Spurthy College of Pharmacy.
Background: Type 2 diabetes is a growing health concern, and the economic burden of managing the disease is substantial. The study aims to evaluate the prescription pattern and pharmacoeconomics of drugs used in type 2 diabetics. Objectives: To analyze the prescription pattern of drugs used in type 2 diabetics. To assess the pharmacoeconomic profile of commonly used drugs. To identify areas for optimization of drug therapy and cost-effective management. Methods: Prospective analysis of prescription data from 200 patients with type 2 diabetes. Evaluation of prescription pattern using WHO prescribing indicators. Pharmacoeconomic analysis using cost-minimization and cost-effectiveness approaches. Expected outcomes: Identification of common prescription patterns and potential areas for improvement. Comparison of pharmacoeconomic profiles of different drug classes and regimens. Recommendations for cost-effective management of type 2 diabetes Significance: This study will provide insights into the prescription pattern and pharmacoeconomics of drugs used in type 2 diabetics, enabling healthcare providers and policy-makers to make informed decisions about optimal drug therapy and resource allocation.
Diabetes mellitus (DM) is a condition characterized by insufficient regulation of blood glucose levels. It encompasses various subtypes, such as type 1, type 2, maturity-onset diabetes of the young (MODY), gestational diabetes, neonatal diabetes, and steroid- induced diabetes. Type 1 and type 2 DM are the primary forms, each with distinct underlying mechanisms, symptoms, and treatment approaches, yet both carry the risk of hyperglycemia. This overview discusses the pathophysiology, assessment, and treatment of DM, emphasizing the importance of a collaborative approach in patient care. [1]
Graphical Abstract:
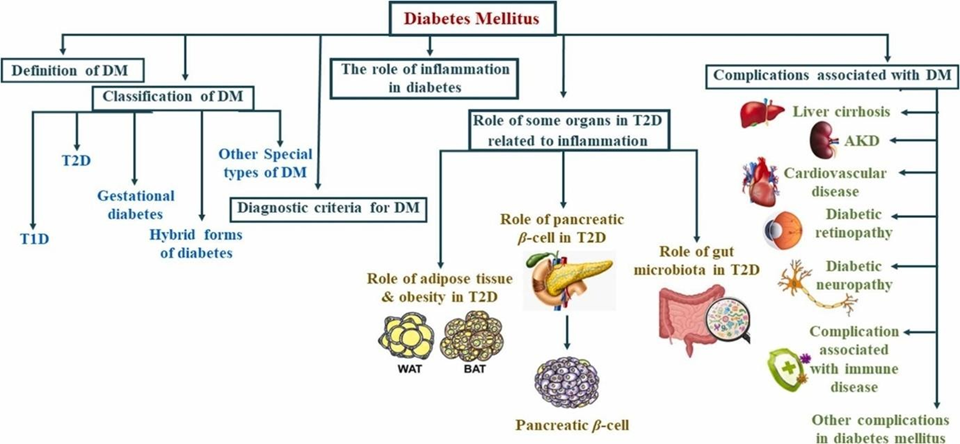
Figure: 1
Introduction:
The term “diabetes mellitus” derives from the Greek word ‘diabetes’, meaning “siphon” or “to pass through,” and the Latin word ‘mellitus’, meaning “sweet”. Apollonius of Memphis first used the term “diabetes” around 250 to 300 BC. Ancient Greek, Indian, and Egyptian civilizations recognized the sweet taste of urine in this condition, which led to the term ‘Diabetes Mellitus’. In 1889, Mering and Minkowski discovered the pancreas’s role in the development of diabetes. Then, in 1922, Banting, Best, and Collip successfully isolated insulin from cow pancreas at the University of Toronto, marking the beginning of effective diabetes treatment. Despite significant advances and ongoing research, diabetes remains a prevalent chronic disease both in the US and globally, and it is the seventh leading cause of death in the US. [1]. Diabetes is a condition characterized by elevated blood sugar (glucose) levels. It arises when the pancreas either fails to produce enough insulin or doesn’t produce any at all, or when the body does not respond effectively to insulin. Diabetes can affect individual of any age and is typically a chronic condition that can be managed with medication and/or lifestyle changes. Glucose, which primarily comes from the carbohydrates in food and drinks, is a crucial energy source for the body. Blood carries glucose to cells for energy use. For glucose to enter cells, it needs insulin, a hormone that acts as a “key”. If the pancreas doesn’t produce sufficient insulin or the body doesn’t utilize it correctly, glucose accumulates in the bloodstream, leading to high blood sugar (hyperglycaemia). Consistently high blood glucose levels can result in serious health complications, such as heart disease, nerve damage, and eye problems. The technical term for diabetes is ‘diabetes mellitus’. It should be noted that there is another condition called ‘diabetes insipidus’ that also involves increased thirst and frequent urination. However, diabetes insipidus is much less common and is different from diabetes mellitus.
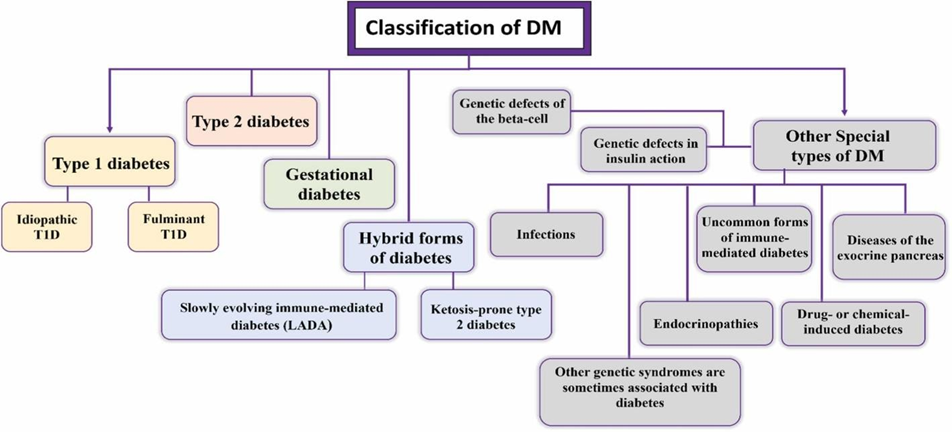
Figure: 2
Type 1 Diabetes:
Type 1 diabetes (T1D) can be identified before abnormal insulin secretion begins. Evidence shows that there is a gradual decline in insulin production that starts at least two years prior to diagnosis. [2]This is an autoimmune condition where the immune system mistakenly attacks and destroys the insulin-producing cells in the pancreas for reasons that are not fully understood. It accounts for up to 10% of all diabetes cases. Although it is commonly diagnosed in children and young adults, it can develop at any age. Ketoacidosis is often the most common initial symptom of the illness in many people. The autoimmune destruction of beta cells has been associated with variousfactors, including genetic predisposition, environmental influences, and unknown causes. In some cases of Type 1 diabetes mellitus (T1DM), the origin is not well understood, particularly among individuals of African or Asian descent. [3]
Idiopathic T1D:
Idiopathic Type 1 diabetes is a form of diabetes that lacks autoantibodies but still necessitates insulin for survival. It is characterized by: persistent insulin deficiency, susceptibility to ketoacidosis, and the absence of autoantibodies. Mainly happen in Asian and African.
Fulminant T1D:
This distinctive form of Type 1 diabetes, first identified in 2000, shares some features with idiopathic Type 1 diabetes, such as not being immune-mediated. [4]This is a rare and severe subtype of Type 1 diabetes, marked by an abrupt transition from normal blood glucose levels to severe hyperglycaemia and ketoacidosis. Approximately 20% of Japanese individuals with acute-onset Type 1 diabetes (between 5,000 and 7,000 cases) experience this condition, which has been primarily described in East Asian countries. It is characterized by extremely rapid and nearly complete destruction of β-cells, resulting in almost no remaining insulin production. This condition is often linked to certain environmental and genetic factors. It is believed that an intensified immune response, possibly triggered by an antiviral reaction, targets pancreatic β-cells without the usual formation of autoantibodies. There have also been cases of this type of diabetes occurring during pregnancy.
Type 2 Diabetes:
Type 2 diabetes mellitus (T2DM) affects 90% to 95% of individuals with diabetes. It is characterized by a complex interplay where the primary problem is the balance between insulin production by beta cells and the body’s response to insulin. This results in insulin resistance, where the body’s cells do not effectively respond to insulin-stimulated glucose uptake. [5]In insulin-resistant obese patients with Type 2 diabetes, absolute insulin levels can be higher compared to insulin-sensitive lean individuals. However, these levels are insufficient relative to the severity of their insulin resistance. Additionally, the first-phase insulin production, which is the initial burst of insulin released in response to glucose stimulation, is often significantly reduced or absent. [6]Impaired glucose tolerance is an intermediate stage of the illness that can indicate an increased risk of developing heart disease. [3]Hyperglycaemia generally worsens and becomes more difficult to manage over time. Additionally, the progressive decline in β- cell function is a key characteristic of the advancement of Type 2 diabetes. [7]
Gestational diabetes:
Pregnancy-related hyperglycemia heightens the risk of adverse outcomes for the mother, foetus, and new-born. [8]While most cases of pregnancy-related hyperglycemia resolve after delivery, the definition used does not account for whether the condition persisted beyond pregnancy. It also does not rule out the possibility that undetected glucose intolerance may have either preceded or developed concurrently with the pregnancy. [3]Although most instances of pregnancy-related hyperglycaemia resolve following delivery, the definition employed does not consider whether the condition continues after pregnancy. It also does not exclude the possibility that underlying glucose intolerance may have existed prior to or developed alongside the pregnancy. [9]Following discussions in 2008–2009, the International Association of the Diabetes and Pregnancy Study Groups (IADPSG), which includes representatives from various obstetrical and diabetes organizations, such as the American Diabetes Association (ADA), advised that high-risk women diagnosed with diabetes at their initial prenatal visit using standard criteria should be classified with overt diabetes rather than gestational diabetes. The ADA has since made slight adjustments to these diagnostic recommendations based on a recent National Institutes of Health (NIH) consensus report. [3]
Symptoms:
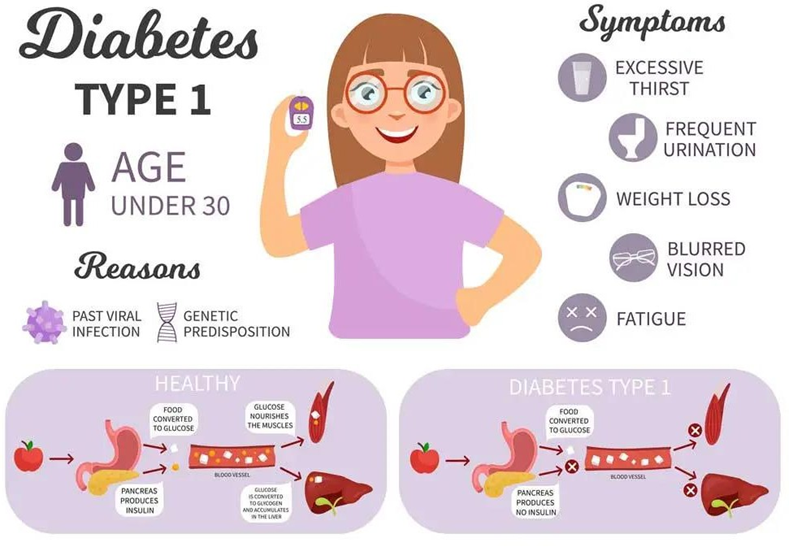
Figure: 3- Symptoms of Type-1 Diabetes
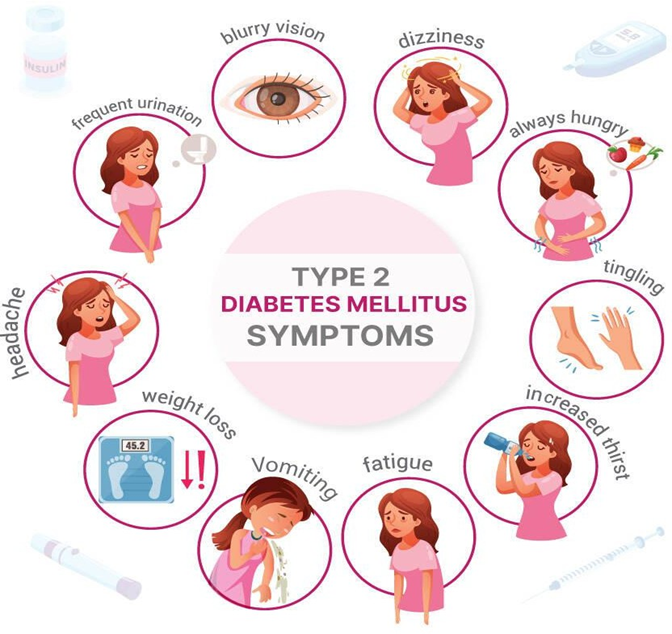
Figure: 4- Symptoms of Type-ΙΙ Diabetes
Causes of Type-1 diabetes:
Type 1 diabetes occurs when the immune system erroneously attacks and destroys the insulin-producing cells in the pancreas, leading to a complete lack of insulin. This process can unfold over months or years. While the exact cause of Type 1 diabetes remains unclear, there is a strong genetic component involved. The likelihood of developing the disease without a family history is about 0.4%. If your biological mother has Type 1 diabetes, your risk is between 1% and 4%, and if your biological father has it, the risk is between 3% and 8%. If both parents have Type 1 diabetes, the risk can rise to as high as 30%. Researchers believe that environmental factors, such as viruses or toxins, may trigger the immune system to attack pancreatic cells in individuals who are genetically predisposed to Type 1 diabetes.
Causes of Type-2 diabetes:
Cells in muscles, fat, and the liver develop insulin resistance, meaning they don’t absorb sugar effectively. Consequently, the pancreas is unable to produce enough insulin to maintain blood sugar levels within a healthy range.
Risk factors:
Several factors can increase the risk of developing diabetes:
Weight: Being overweight or obese is a primary risk factor.
Fat Distribution: Storing fat primarily in the abdomen, rather than in the hips and thighs, is associated with a higher risk. Men with a waist circumference above 40 inches (101.6 centimetres) and women with a waist measurement above 35 inches (88.9 centimetres) are at increased risk.
Inactivity: A sedentary lifestyle raises the risk, as physical activity helps control weight, uses glucose for energy, and improves insulin sensitivity.
Family History: Having a parent or sibling with type 2 diabetes increases an individual’s risk.
Race and Ethnicity: Certain racial and ethnic groups, including Black, Hispanic, Native American, Asian, and Pacific Islander populations, are at higher risk than white populations.
Blood Lipid Levels: Low levels of high-density lipoprotein (HDL) cholesterol, the “good” cholesterol, and high levels of triglycerides are linked to a higher risk.
Age: The risk of type 2 diabetes increases with age, particularly after 35.
Prediabetes: This condition, where blood sugar levels are higher than normal but not high enough to be classified as diabetes, often progresses to type 2 diabetes if left untreated.
Pregnancy-Related Risks: The risk is higher for individuals who had gestational diabetes or gave birth to a baby weighing more than 9 pounds (4 kilograms).
Polycystic Ovary Syndrome (PCOS): This condition, which includes symptoms like irregular menstrual periods, excess hair growth, and obesity, increases the risk of developing type 2 diabetes.
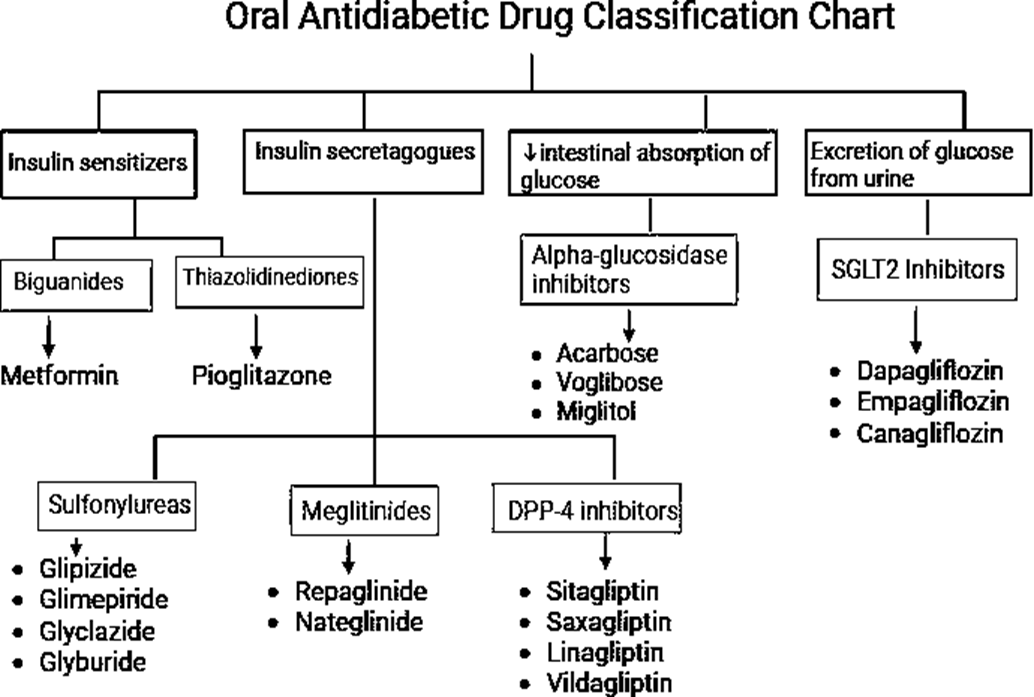
Figure: 5- Classification of Anti-Diabetic Drugs
Mechanism of Action:
The lifespan of type 2 diabetic patients is increasing steadily because of the availability of a wide range of antidiabetic drugs. These drugs decrease blood glucose levels by multiple mechanisms. Metformin, a widely used hypoglycaemic drug, acts by increasing glucose utilization in the peripheral tissues and by reducing hepatic glucose output. Sulfonylureas stimulate insulin secretion from pancreatic β cells. The use of this class of drug is associated with Hypoglycaemic episodes. Thiazolidinediones (TZDs) improve the sensitivity of adipose tissue, skeletal muscles, and the liver towards insulin. Incretin therapies, such as DPP-4-resistant GLP-1 analogues and DPP-4 inhibitors that enhance endogenous GLP-1 levels, promote pancreatic release of insulin. In addition, they are reported to have insulin-independent actions in other tissues, including the brain. Recently introduced SGLT2 inhibitors increase glucose excretion in the urine by preventing glucose reabsorption in the renal tubules. Overall, these antidiabetic drugs have been shown to have beneficial actions in the brain either directly or indirectly through glycaemic control.
Figure: 6- MOA of Anti-Diabetic Drugs
Pharmacoeconomics:
Economics, the study of scarcity and choice, is an inherent part of daily life. Within this broader discipline, health economics applies economic principles to healthcare, facilitating informed decision-making.
This field encompasses:
A subset of health economics, pharmacoeconomics, adapts these principles to pharmaceuticals and policy. It assesses the value of additional benefits relative to additional costs. Pharmacoeconomics is formally defined as “The systemic analysis and description of pharmaceutical costs within healthcare systems and society, comparing costs and consequences of pharmaceutical products and services”. [10]
Economic evaluation serves as a crucial tool, balancing costs and benefits through a structured framework. This process enables decision-makers to make evidence-based choices. All economic evaluation shares a common methodology:
The integration of economic principles into healthcare and pharmaceutical decision making, through health economics and pharmacoeconomics, enables informed resource allocation, optimises healthcare delivery, and improve patient outcomes. [11].
Review Of Literature
J Basic Clin Pharm et.al, 2013 Conducted prospective study on prescription pattern, calculate the cost of antidiabetic drugs and to evaluate the adherence to treatment guidelines in diabetic patients attending the medicine outpatient department in a tertiary care teaching hospital. The study was carried out in 250 patients over a period of 5 month. Out of 250 patients 126 (50.4%) were male and rest were female. A total of 1,391 drugs were prescribed, with mean of 5.56 ± 2.52 drugs and out of which 539 drugs were antidiabetics with mean of 2.18 ± 0.96. In monotherapy, metformin was frequently 218 (40.45%) prescribed. Glimepiride and metformin was the most frequently prescribed in 119 (76.28%) out of 156 antidiabetic drug combinations. Most commonly used drugs other than antidiabetics were aspirin 146 (18.9%) and atorvastatin 119 (15.41%). Mean cost of therapy for a month for a diabetic patient was 354.60 ± 305.72 INR. Majority 209 (83.6%) of prescriptions was in accordance to guidelines. The therapy cost for a diabetic patient ranged from 15 to 2501 INR per month and most of the patients fall in the cost range of 100-400 INR i.e. in 68.4% of the patients. Mean cost of therapy for a diabetic patient was 354.60 ± 305.72 INR. Percentage cost variation, which ranges from 1.47 to 181.81 for Glimepiride + Metformin + Pioglitazone and glimepiride alone, respectively. The study concluded that Metformin was the most frequently prescribed drug in the diabetes patient. Metformin and glimepiride being the most frequent combination used. Majority of the prescriptions followed standard guidelines. [12]
Nihar R Desai et al. 2012 conducted study on the use of specific drugs for the initial management of type 2 diabetes and to estimate the economic consequences of non- recommended care. The study was carried out in 254,973 patients, aged 18 to 100 years, who were newly initiated on oral hypoglycemic monotherapy, over the period of January 1, 2006, and December 31, 2008, by using prescription claims data from a large pharmacy benefit manager. Linear regression models were used to assess whether medication initiation patterns changed over time. Over the course of the study period, the proportion of patients initially treated with metformin increased from 51% to 65%, whereas those receiving sulfonylureas decreased from 26% to 18% (P<.001 for both). There was a significant decline in the use of thiazolidinediones (20.1%-8.3%, P<.001) and an increase in prescriptions for dipeptidyl peptidase-4 inhibitors (0.4%-7.3%, P<.001). Younger patients, women, and patients receiving drug benefits through Medicare were least likely to initiate treatment with metformin. Combined patient and insurer spending for patients who were initiated on alpha-glucosidase inhibitors, thiazolidinediones, meglitinides, or dipeptidyl peptidase-4 inhibitors was $677 over a 6-month period compared with $116 and $118 for patients initiated on metformin or a sulfonylurea, respectively, a cost difference of approximately $1120 annually per patient. [13].
A. Penfornis et.al,2012 conducted observational study to describe insulin therapy in patients with diabetes, to determine treatment costs and to compare costs among treatment regimens. This observational study was performed by 734 French pharmacists. Out of the total of 361 patients with T1DM and 1902 with T2DM were enrolled in the survey. Patients with T1DM more frequently took 1–2 injections per day (46.3% of patients) and used single-dose basal insulin together with ≥ 1 dose of rapid insulin (43.8%). Patients with T2DM used multiple treatment regimens, with 58 different combinations documented. Most took basal/intermediate insulin only (42.5%) or combinations of basal/intermediate and rapid insulins (52.7%). Mean cost of insulin therapy was € 27.4/week for T1DM and € 45.4/week for T2DM. In T1DM, insulin was the biggest cost component and increased with the number of injections/day. In T2DM, nurse visits were the most important cost contributors irrespective of treatment regimen. Overall, the cost of insulin therapy increased with the complexity of the insulin schemes. The study concluded that Considerable heterogeneity is found in insulin treatment regimens used in everyday diabetes care. [14].
Liaquat Ali et.al 2019, Conducted study to estimate the cost-of-illness of type 2 diabetes and to find its determinants in Bangladesh. This cross-sectional study was conducted in 2017 to recruit 1253 participants with type 2 diabetes. Among the participants, 54% were male. The mean (±SD) age was 55.1 ± 12.5 years and duration of diabetes was 10.7 ± 7.7 years. The average annual cost was US$864.7 per patient. Medicine cost accounted for 60.7% of the direct cost followed by a hospitalisation cost of 27.7%. The average annual cost for patients with hospitalisation was 4.2 times higher compared to those without hospitalisation. Being females, use of insulin, longer duration of diabetes, and presence of diabetes complications were significantly related to the average annual cost per patient. The study concluded that the cost of diabetes care is considerably high in Bangladesh, and it is primarily driven by the medicine and hospitalisation costs. [15].
Dr. Won Chan Lee et.al 2012,Conducted retrospective study To evaluate claims- related treatment adherence, health care resource utilization, and associated costs of therapy conversion from an insulin vial and syringe to a premixed biphasic insulin analog pen device among privately insured patients with type 2 diabetes mellitus This study includes total Four hundred eighty-six adult patients with a confirmed diagnosis of type 2 diabetes who converted from an insulin analog vial and syringe (233 patients) or a human insulin vial and syringe (253 patients) to a biphasic insulin analog pen device between July 1, 2001 and December 31, 2002. After conversion, MPR increased significantly from 59% to 68% (p<0.01). A significant decrease in the likelihood of experiencing a Hypoglycemic event was also observed after conversion (odds ratio [OR] 0.40, 95% confidence interval [CI] 0.27–0.61, p<0.05), with Hypoglycemic occurrences reduced nearly two thirds among subjects with optimal adherence indicated by an MPR of 80% or greater (incidence rate ratio 0.36, 95% CI 0.11–0.76, p<0.05). Significant decreases in hypoglycemia-attributable emergency department visits (OR 0.36, 95% CI 0.16–0.84, p<0.05) and physician visits (OR 0.39, 95% CI 0.20–0.77, p<0.05) were observed. Total mean all-cause annual treatment costs were reduced by $1748/patient (p<0.01), hypoglycemia-attributable costs were reduced by $908/patient (p<0.01), and other diabetes-attributable costs were reduced by $643/patient (p<0.01). Patients with an MPR of 80% or greater were associated with significant reductions in all-cause health care costs (OR 0.55, 95% CI 0.31–0.80, p<0.05). The study concluded that, the patients with type 2 diabetes may exhibit considerable improvements in clinical and economic outcomes after insulin therapy conversion from vial and syringe to a premixed biphasic insulin analog pen device. [16].
Christian Hampp et.al 2014 Conducted study to describe market trends for antidiabetic drugs, focusing on newly approved drugs, concomitant use of antidiabetic drugs, and effects of safety concerns and access restrictions on thiazolidinedione use. Since 2003, the number of adult antidiabetic drug users increased by 42.9% to 18.8 million in 2012. Metformin use increased by 97.0% to 60.4 million prescriptions dispensed in retail pharmacies in 2012. Among antidiabetic drugs newly approved for marketing between 2003 and 2012, the dipeptidyl peptidase-4 (DPP-4) inhibitor sitagliptin had the largest share with 10.5 million prescriptions in 2012. Rosiglitazone use plummeted to <13,000 prescriptions dispensed in retail or mail-order pharmacies in 2012. Concomitancy analyses showed that 44.9% of metformin use was for monotherapy. Between 33.4 and 48.1% of sulfonylurea, DPP-4 inhibitor, thiazolidinedione, and glucagon-like peptide 1 analog use was not accompanied by metformin. This study concluded that The antidiabetic drug market is characterized by steady increases in volume, and newly approved drugs experienced substantial uptake, especially DPP-4 inhibitors. The use of rosiglitazone has been negligible since restrictions were put in place in 2011. [17].
Kazeem B. Yusuff et.al 2008, conducted study to describe the pattern of anti-diabetic drug prescribing; ascertain the level of glycemic control, adherence with prescribed anti-diabetic medications, and diabetes self-management practices among patients with type- 2 diabetes in a tertiary care setting in Nigeria .The study consisted of two phases. A cross-sectional review of randomly selected 200 case notes of type 2 diabetic patients that attended the Endocrinology clinic over 3 month; and cross-sectional interviews, with a pre-tested Adherence and Self-Management Monitoring Tool (ASMMT), of 200 consecutive patients that presented their drug prescriptions at the satellite pharmacy unit over a 4 week period at a 900-bed teaching hospital located in Ibadan, South-Western Nigeria. Results Oral Hypoglycemic Agents (OHA) were prescribed for 86% (171) of cohorts while insulin and OHA was prescribed in 14% (29). About 70.8% (121) of patients on OHA were on combination therapy. The most frequently prescribed OHA combination was glibenclamide and metformin (95.8%). Glibenclamide was prescribed as twice daily regimen in 69% of cohorts. The most frequently documented side effect was hypoglycemia (60.3%). Only 44% (88) of cohorts had adequate glycemic control; of these, 93% (82) were adjudged adherent with prescribed anti-diabetic drugs. Interviews with the structured ASMMT revealed that 59% of patients were non- adherent with the previous anti-diabetic drugs due to lack of finance (51.7%); side effects (34.5%); perceived inefficacy of prescribed anti-diabetic drugs leading to self- medication with local herbs (13.8%). Only 20% of non-adherent patients claimed disclosure to physicians during consultation. The identified factors for non-disclosure were lack of privacy during consultation (58%); and short consultation time (42%). The knowledge and practice of critical components of diabetes self-management behaviors were generally low among the cohort studied. However, it was significantly higher among patient judged adherent with their prescribed anti-diabetic medications (P < 0.05). Conclusion Majority of patients with type 2 diabetes in an ambulatory tertiary care setting in Nigeria are managed with OHA combinations, mainly glibenclamide and metformin. While the current prescribing strategy achieved glycemic control in about one third of patients, majority are still not meeting the recommended blood glucose targets due to poor adherence with prescribed drug regimen, and poor knowledge and practice of successful self-management. [18]
S Grover, et.al 2005, Conducted study to assess the cost of care of Indian patients with diabetes mellitus. This study includes 50 outpatients with diabetes mellitus (diagnosed according to WHO criteria, Expert Committee, 1997) was assessed over a six month period using a specially designed questionnaire, together with structured assessments of disability. Total annual cost of care was 14 508 rupees (263.78 euros). The largest proportion of the total cost was made up of direct costs (68%), followed by indirect costs (28.76%) and provider’s costs (2.8%). Drug costs were high. Total treatment cost was significantly higher in those who were more educated, those who visited the hospital more often, and those receiving a greater number of drugs. This study concluded that diabetes mellitus is an expensive illness to treat even in developing countries. The main brunt of financial burden is borne by the family. [19]
Mette Hammer, et.al 2015 conducted retrospective cohort study using administrative claims data from July 2009 through September 2013. A total of 1321 patients were identified. The mean PDC was 0.59 and 34% of patients were classified as adherent, while 60% were persistent over 12 months of follow-up. Adherent and persistent patients were more likely to achieve each of the A1C goals than their non-adherent and non-persistent counterparts after adjusting for patient characteristics. Adherence and persistence were associated with higher adjusted diabetes-related pharmacy and total healthcare costs during follow-up; whereas persistent patients had significantly lower diabetes-related medical costs than non-persistent patients. The study concluded that Persistent patients showed significantly lower medical costs versus those discontinuing liraglutide. Total healthcare costs were higher for adherent and persistent cohorts driven by higher pharmacy costs. [20]
Matt Petersen et.al 2008, conducted study to quantify the economic burden of diabetes caused by increased health resource use and lost productivity, and to provide a detailed breakdown of the costs attributed to diabetes. This study uses a prevalence-based approach that combines the demographics of the population in 2007 with diabetes prevalence rates and other epidemiological data, health care costs, and economic data into a Cost of Diabetes Model. The total estimated cost of diabetes in 2007 is $174 billion, including $116 billion in excess medical expenditures and $58 billion in reduced national productivity. Medical costs attributed to diabetes include $27 billion for care to directly treat diabetes, $58 billion to treat the portion of diabetes-related chronic complications that are attributed to diabetes, and $31 billon in excess general medical costs. The largest components of medical expenditures attributed to diabetes are hospital inpatient care (50% of total cost), diabetes medication and supplies (12%), retail prescriptions to treat complications of diabetes (11%), and physician office visits (9%). People with diagnosed diabetes incur average expenditures of $11,744 per year, of which $6,649 is attributed to diabetes. People with diagnosed diabetes, on average, have medical expenditures that are ∼2.3 times higher than what expenditures would be in the absence of diabetes. For the cost categories analysed, ∼$1 in $5 health care dollars in the U.S. is spent caring for someone with diagnosed diabetes, while ∼$1 in $10 health care dollars is attributed to diabetes. Indirect costs include increased absenteeism ($2.6 billion) and reduced productivity while at work ($20.0 billion) for the employed population, reduced productivity for those not in the labour force ($0.8 billion), unemployment from disease-related disability ($7.9 billion). [21].
Khadka Sheela et al ,2023 conducted retrospective, cross-sectional study to examines the differences in such outcomes between SGLT-2 Inhibitors (SGLT-2), DPP-4 Inhibitors (DPP-4), and GLP-1 Receptor Agonists (GLP-1). This study aim was to compare diabetes-related all-cause hospitalisation between the SGLT-2, GLP-1, and DPP-4 users with Type 2 Diabetes (T2DM) and total healthcare expenditure, emergency expenditure, and prescription expenditure. This retrospective, cross-sectional study was done from the year 2015 to 2019. Out Of the total, 1,965 hospital-visited patients were identified to be receiving either SGLT-2 (n= 306), GLP-1 (n=392), or DPP-4 (n=819). Unadjusted total all-cause average inpatient visit and outpatient visits were significantly lower with the SGLT-2 cohort (1.64; p= 0.05 and 5.52; p<0.01, respectively). However, unadjusted total health, inpatient, and prescription expenditures were significantly higher among the GLP-1 cohort ($24,924, $6,162, and $12,066, respectively; p<0.0001). After adjusting, total health expenditure keeping SGLT-2 as a reference, with every unit increase in GLP-1 and DPP-4 prescription, health expenditure increased in a significant manner by $0.1371 and decreased by $0.2235 respectively, whereas the prescription expenditure was significantly lower in the DPP-4 ( = -0.3342; p= 0.02) compared to SGLT-2. However, there were no significant differences in the emergency and inpatient visits between the three cohorts after adjusting for the socioeconomic factors. Conclusion: This study noted that the patient on SGLT-2 therapy experienced a minimum number of hospital visits in comparison to other drugs and GLP-1 cohort was associated with higher total health expenditure. However, further study is warranted in order to understand the additional benefits offered by the newer group of antidiabetic agents and their impact on healthcare utilization and costs. out of the total, 1,965 hospital-visited patients were identified to be receiving either SGLT-2 (n= 306), GLP- 1 (n=392), or DPP-4 (n=819). Unadjusted total all-cause average inpatient visit and outpatient visits were significantly lower with the SGLT-2 cohort (1.64; p= 0.05 and 5.52; p<0.01, respectively). However, unadjusted total health, inpatient, and prescription expenditures were significantly higher among the GLP-1 cohort ($24,924,
$6,162, and $12,066, respectively; p<0.0001). After adjusting, total health expenditure keeping SGLT-2 as a reference, with every unit increase in GLP-1 and DPP-4 prescription, health expenditure increased in a significant manner by $0.1371 and decreased by $0.2235 respectively, whereas the prescription expenditure was significantly lower in the DPP-4 ( = -0.3342; p= 0.02) compared to SGLT-2. However, there were no significant differences in the emergency and inpatient visits between the three cohorts after adjusting for the socioeconomic factors. The study concluded that the patient on SGLT-2 therapy experienced a minimum number of hospital visits in comparison to other drugs and GLP-1 cohort was associated with higher total health expenditure. [22].
MATERIALS AND METHODOLOGY
RESULTS
Gender wise distribution of Prescription: -
Table 1: Gender wise distribution of Prescription
|
Gender |
Frequency |
Percentage |
|
Female |
109 |
54.5% |
|
Male |
91 |
45.5% |
|
Total |
200 |
100.0% |
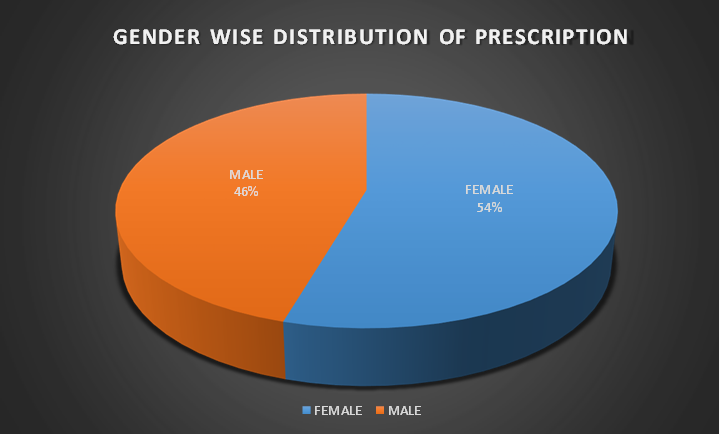
Figure 1: Gender wise distribution of Prescription
Age wise distribution of Prescription: -
Table 2: Age wise distribution of Prescription
|
Age Group |
Frequency |
Percentage |
|
<40 |
18 |
9.0% |
|
40-49 |
26 |
13.0% |
|
50-59 |
75 |
37.5% |
|
60-69 |
54 |
27.0% |
|
≥70 |
27 |
13.5% |
|
Total |
200 |
100.0% |
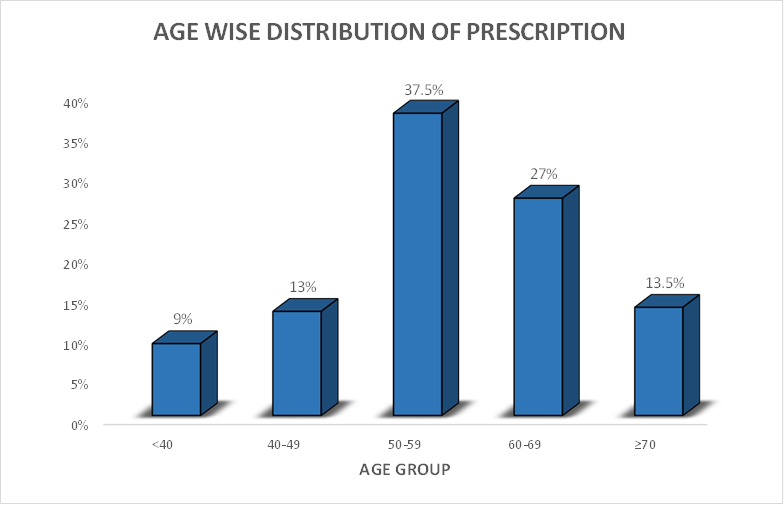
Figure 2: Age wise distribution of Prescription
Prescription Frequency of Individual Drug Classes:
Table 3: Frequency of individual drug classes
|
Drug Class |
Frequency |
Percentage |
|
|
1. |
Insulin |
45 |
43.26% |
|
2. |
Sulfonylureas |
9 |
8.65% |
|
3. |
Thiazolidinediones |
3 |
2.88% |
|
4. |
Α – GLUCOSIDASE INHIBITORS |
2 |
1.92% |
|
5. |
Dpp-4 Inhibitors |
21 |
20.19% |
|
6. |
Sglt2 Inhibitors |
24 |
23.07% |
Figure 3: Frequency of individual drug classes
Frequency Analysis of Multi-Drug Combinations:
Table 4: Frequency of multi-drugs combination
|
Drug Class |
Frequency |
Percentage |
|
|
1. |
Sulfonylureas+Biguanides |
36 |
17.64% |
|
2. |
Dpp-4 Inhibitors+ Biguanides |
29 |
14.21% |
|
3. |
Α–Glucosidase Inhibitors+Biguanides |
2 |
0.98% |
|
4. |
Α–Glucosidase Inhibitors+Sglt2 Inhibitors |
3 |
1.47% |
|
5. |
Sglt2 Inhibitors+Dpp-4 Inhibitors |
61 |
29.90% |
|
6. |
Thiazolidinedione+Dpp-4 Inhibitors |
2 |
0.98% |
|
7. |
Sulfonylureas+Thiozolidinedione+Biguanide |
4 |
1.96% |
|
8. |
Α–Glucosidase Inhibitors+Biguanides+Sulfonylureas |
11 |
5.39% |
|
9. |
Sglt2 Inhibitors+Sulfonylureas+Biguanides |
3 |
1.47% |
|
10. |
Sglt2 Inhibitors+Dpp-4 Inhibitors+Biguanides |
53 |
25.98% |
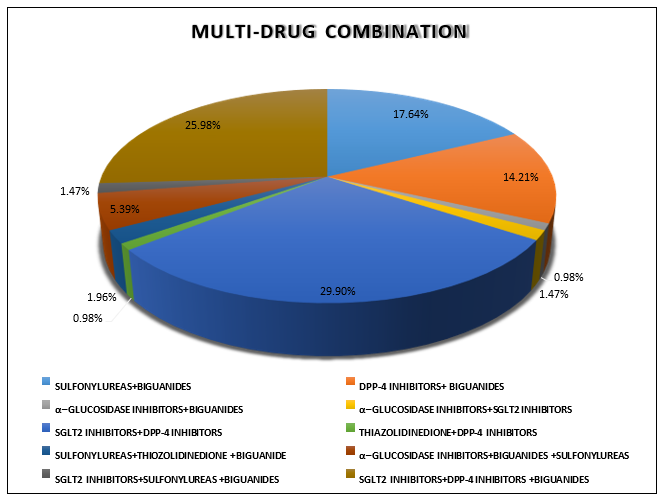
Figure 4: Frequency of multi-drugs combination
Pharmacoeconomics of Insulin:
Table 5: Pharmacoeconomics of Insulin
|
Brand name |
Cartridge (3ml) price(Rs) |
Flexpen price(Rs) |
|
Lantus |
640 |
769 |
|
Humalog |
900 |
1017 |
|
Novomix |
937 |
1042 |
|
Xsulin |
310 |
560 |
|
Ryzodeg |
1126 |
1450 |
|
Human Actrapid |
386 |
569 |
|
Basugine |
594 |
999 |
|
Mixtard 30HM |
386 |
569 |
|
Nobeglar 100IU |
571 |
685 |
|
Fiasp 100IU |
740 |
914 |
|
Basaglar 100IU |
640 |
769 |
Pharmacoeconomics of drugs belong to Sulfonylureas:
Table 6: Pharmacoeconomics of Sulfonylureas
|
Drug |
Brand name |
Price (Rs) |
|
Glimepiride |
Geminor (2mg) |
65[10S] |
|
Euglim(2mg) |
97[15S] |
|
|
Adglim(1mg) |
36[10S] |
|
|
Azulix(2mg) |
65[10S] |
|
|
Glynamic(1mg) |
37[10S] |
|
|
Gliclazide |
Glizid(40mg) |
36[10S] |
|
Diamicron XR (60mg) |
280[15S] |
|
|
Cyblex SR (30mg) |
146[15S] |
|
|
Pioglitazone |
Pioglar (15mg) |
76[10S] |
|
Glimepiride+Metformin |
Geminor M1 |
147[15S] |
|
Gluconorm G1 |
225[15S] |
|
|
Gemer 1 |
149[15S] |
|
|
Switglim M |
63[15S] |
|
|
Adglim M2Forte |
95[10S] |
|
|
Diapride M1 |
136[15S] |
|
|
Gliclazide+Metformin |
Prizide M 80 |
139[15S] |
|
Glycinorm M 40 |
130[15S] |
|
|
Cyblex M(40mg) |
120[15S] |
Pharmacoeconomics of drugs belong to SGLT2 inhibitors:
Table 7: Pharmacoeconomics of SGLT2 inhibitors
|
Drug |
Brand Name |
Price (Rs) |
|
Dapagliflozin |
Dapamac 10 |
164[10S] |
|
Oxra(10mg) |
217[14S] |
|
|
Dapefy 10 |
217[14S] |
|
|
Udapa 10 |
141[10S] |
|
|
Dapagliflozin+Metformin |
Dapavel M |
159[10S] |
|
Dapaglyn M |
229[15S] |
|
|
Daplo M5 |
149[10S] |
|
|
Glucreta M5 |
112[10S] |
|
|
Dapagliflozin+Sitagliptin +Metformin |
Dapamac trio(500mg) |
187[10S] |
Pharmacoeconomics of drugs belong to DPP-4 inhibitors:
Table 8: Pharmacoeconomics of DPP4 inhibitors
|
Drug |
Brand name |
Price (Rs) |
|
Sitagliptin |
Sitadoc(100mg) |
270[15S] |
|
Istavel(100mg) |
142[10S] |
|
|
Emsita(100mg) |
165[10S] |
|
|
Sitared 100 |
142[10S] |
|
|
Vildagliptin |
Verifica SR 100 |
194[10S] |
|
Gluvilda OD 100 |
120[10S] |
|
|
Vitaglo OD 100 |
142[10S] |
|
|
Linagliptin+Metformin |
Ondero met |
149[10S] |
|
Linanext M |
111[10S] |
|
|
Linares M |
110[10S] |
|
|
Sitagliptin+Dapagliflozin |
Macsita D |
169[10S] |
|
Sitagliptin+Metformin |
Istamet |
156[15S] |
|
Sitadoc M |
210[15S] |
|
|
Vildagliptin+Metformin |
Vilact M(1000mg) |
83[10S] |
|
Glipy met 500 |
149[15S] |
|
|
Zomelis met |
179[15S] |
|
|
Zavamet 1000 |
129[10S] |
Patient demographics
As, Table: 1, shows that among 200 patients, 109 (54.5%), were females and 91 (45.5%) were males.
Age distribution
Age wise distribution geriatric patients were more. As Table 2 shows that 37.5% of the patients were in the age group of 50-59 and less percentage is seen in age group of less than 40 (9%).
Frequency of individual class drug
From this study, around 43.26%of the patients were taking insulin, followed by (23.07%) SGLT-2 Inhibitors, DPP-4 Inhibitors (20.19%), sulfonylureas (8.65%) and rest of the drugs having lesser percentage in individual class drug, as shown in figure- 3
Frequency of multi-drug combination
From this study, around 29.9% of the patients were taking (SGLT-2 Inhibitors +DPP4 Inhibitors), followed by SGLT-2 Inhibitors +DPP-4 Inhibitors+Biguanides (25.98%), sulfonylureas+Biguanides (17.64%) and rest of the drug having lesser percentage in combination multi drug class, as shown in figure-4.
Pharmacoeconomics:
Pharmacoeconomics of Insulin
From this study, Xsulin and Human Actrapid is the least expensive options among them Ryzodeg is the most expensive option which might limit its use. Flexpens are generally more expensive than cartridge. As shown in Table-5.
Pharmacoeconomics of sulfonylurea
From this study, Glimepiride: Adglim (1mg), Glynamic (1mg) are the cheapest option among them, Gliclazide:Glizid (40mg) is also affordable. Diamicron XR (60mg) is the most expensive among them. In combination, Gluconorm G1 is the most expensive among them while, Switglim M is the least expensive option. As shown in Table-6
Pharmacoeconomics of SGLT-2 Inhibitors
From this study, Udapa (10mg, Rs 141) and Glucreta MS (Rs112) are the most affordable option in individual and combination class of drug. IN combination, Dapaglyn M (Rs229) is the most expensive option among them. And in individual Oxra (10mg) and Dapefy 10 (both Rs 217) is the most expensive option among them. The most prescribed drug is Dapamac trio (Rs187). As shown in Table-7.
Pharmacoeconomics of DPP-4 Inhibitors
From the study, Istavel (100mg) and Sitared 100 mg (both Rs 142) are the cheapest option among them. Gluvilda OD (100mg, Rs120) and Vilact M (100mg, Rs83) are the cost-effective option. In combination Linares M and Linanext M is the least expensive option among them while, Sitadoc M (Rs200) is the most expensive option, as shown in Table-8.
DISCUSSION
In this study a total of 200 prescriptions of diabetic patients were analysed after taking their consent. Majority of the patients were in this were females (54.5%), while males were (45.5%). The study focused on the patients aged between 20 to 80 years. Patients in the age group of 50-59 years have more diabetic disease as compared to other age groups population. Geriatric patients have more diabetic problems as compared to other age group population.
The most commonly utilized antidiabetic medication was Insulin in individual classes of drug while in multi-drug combinations, most commonly used antidiabetic medication is SGLT-2 Inhibitors +DPP-4 Inhibitors.
In combination therapy sulfonylureas and biguanides (eg: metformin) were frequently used medication for the control of hypoglycaemia. The use of metformin as a first line therapy was well documented while sulfonylureas also offer some additional glycaemic control.
From the pharmacoeconomic study of Insulin, Xsulin and Human Actrapid brand was the least expensive option among them. While Ryzodeg was the most expensive brand option. It was observed that Flexpens was more expensive than Cartridges.
The pharmacoeconomic study of sulfonylureas, for individual class of drug saw that Glimepiride (Adglim, Glynamic) was the cheapest among them. In Gliclazide (Glizid) was also affordable. While in combination class of drug Gluconorm G1 was the most expensive and Switglin M was the least expensive brand as compared to other.
The pharmacoeconomic study of DPP-4 Inhibitors, for individual class of the drugs Istavel was the cheapest option in Vildagliptin, Sitadoc was the expensive among Vildagliptin. In combination drug Zomelis met was the most expensive in Sitagliptin
+Metformin, while Sitadoc M was the most expensive in Sitagliptin+Metformin. Linares M and Linanext M was the least expensive in combination.
The pharmacoeconomic study of SGLT-2 Inhibitors, for individual class of drug, Udapa 10 was the least expensive as compared to Oxra and Dapefy 10 that was more expensive. In combination class of drug Dapaglyn M was the most expensive as compared to the other Glucreta M5 which was the least expensive in the combination of Dapagliflozin +Metformin.
The use of combination therapy enhances the importance of patient education and adherence. Further study must be done to investigate adherence rates among patient to identify the barriers and develop the strategies to improve management.
CONCLUSION
The examination of prescription trends and the pharmacoeconomic implications of antidiabetic medications in a tertiary care setting underscores the critical intersection of clinical efficacy and economic sustainability in diabetes management. As the prevalence of diabetes continues to rise globally, the demand for effective treatment options has intensified, leading to an evolving landscape of antidiabetic medications. This analysis reveals that while newer classes of medications, such as SGLT2 inhibitors and DPP-4 inhibitor, demonstrate significant benefits in terms of glycaemic control and cardiovascular outcomes, their higher acquisition costs pose challenges for healthcare systems.
Prescription trends indicate a marked shift towards these newer agents, driven by their favourable safety profiles and additional therapeutic benefits. However, this trend raises concerns regarding the overall affordability and accessibility of diabetes care, particularly in resource-limited settings. The need for a balanced approach is evident, as healthcare providers must consider not only the clinical effectiveness of these medications but also their economic implications for both patients and healthcare systems.
Pharmacoeconomic analysis play a crucial role in informing prescribing practices. By evaluating the total cost of treatment, including medication costs, hospitalisations, and complications related to diabetes, healthcare professionals can make informed decisions that align with both patient needs and economic realities. This necessitates a shift toward value-based care, where the focus is on achieving the best health outcomes at the lowest possible costs.
Moreover, the integration of pharmacoeconomic data into clinical guidelines can facilitate more rational prescribing practices. Educational initiatives aimed at healthcare providers can further enhance understanding of cost-effectiveness, empowering them to choose therapies that provide optimal outcomes without compromising financial sustainability.
Future research is essential to continue evaluating the long-term pharmacoeconomic impact of antidiabetic medications, particularly as new therapies emerge. Real-world evidence studies can provide insights into the effectiveness and cost implications of these medications in diverse populations, informing better healthcare policy and practice.
In summary, the interplay between prescription trends and pharmacoeconomic considerations in antidiabetic medication underscores the need for a multifaceted approach to diabetes management. By prioritising both clinical outcomes and economic viability, stakeholders can improve the quality of care for individuals with diabetes while ensuring the responsible use of healthcare resources. This holistic perspective will be vital in shaping future diabetes management strategies in tertiary care settings and beyond.
REFERENCES





Jiji K.*, Dayami Satya, Shubham Raj, Soham Das, Soumyadip Guchhait, Prescription Trends and Pharmacoeconomic Implications of Anti-Diabetic Medications in a Tertiary Care Setting, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 575-596 https://doi.org/10.5281/zenodo.17529133
 10.5281/zenodo.17529133
10.5281/zenodo.17529133
