Clinical Pharmacologist, KLE-HCG Suchirayu Hospital Hubballi.
The antifolate and antimetabolite medication methotrexate is used for its anti-inflammatory and immunosuppressive effects. In addition to some cancers including leukaemia and lymphoma, it is frequently recommended for autoimmune conditions like psoriasis and rheumatoid arthritis. Methotrexate functions by blocking the enzyme dihydrofolate reductase, which is necessary for DNA synthesis and cell division. This is especially true for cells that divide quickly. This case involves a 74-year-old woman who was taking methotrexate and developed methotrexate-induced neutropenia, a rare but dangerous side effect brought on by accidental use or dosage mistakes. If neutropenia—characterized by dangerously low neutrophil levels—is not identified and treated quickly, it can result in infections that are potentially fatal. In clinical pharmacy practice, this example emphasises the significance of patient education and accurate dose, as well as the clinical ramifications of methotrexate toxicity.
A folic acid antagonist called methotrexate is a key drug used to treat a number of autoimmune conditions, including psoriasis, rheumatoid arthritis, and several types of cancer, including acute lymphoblastic leukaemia. It works by inhibiting dihydrofolate reductase, which impairs DNA synthesis, especially in cells that divide quickly. Although methotrexate is usually well tolerated at low dosages, there are a number of side effects linked to its use, such as hepatotoxicity, gastrointestinal issues, and haematologic toxicity[1].Patients may be at risk for serious infections due to neutropenia, a less frequent but potentially fatal side effect of methotrexate treatment. Direct bone marrow suppression or a build-up of toxic methotrexate levels can cause neutropenia, especially in patients with genetic predispositions, medication interactions, or renal impairment. Neutropenia brought on by methotrexate may predispose[2] Neutropenia brought on by methotrexate may lead to systemic problems like sepsis and put patients at risk for serious infections like bronchopneumonia. The risk of methotrexate toxicity and associated effects may be increased by specific concomitant disorders. The drug's clearance may be hampered by acute kidney injury (AKI), which could result in higher serum levels and greater toxicity. Clinical results may deteriorate if anaemia further impairs the body's defences against infections. Furthermore, RA-ILD presents a special difficulty since it makes patients more susceptible to pulmonary infections, which might be made worse by immunosuppression brought on by neutropenia[3] .
Case Presentation: A 74 year old female patient presented with chief complaints of inability to consume food and shortness of breath since 3 days . She is a known case of Rheumatoid arthritis (RA) since 8 years.. She was previously admitted to the hospital for the treatment and management of bilateral bronchopneumonia, anaemia, sepsis,Acute kidney injury (AKI) and RA associated interstitial lung disease(ILD). She has oral mucositis, which prevents her from eating. The patient had been taking methotrexate without realising it even after being told to discontinue . Upon inspection, the respiratory system r/s is b/l AE+, the respiratory rate is 24, and the SPO2 is 92%. Haematocrit (HCT, PCV): 32.8%; haemoglobin: 10.5 g/dl; RBC: 3.54 10^6/uL; neutrophils: 0.0%; WBCs: 0.98 10^6/uL. According to biochemistry studies, procalcitonin is 0.98 ng/mL and creatinine is 1.28 mg/dL. A peripheral smear analysis revealed normocytic normochromic anaemia accompanied by thrombocytopenia and leukopenia. The quantity of platelets decreased (81 10^/uL). C-reactive protine(CRP) levels were 90mg/dl. 2D echo scans were normal.HRCT -Chest – plain reports showed a. Nonspecific inyerstitial pneumoniae b. Patchy consolidations in apical segments of B/L upper lobes – Bronchopneumonia c. Mild pulmonary Hypotension . She was started on Noradrenaline for hypotension. The patient was also prescribed a 50 mg pill of Leucovorin Calcium to counteract the effects of methotrexate and a 0.1% oral gel of Triamcinolone and Candid mouth paint for oral mucositis. During her stay in the hospital she was put on Inj Meropenam 2GM, INJ LINID 500MG( both for neutropenic sepsis), NEB Ipratropium Bromide &Levosalbutamol,Neb Budecort, Tab Oseltamivir Phosphate 75mg And Syrup Lactulose.
|
Table 1 Laboratory investigations of the patient |
|
|
|
|
Test description |
Results |
Unit |
Reference interval |
|
HB |
10.5 |
g/dL |
|
|
RBC |
3.54 |
10^6/?L |
3.8-4.8 |
|
WBC |
0.98 |
10^9/?L |
4.0-10.0 |
|
Neutrophils |
0.0 |
% |
40-80 |
|
Platelets |
81 |
10^3/?L |
150-410 |
|
PCV |
32.8 |
% |
36-46 |
|
Creatinine |
1.28 |
mg/dL |
0.66-1.25 |
|
Procalcitonin |
0.98 |
ng/mL |
0.074-0.101 |
|
CRP |
90 |
Mg/dL |
0-6.0 |
CBC- complete blood count ;RBC- red blood cells ;WBC –white blood cells; PCV- packed cell volume ; CRP-C- reactive protein
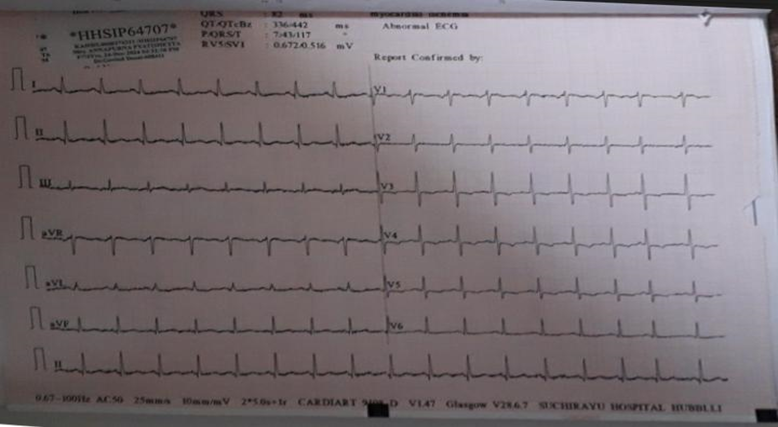
ECG- Abnormal (Myocardial Ischemia)
DISCUSSION: An essential component of the therapy of autoimmune disorders, ectopic pregnancies, and some types of cancer is methotrexate (MTX), a folate antagonist. The main way it works is by blocking the enzyme dihydrofolate reductase (DHFR), which is essential for the production of tetrahydrofolate. DNA replication and nucleotide production depend on tetrahydrofolate, especially in cells that divide quickly[4] .Although it can also impact healthy cells that divide quickly, such as bone marrow's haematopoietic progenitor cells, this cytotoxic effect is therapeutic when it comes to malignant or hyperactive immune cells.[5])Because methotrexate affects bone marrow suppression, neutropenia is a serious side effect.[6]The following steps are part of the pathophysiology: 1. Inhibition of Folate Metabolism: By competitively inhibiting DHFR, methotrexate lowers tetrahydrofolate levels, which hinders the production of purines and thymidines. 2. Disruption of DNA Synthesis: Insufficient nucleotides cause DNA replication to halt, especially in the bone marrow's proliferative haematopoietic stem cells. 3. Myelosuppression: When the bone marrow is suppressed, less neutrophils are produced (granulopoiesis), which results in neutropenia[7] High doses, renal impairment (which delays drug clearance), concurrent use of medications such as proton pump inhibitors or NSAIDs (which interfere with renal excretion), and genetic polymorphisms in the enzymes involved in folate metabolism are risk factors for methotrexate-induced neutropenia[8]In extreme situations, poor medication excretion exacerbates methotrexate toxicity. Increased drug accumulation brought on by renal failure intensifies the cytotoxic effects of the medication[9] .Furthermore, the decreased availability of folate further exhausts stores required for DNA recovery and repair. Fever, infection susceptibility, and other indications of bone marrow suppression are frequently seen in the clinical presentation of methotrexate-induced neutropenia. Treatment include stopping methotrexate right away, giving folinic acid (leucovorin) to save healthy cells by avoiding DHFR inhibition, and providing supportive care such as granulocyte colony-stimulating factors (G-CSFs) or antibiotics [10].Preventing and reducing this side effect requires knowledge of methotrexate's pharmacokinetics and pharmacodynamics as well as patient-specific risk factors. Adequate dose modifications and careful monitoring of renal function and total blood counts are essential to ensuring patient safety[11]
CONCLUSION: This case highlights the potentially severe complication of methotrexate-induced neutropenia in patients with comorbid conditions such as RA-associated interstitial lung disease, acute kidney injury, and anemia. The inadvertent continued use of methotrexate despite contraindications underscores the critical need for patient education, awareness, and regular follow-up. Early recognition and management, including prompt discontinuation of methotrexate, administration of leucovorin calcium, and supportive care with antibiotics and granulocyte colony-stimulating factors, are essential to prevent life-threatening consequences.Furthermore, this case emphasizes the crucial role of pharmacists in preventing such adverse events through active intervention. Pharmacists can play a pivotal role in educating patients about proper medication use, monitoring for potential drug interactions, and providing counseling on the risks of methotrexate toxicity. Increased awareness among healthcare providers and patients, coupled with pharmacist-led interventions, can significantly reduce the likelihood of medication errors and improve overall patient safety.
REFRENCES



Mithila Sreeramoju*, Dr. Aishwarya Suresh Pattanshetti, Dr. Govind Desai, Methotrexate Induced Neutropenia: A Case Report, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 646-649. https://doi.org/10.5281/zenodo.14995506
 10.5281/zenodo.14995506
10.5281/zenodo.14995506
