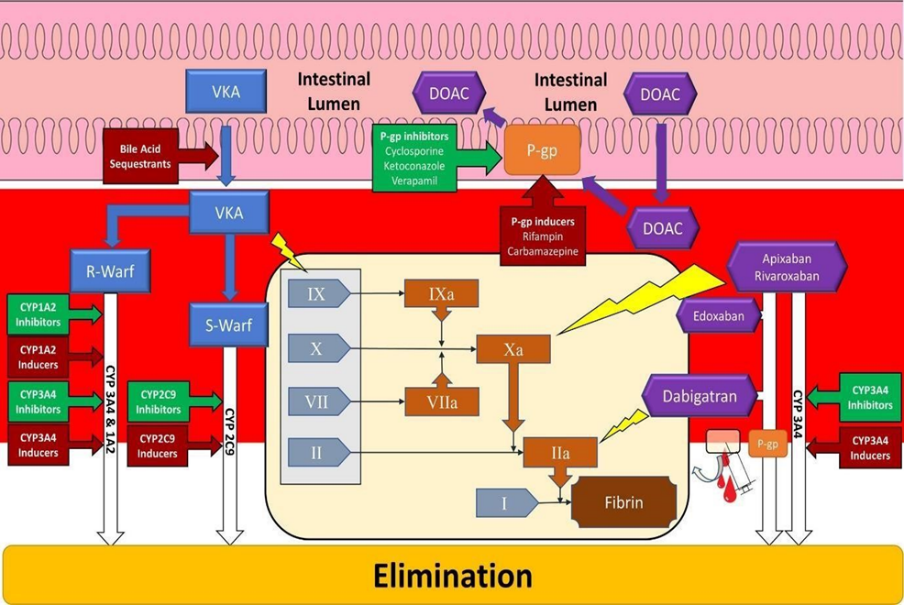
Fig.2 Drug Interactions
4.1 Drug interactions:
Digoxin, warfarin, and certain antidepressants are significantly impacted by the strong suppression of CYP2D6 and P-glycoprotein [14]. To reduce risk, careful patient selection, ECG monitoring, and dose modification based on hepatic and renal function are crucial.
5. INSIGHTS ON QUINIDINE THERAPY
5.1 Therapeutic Drug Monitoring and Dose Individualization:
Therapeutic drug monitoring (TDM) is essential for maximising treatment and reducing toxicity due to quinidine's limited therapeutic window and inter-individual metabolic variability [5]. To guide dose modifications and prevent negative effects, plasma quinidine concentrations should be routinely measured, particularly in individuals with hepatic or renal impairment.
5.2 Pharmacogenomics and Metabolic Variability:
Current research emphasises how quinidine metabolism is impacted by genetic variations in CYP2D6, which affect plasma levels and clinical response [14]. Personalised strategies that take pharmacogenomic characteristics into account could increase efficacy and safety.
5.3 Electrophysiological Monitoring:
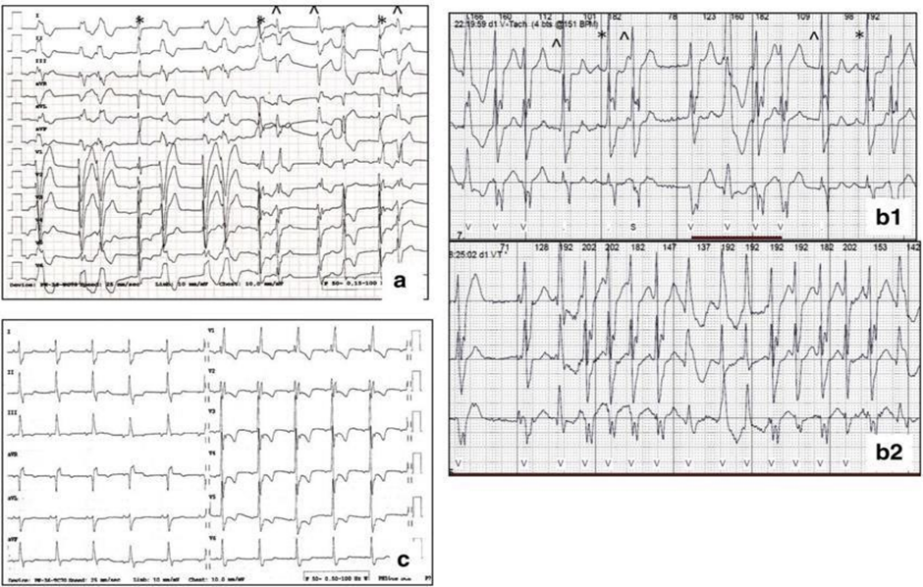
Fig.3 Electrocardiogram of Quinidine
During quinidine therapy, it is recommended to continuously monitor the electrocardiogram, particularly for patients who have baseline QT prolongation or who are on concurrent drugs that impact cardiac repolarisation [6]. Patients who are most likely to benefit from quinidine medication can also be identified with the use of sophisticated electrophysiological testing.
6. MODERN RELEVANCE AND FUTURE DIRECTIONS
As catheter ablation and more recent antiarrhythmics have become more common, quinidine has become a specialised but necessary treatment [3,10]. Particularly in uncommon hereditary arrhythmias when specific ion channel regulation is necessary, recent research indicates that its distinct electrophysiological profile might make it a perfect candidate for precision cardiology [15]. Further investigation into its modifiedrelease formulations and stereoisomeric analogues could improve its safety and efficacy profile.
7. PHARMACOGENOMICS AND PERSONALIZED THERAPY
Recent developments in pharmacogenomics have brought attention to how genetic variability affects the safety and therapeutic efficacy of quinidine. Genetic variations in drug-metabolizing enzymes, including CYP2D6, have been demonstrated to dramatically change medication clearance rates and plasma levels, which may affect antiarrhythmic action as well as the likelihood of side effects [14].
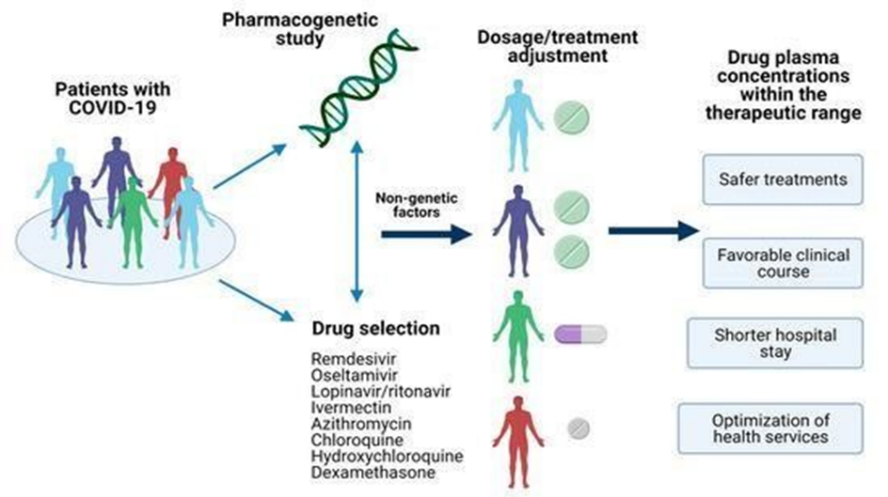
Fig.4 Pharmacogenomics Therapy
A compelling option for genotype-guided therapy, quinidine may also affect patientspecific responsiveness due to variations in ion channel genes, especially those encoding sodium and potassium channels [3,10,15]. This precision-based method can improve therapy results in uncommon channelopathies, minimise the occurrence of proarrhythmic events as torsades de pointes [6,13], and optimise dose selection. Integrating genetic screening into clinical decision-making could reinterpret quinidine's function as the area of cardiovascular pharmacogenomics develops, enabling its more efficient, individualised, and targeted delivery.
CONCLUSION
Quinidine's lasting influence highlights the significance of natural substances in the history of medicine. For certain viral disorders and high-risk arrhythmias, it remains a useful tool in the cardiologist's toolbox, even though normal use has decreased. In specialised care, quinidine is still a useful therapeutic agent despite its historical status because to rekindled scientific interest and cautious clinical use.
REFERENCES







K. Panchatcharam, P. K. Gokul, C. Velumurugan, N. Kumaran, Dr. H. Muhammad Rafeek, Dr. N. Gnanasekar, Dr. D. Rajalingam, Quinidine – A Natural Alkaloid with a Timeless Role in Cardiac Care, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1543-1548. https://doi.org/10.5281/zenodo.16875088
 10.5281/zenodo.16875088
10.5281/zenodo.16875088
