Department of Pharmaceutics, Bengal School of Technology, Sugandha, Delhi Road, Hooghly-712102, West Bengal, India.
Among the various routes of administration, oral route is the most suitable and convenient. Drug actions can be improved by developing new oral drug delivery systems such as mucoadhesive buccal drug delivery system. The oral cavity is an ideal site for drug delivery, bypassing intestinal degradation and first pass hepatic metabolism. Mucoadhesion can be defined as a state in which two components, of which one is of biological origin are held together for extended periods of time by the help of interfacial forces mucoadhesion is the attachment of the drug along with a suitable carrier to the mucous membrane. Mucosal surfaces benefit to drug molecules not to amenable to the oral route. Mucoadhesive dosage forms provide prolonged retention at the site of application and providing a controlled drug relese for enhanced therapeutic effects. Mucoadhesion is a complex phenomenon which involves wetting, adsorption and interpenetration of polymer chains. Many researchers are working on the investigations of the interfacial phenomena of mucoadhesion with the mucus. Mucoadhesion is currently explained by six theories which are electronic, adsorption, wettability, diffusion and mechanical. Buccal mucosa’s accessibility and immobility make it ideal for retentive dosage forms. The aim of this review is the mechanisms and theories involved in mucoadhesion.
Buccal drug administration is most common route for drug delivery. Buccal mucosal delivery offers several advantages, including: it is patient friendly, has the ease of self medication, allows for a flexible and controlled dosing schedule in comparison to most other drug delivery system. However, it has following demerits together with hepatic first pass metabolism and enzymatic degradation within the gastro intestinal tract, the restrict oral administration of certain classes of the drugs mainly peptides and proteins. Consequently, different absorptive mucosa is taken into consideration as potential sites for drug administration [1]. Buccal drug delivery involves administration drugs through the mucous membranes in mouth. The different transmucosal route, buccal mucosa has first- rate accessibility, an expanse of smotth muscle and generally stationary mucosa, hence appropriate for administration of retentive dosage forms [2]. Transmucosal drug delivey through rectal, vaginal, ocular nasal and oral cavities offers advantages over traditional systemic administration methods. These advantages includes rapid drug loss, avoidance of presystemic elimination within the GI tract and depending on the particular drug, a beneficial gut microbes for absorption [3]. Oral mucosal cavity drug delivery falls into two main categories: (a) sublingual delivery (b) buccal delivery. Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces.
Bioadhesion And Mucoadhesion
Bioadhesion describe adhesion between any biological and synthetic surface. Adhesion occurring in a biological setting is termed “bioadhesion”. Bioadhesion is defined as the state in which two materials, at least one biological in nature, are held together for extended period of time by internal forces. In bioadhesive drug delivery the term bioadhesion refers to the bonding between biodegradable polymer and soft tissues, such as intestinal mucosa [4]. Mucoadhesion describe the particular interaction of a mucosal membrane with a synthetic surface. In general, bioadhesion is a term which includes adhesive interactions with any biological or biologically derived substance, and mucoadhesion is used when the bond is formed with a mucosal surface [5].
Mechanism Of Mucoadhesion
Mucoadhesion involves attaching drugs to mucous membranes using suitable carrier. Mucoadhesion has the following mechanism:
The Residence time for mucosal routes is typically in a minute or less than an hour [7].
Theories Of Mucoadhesion
Wetting Theory Of Mucoadhesion
The wetting theory applied to liquid or low viscosity bioadhesives. The wetting theory was developed predominantly in regard to liquid adhesives, uses interfacial tension to predict spreading and in turn adhesion. The wetting theory calculates contact angles and the thermodynamic work of adhesion [8].
The contact angle (Q) ideally zero for optimal spreading is linked to interfacial tensions(g) as per the Youngs eqation,
Gtg = gbt + gbg COS Q
Where t, g and b represent tissue, gastrointestinal contents and bioadhesive polymer.
The spreading coefficient, Sb/t can be given by,
Sb/t= gtg - gbt - gbg
For the bioadhesion to take place the spreading coefficient should be positive. It gives advantages to maximize the interfacial tension at the tissue GI- contents interface and minimizing the surface tension at the other two interfaces [9].
Electrostatic Theory Of Mucoadhesion
This theory is based on both mucoadhesive and biological materials posses opposite electrical charges. When these materials come into contact with each other, they transfer the electrons leading to formation of double electronic layer at the interface, where attractive forces within this layer determines the mucoadhesive strength [10].
Fracture Theory Of Adhesion This theory based on mechanical measurement of mucoadhesion [11]. It gives relation between the forces required for detachment of polymers from the mucus and strength of their adhesive bond. The work fracture is greater when the network strands are longer or the degree of cross – linking is reduced [12].
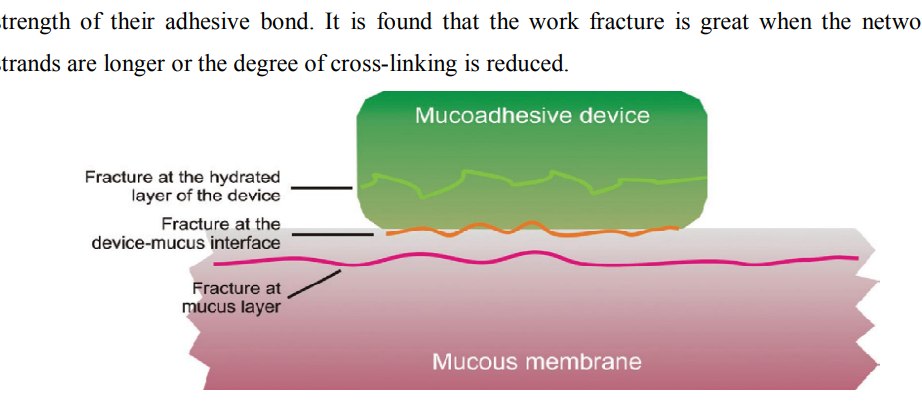
Figure 1: Regions where the mucoadhesive bond ruptures can occur.
Adsorption Theory Of Mucoadhesion
After initial contact, surface adhere due to surface forces between their chemical structure. When polar molecules or groups are present, they reorientate at the interface. The properties of polymer decide the formation of chemical bond [13].
Diffusion Theory
According to this theory mucin and polymer chain penetrates each other to sufficient depth to create a semi permanent adhesive bond [14,15]. The degree of penetrate depends on diffusion coefficient, flexibility and nature of mucoadhesive chains, mobility and contact time of polymer chain. The depth of interpenetration required to produce an efficient bioadhesive bond lies in range 0.2-0.5 µm [16].
Factor Affecting Mucoadhesion In The Oral Cavity
Mucoadhesion Depends On Bioadhesive Polymer And Medium In Which The Polymer Will Reside [17]. The Various Factor Affect Mucoadhesive Properties Of Polymers Such As Molecular Weight, Flexibility, Hydrogen Bonding capacity, cross linking density, charge concentration and swelling of polymer [18].
Polymer related factor
Molecular weight:
Maximum bioadhesion occurs at an optical molecular weight. Bioadhesion strength of polymer increase with molecular weight up to 100,000 and beyond this level there is no significant effect on bioadhesive strength [19]. Size and configuration of polymer are important.
Concentration of active polymer:
When the concentration of polymer is low, the interaction between polymer and mucus is unstable. More concentration of polymer would result in longer penetrating chain length and better adhesion [20,21].
Flexibility of polymer chains:
Bioadhesion starts with diffusion of polymer chains in the internal region. Polymer chains require substantial flexibility in order to achieve the desired entanglement with the mucus [22]. The mobility and flexibility of polymer are related to their viscosity and diffusion coefficients. Cross linking in water soluble polymer reduces the mobility of polymer chains [23].
pH:
pH was found to exert a significant effect on mucoadhesion [24]. pH of medium is determinant factor for degree of hydration of highly cross linked polyacrylic acid polymers and it will be increases between pH 4-5 and decreases more at alkaline pH [25].
Swelling:
Hydrogen is necessary for mucoadhesive polymer to expand and create a proper macromolecular mesh of sufficient size and also induce mobility in polymer chains to enhance interpenetration process between polymer and mucin [26]. Polymer swelling exposes the bioadhesive sites for hydrogen bonding, thus permits mechanical entanglement [27].
Physiological variables
Mucin turnover rate:
The natural turnover of mucin molecules from mucus layer is important because the mucin turnover is expected to limit the residence time of mucoadhesive on the mucus layer and the mucin turnover results in substantial amount of soluble mucin molecules. These molecules interact with mucoadhesive before they interact with mucus layer [28].
Disease state:
During the disease conditions such as common cold, gastric ulcer, bacterial and fungal infections of female reproductive tract the physiochemical properties of mucus changes [29]. Mucoadhesive properties of delivery system should be checked under these condition [30].
Advantages Of Oral Mucoadhesive Drug Delivery
Limitation Of Buccal Drug Delivery:
Buccal Drug Delivery System:
Drug delivery via membranes of oral cavity can be subdivided as follows:
Basic Components Of Buccal Drug Delivery
Permeability:
The oral mucosae in general are somewhat leaky epithelia intermediate between that of the epidermis and intestinal mucosa. It is estimated that the permeability of buccal mucosa is 4-4000 times greater than that of the skin. Substances that facilitate the permeation through buccal mucosa are called permeation enhancer [37].
List of compounds used as oral mucosal permeation enhancers [37]
|
Permeation Enhancer(Siegel IA et al., 1981) |
|
23- lauryl ether |
|
Aprotinin |
|
Azone |
|
Benzalkonium chloride |
|
Cetylpyridinium chloride |
|
Cetyltrimethylammonium bromide |
|
cyclodextrin |
|
Dextran sulfate |
|
Lauric acid |
|
Lysophosphatidylcholine |
|
Menthol |
|
Oleic acid |
|
Sodium EDTA |
Drug substance:
Before formulating buccoadhesive drug delivery system, the intended release duration (rapid/prolonged) and effect (local/systemic) must be determined. The selection of suitable drug for the design of buccoadhesive drug delivery system should be based on pK properties.
Characteristics of drug substance:
Buccoadhesive polymer [38]
|
Criteria |
Categories |
Example |
|
Source |
Natural Synthetic |
Agarose, Chitosan, Gelatin, Gums(Guar, xanthan, pectin) Cellulose derivatives: CMC, HEC, HPc, HPMC Polyacrylic acid derivative: CP, PC, PAA, Polymethacrylate Other: PVA, PVP, Thiolated polymer. |
|
Aqueous solubility |
Water soluble
Water Insoluble |
CP, HEC, HPC, HPMC, PAA, Sodium CMC. Chitosan, EC, PC |
|
Charge |
Cationic Anionic Non-ionic |
Aminodextran, chitosan EDTA, CP, CMC, PAA, Pectin Hydroxyethyl starch, HPC, PVA. |
|
Potential bioadhesive forces |
Covalent Hydrogen Electrostatic interaction |
Cyanoacrylate. Acrylates, methacrylic acid, CO, PC, PVA Chitosan |
Characteristics of an ideal mucoadhesive polymer:
Backing membrane [37]:
Backing membrane plays very important role in attachment of bioadhesive devices to the mucus membrane. The material used as backing membrane should be inert, and impermeable to the drug and penetration enhancer. Commonly used materials in backing membrane are carbopol, magnesium stearate, HPMC, HPC,CMC.
Buccal Route Of Drug Absorption:
For drug transport across oral mucosa there are 2 permeation pathways: paracellular and transcellular routes. Permeants can utilize both routes simultaneously, but one route is typically favored based on the diffusant’s physiochemical properties. Lipophilic compounds have poor solubility in hydrophilic environments like intercellular spaces and cytoplasm. The cell membrane’s lipophilic nature hinders hydrophilic compounds, while intercellular spaces impede lipophilic compound, due to their respective partition coefficient [39].
Buccal Formulation [40] :
Types Of Buccal Formulation [41] :
Buccal Tablets:
Buccal Patches And Films:
Buccal patch made of two or multi layered of thin film round or oval as consisting of bioadhesive polymeric layer and impermeable backing layer to provide unidirectional flow of drug across bucccal ,mucosa.
Example:Isosorbide dinitrate in the form of unidirectional erodible buccal film are developed and characterized for improving bioavailability.
Buccal Semisolid Dosage Forms:
A semisolid dosage form consist of finely powdered natural or synthetis polymer dispersed in a polyethylene or in aqueous solution.
Example: gels, ointment
Gels are usually clear, transparent , semisolids containing solubilized active substances.
Buccal Powder Dosage Forms:
Buccal bioadhesive powder dosage forms are mixture of bioadhesive polymers and drug which are spread onto the buccal mucosa. A significance increase in residence time relative to oral solutions was observed.
CONCLUSION:
Mucoadhesive buccal drug delivery is a promising area with the aim of systemic delivery of orally inefficient drug as well as a feasible and attractive for non- invasive delivery of potent peptide and protein drug molecules [42]. The various advantages of oral mucoadhesive drug delivery system like prolongation of residence time of the drug which in turn increases the absorption of the drug are important factors in the oral bioavailability of many drugs [43]. The factors which are determinant in the success of the mucoadhesive drug delivery are polymer physiochemical properties and the in vivo factor such as mucin turnover rate, mucin flow [44]. The buccal mucosa is a promising delivery route for drugs that need to avoid the gastrointestinal tract due to degradation by the gastric pH, intestinal enzymes or due to a substantial hepatic first pass effect [45].
REFERENCES



Anandamoy Rudra*, Archita Sadhukhan, Arindam Dutta, Mucoadhesive Buccal Drug Delivery: A Review, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 782-790. https://doi.org/10.5281/zenodo.14305298
 10.5281/zenodo.14305298
10.5281/zenodo.14305298
