Department of Pharmacy, Mahatma Jyotiba Phule Rohilkhand University, Bareilly, Uttar Pradesh, India 243006
Potential methods for primary disease prevention have been identified as a result of a better understanding of the mechanisms behind endometrial carcinogenesis; however, a prospective assessment of their effectiveness in clinical trials is still pending. Invasive endometrial sampling has historically been necessary for the diagnosis of endometrial cancer, which is linked to a higher survival rate. The use of cytology and protein and DNA biomarkers in new, minimally invasive tests has the potential to revolutionize diagnostic processes and enable the monitoring of high- risk groups. Decisions for adjuvant treatment are increasingly being guided by the molecular classification of endometrial malignancies, which demonstrated therapeutic utility in addition to a prognostic influence. Increasing the use of targeted therapies, especially immunotherapy, and debulking surgery has also transformed the management of advanced and recurrent diseases. In addition to summarizing recent developments in endometrial cancer prevention, diagnosis, and therapy, this review aims to pinpoint areas that require further investigation.[1,29] In women, ovarian torsion is an uncommon but serious disorder. To maintain the function of the ovaries and tubes and avoid serious morbidity, early detection is essential. Complete or partial rotation of the adnexal supporting organ with ischemia is referred to be ovarian torsion. Females of various ages can be affected. About 2% to 15% of patients who have surgical therapy for adnexal masses experience ovarian torsion. An ovarian mass is the primary risk factor for ovarian torsion. Acute pelvic discomfort, followed by nausea and vomiting, is the most typical sign of ovarian torsion. Information on ovarian cysts can be obtained through pelvic ultrasonography.The mainstay of diagnosis and therapy for suspected ovarian torsion is either surgery or detorsion.
The most common gynecologic malignancy that almost all gynecologists encounter is endometrial carcinoma. Having a solid grasp of the epidemiology, pathophysiology, diagnostic, and treatment options for this type of cancer allows obstetrician-gynecologists to identify women who are at higher risk, assist in lowering risk, and encourage early identification. illness that arises in the tissue lining the uterus, the small, pitiful organ in a woman's pelvis where a fetus develops. Most endometrial cancers are adenocarcinomas, or tumors that originate in cells that secrete and leak mucus and other fluids.[9] Endometrial carcinoma is the most common type of cancer that affects the organs of the female reproductive system. In Europe, one to two out of every 100 women will get endometrial cancer in the future. In the European Union, endometrial cancer is diagnosed in about 88,000 women annually. in the great majority of countries throughout Europe. It is the sixth most common cause of cancer-related mortality among women in Western Europe. Endometrial cancer usually affects women over 50 after menopause, while up to 25% of cases may occur before menopause. About 75% of women receive a stage I uterine cancer diagnosis. These women have a good prognosis with a 90% 5-year.

Fig 1. Schematic representation of Uterine Anatomy
Advances in Endometrial Cancer Prevention:
Because of its substantial association with modifiable risk factors, endometrial cancer appears to be well suited for primary disease prevention; modeling suggests that up to 60% of endometrial cancer cases may be prevented.[2,80,86]. A greater understanding of the mechanisms causing endometrial carcinogenesis, specifically unopposed estrogen, insulin resistance, and chronic inflammation, has led to the proposal of several interventions aimed at reducing the incidence of endometrial cancer, though data on their efficacy is primarily limited to retrospective observational studies.
Controlling Weight:
Obesity has the strongest association with endometrial cancer among the twenty most common tumor types, accounting for around 34% of diagnoses. However, because weight loss improves insulin sensitivity, decreases inflammation, and reduces adiposity and the aromatase-induced conversion of androgens into estrogen, it is associated with a lower risk of endometrial cancer. The Women's Health Initiative found that intentional weight loss of as little as 5% bodyweight over a three-year period is associated with a 39% (95%CI 12–58%) reduction in the risk of endometrial cancer. Interestingly, weight loss was most beneficial for obese women (HR 0.44, 95%CI 0.25–0.78), but it was also beneficial for women with a normal BMI (HR 0.61, 95%CI 0.27– 1.38). Although altering one's lifestyle can help one lose weight, it can be challenging to maintain and raise the chance of weight cycling, which appears to be more detrimental to the risk of endometrial cancer than maintaining a higher weight [13,19,21]. It is undeniable that most women cannot jog seven hours a week, which is required to reduce the risk of endometrial cancer by 10%. As a result, the focus has shifted to newly created anti-obesity medications (AOMs), which appear to offer more significant and sustainable weight loss than lifestyle modifications and previously established AOMs like orlistat. Glucagon-like peptide 1 (GLP- 1) agonists, such as semaglutide and liraglutide, increase insulin sensitivity, delay stomach emptying, and decrease appetite. The mean weight loss at two years was −15.2% when weekly semaglutide was taken in conjunction with a behavioral intervention in a STEP 5 RCT, whereas the mean weight change with a placebo was −2.6% (p < 0.0001). 51.8% of participants in a SCALE RCT lost at least 5% of their body weight, while 24% of those who received a placebo did the same (p < 0.0001). This implies that ligarglutide works just as well. The side effects include atrioventricular blockage, skin reactions, gastrointestinal upset, and occasionally, pancreatitis; long-term tolerance and safety have not yet been established[19,20,22].
Chemoprevention of Hormones:
Oral contraceptives have been shown to reduce the risk of endometrial cancer by 24% for every five years of use, a benefit that has been demonstrated for the past 20 years. Importantly, this effect appears to persist for up to 30 years after stopping intake. [3,23,24] Although oestrogen-containing preparations are not recommended for women with a BMI > 35 kg/m2 due to an increased risk of arterial and venous thrombotic events, the international consensus group recommends the combined oral contraceptive pill for women with Lynch syndrome who require contraception because of its positive effects on the risks of both ovarian and endometrial cancer. Even though irregular bleeding often results in higher dropout rates, progestin- only contraception is also likely to be effective. The levonorgestrel-releasing intrauterine system (LNG-IUS) may be the best method of preventing endometrial cancer, based on a number of observational studies. It has been demonstrated that long-term use of the device can lower the risk of endometrial cancer by up to 78%. It seems to reduce endometrial development even in women with a BMI of 40 kg/m2, and modeling suggests that it could be a financially feasible primary disease prevention method for high-risk women.[4,25,81] It is encouraging that a new meta- analysis did not confirm the earlier worries of a higher risk of postmenopausal breast cancer associated with the use of LNG-IUS. To ascertain whether the LNG-IUS is both efficacious in lowering the risk of endometrial cancer and sufficiently preferred by women for routine usage, adequately powered clinical trials are now necessary. It has been reported that long term consumption of following drugs prevents the endometrial cancer.
Aspirin:
Aspirin, a cycloxyengase-2 inhibitor, reduces estrogen and aromatase levels, induces apoptosis, and has anti-inflammatory effects. Long-term aspirin use may be a more effective strategy for obese women (relative risk reduction 20–44%), but it may only marginally reduce the incidence of endometrial cancer in women in the general population (8–11%). The RCT was not adequately powered to assess the benefit to women in terms of the risk of endometrial cancer, but the CAPP2 analysis shown that regular aspirin use in individuals with Lynch syndrome clearly reduced the risk of colorectal cancer. However, the results were encouraging (hazard ratio 0.50, 95% CI 0.22–1.11) and call for more investigation.
Metformin:
There has been a lot of interest in using the insulin-sensitizer metformin and the oral biguanide for the treatment of endometrial cancer. Despite initial promising results in single- arm studies, metformin did not appear to reduce endometrial proliferation when examined in a more methodologically sound RCT. These results were confirmed by a Cochrane research that found insufficient evidence to support the use of metformin either by itself or in combination with progestin therapy to treat endometrial hyperplasia..[5] As the authors noted, only two trials with a combined total of 59 patients were appropriate for inclusion in their study, making it difficult to draw conclusions that may be applied to other situations.[15] A meta-analysis of six trials demonstrated that metformin use was not associated with a lower risk of endometrial cancer, even after adjusting for the confounding variable of diabetes (odds ratio 1.05, 95%CI 0.82–1.35). In addition to demonstrating that adding metformin to the LNG- IUS did not increase its effectiveness in treating early-stage endometrial cancer, a recently published feMMe study also demonstrated the low cytostatic effect of metformin on the endometrium. Collectively, these results should discourage researchers from utilizing metformin as a chemotherapeutic treatment for endometrial cancer.[26,27,30]
EPIDEMIOLOGY AND RISK FACTORS :
Estrogens have been implicated in the genesis of endometrial cancer in a number of epidemiological investigations. Long-term, unopposed estrogenic action, whether endogenous or exogenous, has been proposed as the etiology of endometrial cancer due to its high connection with women who have an intact uterus. Endometrial cells go through more mitosis when estrogens are not countered, which raises the risk of somatic mutations and errors in DNA replication.[6,71,72,75] These changes manifest clinically as hyperplasia and malignancy.Nonetheless, the carcinogenic effect of estrogen on the endometrium is largely offset by the effects of progesterone. Genetic factors, which account for less than 5% of endometrial cancers (such as Lynch syndrome due to a mutation in the mismatch repair gene and hereditary non- polyposis colorectal cancer), and previous pelvic irradiation are additional risk factors. Table 1 shows the endometrial cancer risk in relation to epidemiological risk variable .
Table 1: Relative risk of developing carcinoma endometrium with some epidemiological risk factors
|
|
Risk Factor |
Relative Risk |
|
A |
Prolonged estrogen exposure |
|
|
|
Estrogen-only hormonal therapy |
02-Oct |
|
|
Early menarche |
1.5-2 |
|
|
Late menopause |
02-Mar |
|
|
Nulliparity |
2 |
|
|
Anovulation (Polycystic Ovarian Syndrome) |
3 |
|
B |
Demographic Characteristics |
|
|
|
increasing age (> 55 years) |
1.4 |
|
|
High socioeconomic status |
1.3 |
|
|
Family history of uterine malignancy (Lynch syndrome) |
22-50% life time risk |
|
C |
Diabetes mellitus |
2 |
|
D |
D. Obesity |
2.4 |
|
|
For type I endometrial cancer |
|
|
|
BMI 25.0 to 30 kg/m2 |
OR 1.5 |
|
|
BMI 30.0 to 39.9 kg/m2 |
OR 2.5-4.5 |
|
|
BMI ≥40.0 kg/m2 |
OR 7.1 |
|
|
For type II endometrial cancer: |
|
|
|
BMI 25.0 to 30 kg/m2 |
OR 1.2 |
|
|
BMI 30.0 to 39.9 kg/m2 |
OR 1.7-2.2 |
|
|
BMI ≥40.0 kg/m2 |
OR 3 |
|
E |
Hypertension |
1.5 |
|
F |
Prior pelvic RT |
8 |
|
G |
Tamoxifen |
2 |
Types of Histopathology:
The most prevalent histological form of endometrial cancer is endometrioid adenocarcinoma. In 1983, Bokhman identified two separate varieties, each with a unique occurrence, clinical presentation, molecular pattern, and biological behavior. [7,8,26,27]
Type 1 Endometrial Carcinoma
Type 1 endometrial cancers account for 80% of uterine carcinomas. These tumors react to estrogen and are present in premenopausal or perimenopausal age groups.They are frequently well-differentiated and have an endometrioid histology. Type 1 endometrial carcinomas are usually linked to extended and unopposed estrogen exposure, as seen in women with obesity, anovulatory cycles, infertility, and estrogen-secreting tumors. These tumors frequently have a favorable prognosis, with a 5-year survival rate of >90%. These people have K-RAS mutations, microsatellite instability, PTEN, PiK3CA, and K-RAS overexpression. [28,29,30]

Fig 2. Endometrial Cancer
Type 2 Endometrial Carcinoma
The remaining 10–20% of cases are type 2 endometrial malignancies. They typically develop in an atrophic endometrial context and are estrogen independent. They affect older, postmenopausal, multiparous, non-obese, tamoxifen-using, and smoking women. Serous, clear cell, mucinous, squamous, and grade 3 endometrioid adenocarcinoma are among the histological forms.[8,31,32,55] These are aggressive cancers that frequently exhibit extrauterine dissemination and profound myometrial invasion. With a 50% chance of recurrence and a 35% overall survival (OS), type 2 tumors have a worse prognosis. They are linked to genetic changes in the expression of HER2/neu, p53, and E-cadherin.
Molecular typing: Next-generation sequencing has revealed four molecular subtypes of endometrial cancer.The four endometrial cancer categories proposed by the Cancer Genome Atlas (TCGA) in the ProMisE project showed a new, repeatable technique of diagnosing endometrial cancer that went beyond histological criteria, despite the fact that it was not cost- effective.Testing is now possible thanks to immunohistochemistry (iHC)-based surrogate typing for endometrial cancer. [33,34,57] Based on somatic copy number alteration (CAN), somatic mutation number, and MSI status, endometrial cancer can be classified into four groups.The ultra-mutated phenotype of POLE mutations, which is linked to extremely positive clinical consequences
The instability of microsatellites (MSI)
CN low copy-number
A high copy-number (CN high)
There are limitations to the iHC-based classification. Endometrioid grade 3 is found in nearly all four subtypes, although clear cell carcinomas are not found in any of them. Therefore, before the relevance is fully acknowledged, more information regarding the outcomes of patients treated based on molecular subtypes must be gathered and the primary areas of decision making are still unaddressed.[35,40,44]
FIGO STAGING OF ENDOMETRIAL CANCER :
Stage-I
There are major changes to Stage I in the 2023 updated FIGO staging system. Generally speaking, Stage I is restricted to uterine corpus-confined cancers that exhibit aggressive histological types without myometrial invasion, non-aggressive histological types (such as low-grade EEC), or the lack of substantial/extensive LVSI. Low-grade EECs and other tumors of non-aggressive histological kinds that are limited to the endometrium are classified as Stage IA1 tumors, whereas Stage IA2 tumors are those that involve up to 50% of the myometrium and do not have focal LVSI or LLVSI. Stage IA3 tumors are low-grade endometrioid carcinomas that are limited to the uterus and have concurrent low-grade endometrioid ovarian involvement if the following criteria are met: 1) no significant or extensive LVSI; 2) no superficial myometrial invasion (<50%); 3) no further metastases; and 4) unilateral ovarian tumors that are limited to the ovary and do not rupture or infiltrate thecapsule (similar to pT1a). Stage IB tumors, also referred to as low-grade EECs, are non-aggressive histological types with at least 50% myometrial invasion and limited or localized LVSI. Stage IC cancers are aggressive tumor types that are either limited to the endometrium without myometrial invasion or contained within a polyp. Evidence-based reasoning was used in the creation of these categories. Endometrial carcinomas limited to the endometrium or endometrial polyps (regardless of histological subtype) are associated with a favorable prognosis. A staging action is necessary in order to create this category. A significant portion (≥40%) of high grade tumors, particularly serous carcinomas, that are believed to be limited to the endometrium or a polyp actually involve occult lymph nodes and/or the peritoneum when appropriately graded, making them Stage III illnesses.[39,40,48] Low-grade EECs that are limited to the uterine corpus and do not exhibit localized or LVSI are associated with a favorable prognosis. Low-grade endometrioid carcinomas affecting both the ovaries and the endometrium are associated with a favorable outcome in a subgroup of patients . Previously categorized as totally distinct tumors, molecular research has revealed that these cancers share a shared clonal source. The lack of LVSI and focused LVSI have been associated with a better prognosis than significant/extensive LVSI in low-grade EECs restricted to the uterus. WHO recommendations are followed in the LVSI requirements [3,51,58,60]. Therefore, LVSI should be categorized as "LVSI substantial/extensive" (more than five vessels), "LVSI focal" (less than five vessels), or "LVSI negative" (less than five vessels).
Stage II
Stage II has undergone significant adjustments as part of the updated staging system. The new staging approach will result in a significant increase in the number of women with Stage II malignancies. Non-aggressive histopathological tumors with cervical stromal invasion are classified as stage IIA tumors. According to the WHO 2021 report, stage IIB now includes instances with non-aggressive histological types and significant LVSI, irrespective of local tumor dissemination.[5,52,53] There is a large corpus of literature that supports these findings. LVSI has been repeatedly demonstrated to be a strong and independent predictor of endometrial cancer recurrence in large database series, prospective cohort studies, randomized trials, and single- institution reports.[9] According to a retrospective registry study of more than 1,500 patients from Sweden with Stage I–III endometrioid adenocarcinomas, LVSI is the strongest independent risk factor for lymph node metastases and poor survival, even in cases when lymph node metastases are absent. Stage IIC tumors are aggressive histological forms with any myometrial involvement, whereas Stage IC malignancies are aggressive histological types without myometrial involvement. Aggressive histological forms include gastrointestinal-type mucinous endometrial carcinomas, carcinosarcomas, mesonephric-like carcinomas, serous adenocarcinomas, clear cell adenocarcinomas, high-grade endometrioid, and undifferentiated carcinomas. Aggressive histological types are consistently associated with a much higher likelihood of relapse, according to retrospective reports, large database series, prospective cohort studies, and randomized trials. Combining genetic and clinicopathological factors enhances risk assessment for endometrial cancer in its early stages, according to numerous research.
Stage III
By Stage III, the tumor has either spread locally or regionally. By more properly portraying the clinical picture and prognosis, the new subclassifications are meant to aid in a more appropriate treatment decision-making process. An overview of the modifications made from the prior staging system is provided below. Stage IIIA differentiates between uterine serosa infiltration (IIIA2) and adnexal (IIIA1) infiltration to more accurately indicate tumor activity, especially in high-grade and nonendometrioid carcinomas. Second, Stage IIIB now consists of two substages. Similar to the earlier Stage IIIB sickness, Stage IIIB1 involve the vagina and/or the parametria. Involvement of the pelvic peritoneum is now classified as IIIB2 (previous Stage IV) to better reflect clinical treatment decisions regarding the justification for surgery versus non-surgical first-line treatments for patients with advanced stage illness.[10] These treatment options vary significantly between cases of confined pelvic carcinomatosis and situations of extensive/extrapelvic peritoneal carcinomatosis. The pelvic anatomical landmark is the line that joins the anterior superior iliac spines. Third, solitary tumor cells are not viewed as metastatic and are instead regarded as pN0(i+). Micrometastases (IIIC1i, IIIC2i) and macrometastases to the lymph nodes (IIIC1ii, IIIC2ii) are further split into stage IIIC. Substaging is based on the improved prognosis for patients with lymph node micrometastases.[18,61,67] This subcategorization also reflects the increasing use of sentinel lymph node technique and ultrastaging, which allow for better detection of small volume sickness, including micrometastasis. It is permissible to surgically define the illness as Stage III rather than Stage IV based on the upper limit of the para-aortic lymph node metastases to the renal vessels bilaterally. Finally, because they show evidence of clonal connections and have a usually good prognosis, low-grade EECs that involve both the ovary and the endometrium and fit specific criteria are now classified as Stage IA3 tumors instead of Stage III.[65,67,73] In some cases, no adjuvant treatment is recommended. Stage IA3 does not include cases with more than 50% myometrial invasion, capsule breech, severe LVSI, adnexal involvement, bilateral ovarian involvement, or further metastatic lesions. These cases are still in Stage III and require adjuvant treatment as previously.
Stage IV
The establishment of a new substage, currently known as Stage IVB, for patients who present with extrapelvic peritoneal metastases is the main change made to this area of the FIGO staging system. Stage IIIB2, which is for patients whose peritoneal involvement does not extend beyond the pelvis, is distinct from this substage. Local invasion of the bladder mucosa and/or intestinal/bowel mucosa is still in Stage IVA, but distant metastases, such as to any extra- abdominal lymph nodes or intra-abdominal lymph nodes above the renal arteries to the lungs, liver, brain, or bone, have advanced to Stage IVC. Peritoneal carcinomatosis is relatively rare, occurring in about 2% of patients with endometrial carcinomas. It is important to distinguish those who have distant metastases from those who have this condition.[3,69,73,76]
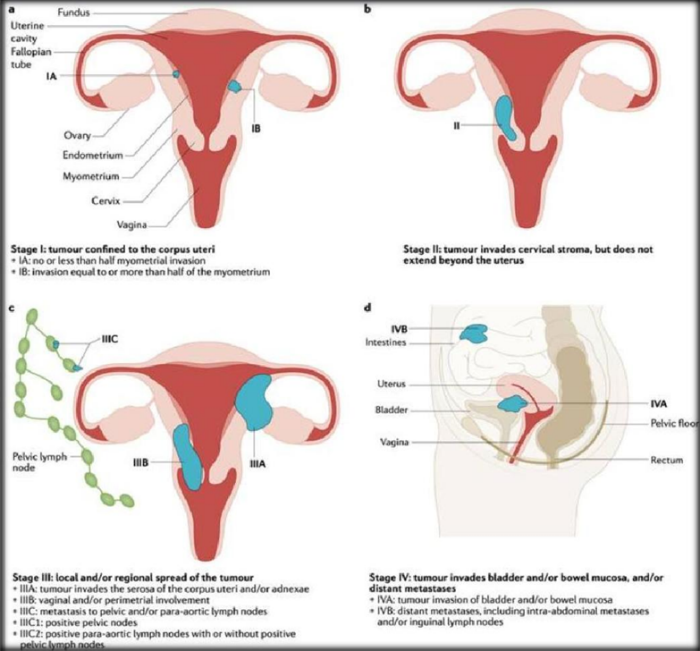
Fig 3. A tumor that is limited to the corpus uteri (Stage I; panel a), invades the cervical stroma but remains confined to the uterus (Stage II; panel b), spreads locally and/or regionally (Stage III; panel c), and invades the bladder and/or bowel mucosa and/or distant metastases (Stage IV; panel d) are the four stages that make up this staging system.
MEDICAL ASPECTS :
While older women usually present with postmenopausal bleeding, younger women usually present with atypical uterine bleeding. The risk of endometrial cancer is approximately 10% for women who experience postmenopausal bleeding. Rarely, asymptomatic women could be diagnosed with infertility.[11,74,78,79] The prior menstrual history may reveal a history of early menarche, late menopause, or irregular periods during the perimenopausal transition.Clinical indicators of severe disease include ascites-induced abdominal distention, constipation, pain, lower extremity lymphedema, hemoptysis, coughing, jaundice, and/or rectalor urine bleeding. A history of diabetes, hypertension, hormone usage, or tamoxifen use may be present. Investigating any family history of uterine, colorectal, or genitourinary cancer is crucial, especially if endometrial cancer is detected before the age of fifty. In addition to a general physical examination that includes assessment of breast and supraclavicular and inguinal lymph node enlargement, uterine size and mobility, and involvement of the cervix, parametrium, lateral pelvic wall, bladder, or rectum, a thorough systemic and gynecological examination (per speculum, per vaginum, and bimanual pelvic examination) is necessary.[12,83,86]
DIAGNOSTIC WORKUP:
Transvaginal sonography (TVS) - Transvaginal sonography (TVS) is the first-line imaging modality utilized to triage these symptomatic patients in order to assess uterine size, endometrial thickness, endo-myometrial interface, myometrial echotexture, and adnexa. Additional testing is necessary for postmenopausal women with endometrial thickness greater than 4 mm, perimenopausal women with intermenstrual bleeding or persistent heavy bleeding, and premenopausal women with anovulatory cycles. Tamoxifen users may experience thickening of the endometrium due to subendometrial cysts. Polyps, endometrial hyperplasia, and the buildup of fluid, blood, or pus are some causes of thicker endometrium. Endometrial and endocervical sampling - A fine Karman's cannula (4 mm) or an endometrial biopsy using endometrial aspiration tools like Pipelle can supply sufficient tissue for histopathology. With an aspiration device, postmenopausal women can detect cancer up to 91– 99% more accurately than premenopausal women. Endocervical curettage must be performed before endometrial aspiration in any situation when endometrial cancer is suspected. Colposcopy, endocervical, and endometrial assessment should also be performed on asymptomatic women with aberrant glandular cells (AGC) on cytology.[9] Dilatation and curettage - Following an office endometrial sample that reveals cancer, routine dilatation and curettage (D&C) is not necessary. Hysteroscopy - Women with negative or insufficient sampling and a high suspicion of cancer are recommended to have additional assessment with hysteroscopy. The following are the indications for directed biopsy and hysteroscopy TVS abnormalities accompanied by negative biopsy The uterine cavity is inaccessible, and even after a negative endometrial aspiration biopsy, women with high risk continue to have symptoms. [12] Endometrial polyps that can be removed at the same time can be diagnosed by hysteroscopy. Transtubal migration of tumor cells following hysteroscopy has raised concerns since it could be identified by cytology as malignant pelvic washings. Although there is noticeable peritoneal spillage during hysteroscopy, it is unclear what the outcome means.Numerous investigations have revealed a higher percentage of positive cytology (30% vs. 12%), but the result (disease- specific survival or recurrence) remained same. According to Kudela et al., the proportion of positive peritoneal cytology following hysteroscopy is same to that following D&C.
APPENDIX A: Systemic Therapy
|
Multi-agent Chemotherapy |
Single-agent IV Therapy |
Hormonal Therapy |
Maintenance Therapy |
|
H/dMMR tumors) |
|
|
TREATMENT:
Surgery is the mainstay of treatment. Adjuvant* therapies are those that are used in conjunction to surgery, such as chemotherapy* and radiotherapy. Each of the following treatments has advantages, disadvantages, and contraindications. To be aware of the treatment's effects, it is advised to consult a doctor about the anticipated dangers and advantages of each procedure. There are multiple treatment options available for certain people, and the decision should be made after weighing the risks and anticipated benefits.[13]
Surgery
Each patient undergoes a preoperative evaluation. Five to ten percent of individuals with endometrial cancer may not be able to have surgery because of medical restrictions and the dangers of anesthesia. This is typically brought on by illnesses including diabetes, heart disease, and obesity. The purpose of surgery for individuals deemed operable is to remove the tumor-containing uterus and stage the disease. Staging the disease - Surgery will enable the disease to be staged. This is accomplished by examining the tumor to determine its size, location, and whether tumor cells are present in the ovaries, cervix, ovarian tubes, lymph nodes, or other parts of the pelvic and abdomen. The liver, diaphragm, omentum, and peritoneal surfaces are among the other abdominal organs that surgeons examine and feel during the procedure. In order to look for cancer cells, surgeons also inject liquid into the abdominal cavity, extract it with suction, and Send it to a lab. We refer to this as peritoneal cleaning. Every tissue that is extracted during the procedure is sent to the lab for a pathologist's inspection (histopathological examination). Removing the tumor -The uterus containing the tumor will be removed . The uterus, two ovarian tubes, and two ovaries are removed during the procedure. A hysterectomy is the removal of the uterus, while a bilateral salpingo-oophorectomy , also known as a bilateral salpingo- ovariectomy, is the removal of both ovarian tubes and both ovaries. Patients with stage I, stage II, and stage III cancer may undergo this procedure by laparoscopically assisted vaginal hysterectomy or by making an incision in the lower abdomen (laparotomy). This method guides the evacuation of the uterus, ovarian tubes, and ovaries through the vagina by projecting and enlarging the image on a television screen using a video camera. This latter method has been demonstrated to shorten hospital stays, decrease the need for painkillers, lower the rate of post-operative complications, and enhance quality of life when compared to laparotomy. [14] It also appears to yield comparable outcomes in terms of tumor removal quality and survival. Several lymph nodes in the pelvis and along the aorta may be removed - It may be necessary to remove the lymph nodes along the aorta and in the pelvic region. Hospitals differ in this practice. There is no proof that removing lymph nodes* improves the accuracy of determining the cancer's stage or that it offers any further benefits for curing the disease or preventing its recurrence. The disease known as lymphoedema, in which lymph fluid builds up in the legs, is more likely to occur if the lymph nodes are removed. Nonetheless, it aids in identifying individuals who could require adjuvant medicines and is a component of the staging process. Many surgeons recommend that all patients undergo surgery have their lymph nodes removed, with the exception of those who have a stage IA tumor and a grade 1 or 2 tumor.
Adjuvant therapy
There is no conclusive evidence to support the routine use of adjuvant treatment for patients with disease confined to the uterus (localized endometrial cancers). [15] For all stages, there is still debate and unclear evidence regarding the best options. It is advised that the choice of endometrial cancer treatment be made by an inter-disciplinary team of medical professionals. An adjuvant therapy is a therapy administered in addition to surgery.[18,25,77] This meeting of multiple doctors is called a multidisciplinary meeting or tumor board review. In this meeting, the planning of therapy is discussed according to the essential information mentioned above.
Adjuvant treatment for stage I cancer -
Observation: It involves routine medical consultations that include a physical examination, a vaginal examination, and history taking (a review of the patient's medical history).[2,65] If signs or symptoms are observed, additional testing, including a radiological examination, blood tests, and an examination under anesthesia may be performed.
Adjuvant vaginal brachytherapy : which is an internal type of radiotherapy where the source of radiation is placed in the vagina.
Adjuvant pelvic radiotherapy : as an external form of radiotherapy, in which radiation is generated from an outside source and then sent to the pelvis.
Adjuvant chemotherapy : which is the use of anticancer drugs to kill cancer cells or limit their growth. It is not clear which combination of drugs are the most effective but they should include one drug containing platinum (cisplatin and carboplatin are platinum containing drugs used in the treatment of endometrial cancer). [16,84,86] For patients with stage I cancers, the choice of the treatment after surgery mainly depends on the risk of recurrence. For patients with low risk of recurrence (stage IA and grade 1-2 tumor), observation is recommended.
Adjuvant treatment for stage II cancer –
Adjuvant vaginal brachytherapy : This is a form of internal radiotherapy in which the vagina serves as the radiation source.
Adjuvant pelvic radiotherapy : which is an external type of radiotherapy where radiations are produced by an external source and then directed to the pelvis
Adjuvant chemotherapy : It involves using anticancer medications to either eradicate or stop the proliferation of cancer cells. Although the best medicine combination is unknown, they should include one platinum-containing medication (cisplatin and carboplatin are platinum-containing medications used to treat endometrial cancer).
Only patients with grade 1-2 tumors that do not have lymphovascular invasion and whose lymph nodes have been excised and are tumor cell-free based on histological analysis are eligible for vaginal brachytherapy. [17] When the lymph nodes have not been checked for tumor cells during the surgery, vaginal brachytherapy and pelvic radiation are recommended. Adjuvant chemotherapy as well as pelvic radiation may be considered. Adjuvant chemotherapy may reduce the risk of "metastasis," or the spread of cancer outside the pelvis, also known as extra-pelvic recurrence. They should include a platinum-containing medication combination, even if the optimal combinations are unclear (cisplatin and carboplatin are platinum). include drugs for the treatment of endometrial cancer.
Treatment of advanced disease (stage III and IV) –
Chemotherapy, radiation, and surgery are usually used to treat advanced endometrial cancer. Five to ten percent of patients with advanced endometrial cancer will not be able to have surgery due to medical limitations. In addition to internal radiotherapy, also referred to as brachytherapy, which includes introducing a radiation source into the uterus or vaginal cavity, and/or external radiotherapy, which involves directing radiation from an external source to the tumor, these patients may also get systemic treatment.
Adjuvant therapy for stage III cancer –
Previously, patients with stage III cancer were recommended to have pelvic radiotherapy* and vaginal brachytherapy after surgery. There is growing evidence that chemotherapy, either in place of or in addition to radiation therapy, is recommended for patients with stage III disease. The optimal course of action should be discussed with doctors. Adjuvant chemotherapy should include one platinum-containing drug (cisplatin and carboplatin are platinum-containing drugs used to treat endometrial cancer). It's crucial to keep in mind that adjuvant radiation, both internal and external, stops local tumor regrowth (in the pelvis). The disease cannot spread outside the pelvis thanks to chemotherapy.
Adjuvant therapy for stage IV cancer –
The goal of treatment for patients with stage IV endometrial cancer is to target cancer cells that have metastasized, or spread, to other regions of the body, such as the pelvis, after cytoreductive surgery. Locally, postoperative radiation therapy prevents the recurrence of pelvic malignancies. A systemic treatment targets cancer cells all across the body, not only in specific places. Examples of systemic treatment include chemotherapy and hormone therapy. Chemotherapy drugs include anthracyclines, taxanes, and platinum-based compounds. For patients with advanced endometrial cancer, paclitaxel-based combination regimens are advised for first-line chemotherapy due to their proven effectiveness and tolerance. It is only appropriate to employ hormonal therapy for endometrioid histologies. It involves taking drugs that include the progesterone hormone. Tamoxifen and aromatase inhibitors are other drugs that are also being used. Treatments for patients with advanced endometrial cancer should be customized to meet their unique requirements, health, and prognosis.Side effects of adjuvant therapies : After therapy, the most common adverse effects of adjuvant therapies are typically reversible. A variety of these adverse effects can be avoided or alleviated using proper tactics. Doctors should be informed up front about this.
Pelvic radiotherapy :
The main source of side effects from external radiotherapy used to treat endometrial cancer is the irradiation of the organs around the uterus. Radiation exposure can result in bladder spasms that create an urgent desire to urinate, blood in the urine, ulceration or necrosis of the mucous membrane lining the bladder, obstruction of the urinary system, and painful urination. Rectal discomfort, diarrhea, mucus and blood rectal discharge, and, in rare cases, intestinal perforation are all consequences of radiation exposure to the lower digestive system. Another potential side effect of pelvic radiation is vaginal constriction. The oncologist should provide treatment recommendations for these post-radiation responses. The goal of contemporary external radiotherapy* techniques like intensity modulated radiation therapy (IMRT) is to lessen the toxicity of the treatment. [5,35,45]
Intravaginal brachytherapy : Although less common, the previously noted adverse effects of external radiation can also manifest with intravaginal brachytherapy due to its superior targeting. During and after the procedure, vaginal dryness is common. Long-term sexual dysfunction may also arise from vaginal dryness and constriction. Radiation therapy reduces ovarian function in young women, which might lead to more vaginal dryness and sexual dysfunction. Additionally, it may increase the risk of osteoporosis and/or pelvic bone insufficiency fractures. For these issues, women need to be treated by a specialist.[17,73,75]
Chemotherapy: Chemotherapy side effects are common. They will be determined by the drug or drugs used, the dosages, and personal circumstances. You should take certain precautions and/or modify your treatment if you have previously experienced other issues, such as heart issues. Generally speaking, using multiple medications causes more side effects than using just one. The most frequent side effects of the drugs used for chemotherapy in endometrial cancer are hair loss and a decreased blood cell count. A low blood cell count can cause infections, bleeding, and anemia. After the chemotherapy is finished, the blood cell count returns to normal and the hair grows back.Other typical adverse effects consist of: • Allergy symptoms, such as redness and flushing • Peripheral neuropathy, a nerve disorder that affects the hands and/or feet and can result in pain, numbness, and/or tingling sensations on the skin • transient visual loss or hearing changes,diarrhea, vomiting, and low blood pressure; inflammation of the mouth lining and other areas ; loss of taste; lack of appetite; and a sluggish heartbeat , dehydration, minor skin and nail abnormalities that go away quickly, excruciating swelling and inflammation where the injection is administered, and discomfort in the muscles or joints , Seizures and fatigue . There may be other, less common, but more dangerous adverse effects. These include, in particular, myocardial infarction, stroke, and impairment of liver and renal function. You should consult a physician if you have any of these symptoms. [4,86] In addition to these, every medication may have other adverse effects. Although not everyone will experience side effects or to the same degree, the most prevalent ones are listed below.
Hormonal therapy: There are several adverse effects linked to hormone therapy. They can range from minor issues like headaches, nausea, and/or breast soreness to more serious ones like abnormal vaginal bleeding, heart difficulties, stroke, blood clots in the lungs (pulmonary embolus), or blood clots in the legs (deep vein thrombosis)
B . Ovarian Torsion
Introduction:
Females of all ages can experience ovarian torsion, which is a gynecological emergency. It describes ischemia alterations in the ovary caused by a full or partial rotation of the adnexal supporting organ. The ovary and fallopian tube are more frequently involved in torsions, while isolated torsion involving just one of them occurs less frequently (one in 1.5 million women). There have also been reports of torsion involving paratubal or paraovarian cysts. In order to safeguard ovarian and tubal function and avoid serious morbidity, early diagnosis and surgery are crucial.

Fig 4. Schematic representation of an Ovarian Cyst vs a Normal uterus
Ovarian Cyst :
A fluid-filled sac that forms on or inside an ovary is called an ovarian cyst. The majority are benign (not malignant) and frequently disappear on their own. Many of them are asymptomatic, and they are somewhat prevalent, particularly in women of reproductive age.[55]
Symptoms:

Fig 5. Ovarian Cyst
Utero ovarian and infundibulo pelvic ligaments:
The ovary can move laterally or posteriorly to the uterus thanks to the infundibulopelvic ligaments, which suspend it. Along the infundibulopelvic ligaments, which connect to the pelvic sidewall, the ovarian vessels pass.[56,58,70] Twisting can be caused by a large leading point, like tumorous development, because adnexal tissue is not fixed. The utero- ovarian (UO) ligament connects the opposite side of the ovary to the uterus. Muscle and fibrous tissue make up the UO ligament. In addition to supporting and connecting the ovary to the uterus, the UO ligament also transports blood from the uterine artery to the ovary.
Pathogenesis :
When an ovarian tumor or cyst develops, it causes ovarian torsion, which rotates the UO ligament as well as the infundibulopelvic ligament. Usually, the mass or cyst is a benign lesion that is larger than 5 cm. However, normal ovaries can also undergo torsion, especially in premenarchal girls with extended infundibulopelvic ligaments.[26,42,49] However, as premenarchal girls reach puberty, the ligament shortens, which may reduce the incidence of ovarian torsion.

Fig 6. Development of ovarian torsion
The study of epidemiology :
According to a 10-year analysis of 128 patients with adnexal torsion, ovarian torsion was present in 2.7% of cases requiring emergency surgery.[54,68,78] 15% of 135 patients with surgically treated adnexal tumors experienced torsion, according to another 10-year research. Ovarian torsion occurred in around 2% to 15% of individuals who underwent surgery to remove adnexal tumors. Premenarchal girls and postmenopausal women are less likely to experience ovarian torsion (17.2% of cases), which primarily affects those in the reproductive age range.
Risk elements :
The main risk factor for ovarian torsion is an ovarian mass, since over 80% of individuals with the condition had ovarian masses that were 5 cm or bigger. The risk of torsion is connected with the sizes of ovarian masses.[64,77,79] Although it can happen with any size mass, ovarian torsion has been documented to happen with masses ranging from 1 to 30 cm (mean 9.5 cm). Multiple big ovarian follicular cysts may result from ovulation inducement used to treat infertility; these large cysts have a higher risk of torsion.
In the premenarchal population :
Ovarian torsion is more frequently associated with a normal ovary in premenarchal girls than in older women . Over half of children with torsion under the age of 15 have healthy ovaries . Compared to patients with aberrant adnexa, more patients with normal adnexa (7/11) experienced torsion.
Torsion of the ovaries during pregnancy :
Pregnancy-related ovarian torsion was between 10% and 22% . Ovarian masses greater than 4 cm are more common between weeks 10 and 17 of pregnancy.The incidence of torsion was 1%–6% lower in pregnant women with adnexal masses 4 cm or larger than in nonpregnant women.
Clinical Presentation :
On clinical presentation, ovarian torsion brought on by an adnexal tumor manifests as a variety of symptoms and indicators. Lower abdomen pain with an abrupt start, followed by nausea and vomiting, is the most typical symptom. Waves of nausea, with or without vomiting, are experienced by certain patients.Abdominal discomfort typically starts suddenly and goes on and off. Up to 210 days following the onset of symptoms, the majority of reported patients arrived for evaluation one day or later. Due to their inability to pinpoint the exact location of their discomfort, premenarchal individuals frequently reported widespread pain. The adnexal torsion was thought to be the cause of the uncomfortable symptoms and indicators. Some people have experienced ovarian torsion without an infectious illness, which causes a low-grade temperature.[5,34,65,79]
Evaluation and diagnosis :
A patient's medical history and physical examination are the first steps taken when they present clinically. Any recent diagnoses of an adnexal mass, persistent stomach pain, and low-grade fever should be included in the medical history. A pelvic mass or pain should be looked for during the physical examination.[45,58] A hematocrit, white blood cell count, electrolyte panel, and serum human chorionic gonadotropin should all be part of the laboratory assessment. Adnexal torsion cannot be diagnosed with a serum marker. An adnexal tumor type may be indicated by a number of blood markers. An ovarian germ cell tumor or pregnancy can be detected by serum human chronic gonadotropin. CA-125 could be a sign of endometrioma or a cancerous ovarian tumor. Some studies have established an association between an increased level of serum interleukin-6 and ovarian torsion , while further research such as oxidative stress during ovarian torsion is needed .

Fig 7. Ovarian Torsion Diagnosis
Imaging studies are the most important for evaluating a pelvic mass . The first-line diagnostic test is ultrasonography. Due to edema or vascular and lymph engorgement, a torn ovary may appear rounder and larger than the contralateral ovary. The components, location, density, Doppler flow, and size of an ovarian tumor can all be easily distinguished by ultrasonography. There can be reduced or absent Doppler flow in the vessels of a torsed ovary . Doppler flow has a high sensitivity and specificity, according to one prospective study. In the diagnosis of ovarian torsion, a different retrospective investigation revealed low sensitivity and excellent specificity . Although it is a useful tool, it is not the gold standard for diagnosis. A whirlpool sign is quite sensitive for ovarian torsion, according to two other investigations [49, 50]. A twisted vascular pedicle is indicated by the whirlpool sign, and circular vessels within the mass are visible on a Doppler ultrasonography. To ascertain the value of this symptom in ovarian torsion, more research on the diagnosis of ovarian torsion is required. If ultrasound results are unclear, magnetic resonance imaging (MRI), however costly, can be useful in identifying ovarian torsion. Compared to an ultrasound, an MRI can show a mass's constituent parts in greater clarity. However, due to radiation and density, computed tomography (CT) is not commonly utilized in cases with ovarian torsion. However, patients experiencing acute pelvic or abdominal discomfort must get CT in order to rule out other conditions such diverticulitis or appendicitis. Lastly, a conclusive diagnosis of ovarian torsion requires direct visualization. Therefore, for ovarian function to be saved early, the diagnosis must be surgically confirmed.
Management :
Surgery is the only method to confirm ovarian torsion and the gold standard for treating it. Laparoscopy and laparotomy are the two surgical techniques available. Laparoscopic surgery has grown in popularity. However, a laparotomy ought to be performed if ovarian or fallopian tube cancer is suspected. It is essential to evaluate ovarian viability and maintain its function throughout surgery. During surgery, a torn ovary can only be viably assessed by gross visual inspection. According to the traditional perspective, larger, black ovaries may appear nonviable due to lymphatic and vascular congestion.[23,33,86] However, a number of investigations have indicated that even those ovaries that resemble black or blue may continue to function after detorsion. More than 80% of patients exhibited normal follicular development following detorsion, according to postoperative ultrasonography follow-up. According to an animal study, even in cases of ovarian torsion with venous and lymphatic congestion, the artery may not be completely blocked. Surgical evaluation and ovarian function preservation have been the cornerstones of treatment for ovarian torsion in recent years. Surgery can be done in a variety of methods, and these days, detorsion and ovarian conservation are nearly always advised over salpingo-oophorectomy. A benign ovarian tumor is frequently treated with an ovarian cystectomy. If there is a strong suspicion of cancer, a salpingo- oophorectomy is required. Numerous observational studies indicate that detorsion is linked to ovarian function preservation.[60,69] The likelihood of function preservation increases with an early approach to torsion. According to an animal study, necrosis may appear if ovarian arteries are blocked for 36 hours or more. According to reports, ovarian conservation declines over time once symptoms appear. There is no proof that detorsion causes more adverse outcomes after surgery.[78,79] Laparoscopic surgery is safe for treating torsion in pregnant women, and management for pregnant patients is comparable to that for nonpregnant patients. Laparoscopic surgery can be used to treat ovarian torsion in newborns, who frequently exhibit irritability.
Prevention of recurrence:
There is a risk of recurrence after detorsion, but the incidence and causes are unknown. According to recent research, several methods can be used to decrease the risk of recurrence. One method is suppression of ovarian cysts by oral contraceptives. Another method is an oophoropexy. However, both approaches lack long?term follow-up and systematic study.
CONCLUSION:
Although the diagnosis of ovarian torsion is difficult and challenging, careful analysis of presenting symptoms (such as sudden onset of lower abdominal pain) is very critical. Pelvic ultrasonography can provide information on ovarian cysts.[85,86] Once ovarian torsion is suspected, surgery is the mainstay of diagnosis and treatment. Ovarian cystectomy, oophorectomy, or conservative treatment with detorsion can be the treatment of choice.
REFERENCES


Anjali Shinde, Dr. Dhairysheel Ghadge, Dr. Shailaja Jadhav, Management of Endometrial Cancer and Ovarian Torsion, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 3560-3582. https://doi.org/10.5281/zenodo.15719842
 10.5281/zenodo.15719842
10.5281/zenodo.15719842
