Department Allied and Healthcare, St. Soldier Institute of Pharmacy, Jalandhar-144011, Punjab, India.
Brain tumors represent a diverse group of neoplasms with varying biological behavior and clinical outcomes, necessitating accurate and timely diagnosis. Imaging plays a central role in the detection, characterization, and monitoring of these tumors. This review provides a comprehensive overview of current imaging modalities used in brain tumor diagnosis, including computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), and hybrid imaging techniques such as PET/CT and PET/MRI. Conventional imaging methods offer essential anatomical information, while advanced and molecular imaging techniques provide insights into tumor physiology and metabolism. The integration of multimodal imaging has significantly improved diagnostic accuracy and treatment planning. Furthermore, recent advancements in artificial intelligence and radiomics are enhancing the capabilities of imaging in neuro-oncology. Despite these developments, challenges such as limited accessibility, high costs, and diagnostic uncertainties persist. Future directions focus on the development of novel imaging biomarkers and the adoption of precision medicine approaches. This review highlights the evolving role of imaging in improving clinical outcomes for patients with brain tumors
Brain tumors constitute a complex and heterogeneous group of neoplasms arising either primarily within the central nervous system (CNS) or as metastatic lesions originating from extracranial malignancies. These tumors exhibit substantial variability in their histopathological characteristics, molecular profiles, growth dynamics, and clinical behavior. Such diversity presents considerable challenges in clinical practice, as prognosis and therapeutic strategies differ markedly across tumor subtypes, ranging from relatively indolent low-grade gliomas to highly aggressive malignancies such as glioblastoma. Consequently, achieving an accurate and timely diagnosis is of paramount importance for optimizing treatment planning, improving survival outcomes, and preserving neurological function1.
In contemporary neuro-oncology, medical imaging plays a pivotal role throughout the entire continuum of patient care, including initial detection, differential diagnosis, treatment planning, intraoperative guidance, and post-therapy monitoring. Unlike invasive diagnostic procedures, imaging offers a non-invasive means to visualize intracranial pathology, providing critical information regarding tumor location, size, morphology, and its relationship to adjacent eloquent brain structures. This is particularly important given the delicate and functionally critical nature of brain tissue, where even small lesions can result in significant neurological deficits2.
Historically, imaging of brain tumors was largely limited to structural techniques that focused on anatomical abnormalities. Computed tomography (CT), introduced in the 1970s, represented a major advancement by enabling rapid cross-sectional imaging of the brain. CT remains valuable in acute clinical settings, particularly for detecting intracranial hemorrhage, calcifications, and mass effect. However, its relatively limited soft tissue contrast reduces its sensitivity for detecting small lesions or distinguishing tumor subtypes. Despite these limitations, CT continues to serve as an important complementary modality, especially in emergency scenarios and in patients with contraindications to magnetic resonance imaging (MRI)3.
The advent of MRI marked a transformative milestone in neuroimaging, significantly enhancing the evaluation of brain tumors. MRI provides superior soft tissue contrast and multiplanar imaging capabilities, making it the gold standard for brain tumor assessment. Conventional MRI sequences, such as T1-weighted, T2-weighted, and fluid-attenuated inversion recovery (FLAIR), enable detailed visualization of tumor anatomy and associated edema. The use of contrast agents further improves lesion detection by highlighting areas of blood–brain barrier disruption, a hallmark of many malignant tumors. Nevertheless, conventional MRI alone may not fully capture the underlying biological heterogeneity of tumors, necessitating the integration of advanced imaging techniques4.
In recent years, advanced MRI modalities have significantly expanded the diagnostic capabilities of neuroimaging. Techniques such as diffusion-weighted imaging (DWI) provide insights into tumor cellularity, while perfusion-weighted imaging (PWI) assesses vascularity and angiogenesis—key indicators of tumor aggressiveness. Magnetic resonance spectroscopy (MRS) further complements these approaches by enabling the non-invasive analysis of tissue metabolites, offering clues about tumor composition and grade. Collectively, these techniques contribute to a more comprehensive understanding of tumor biology, facilitating improved differentiation between tumor types and grades5.
Beyond MRI, functional and molecular imaging modalities have gained increasing prominence in the evaluation of brain tumors. Positron emission tomography (PET), in particular, provides valuable metabolic information that complements anatomical imaging. By using radiotracers such as fluorodeoxyglucose (FDG) or amino acid analogs, PET can assess tumor metabolism, proliferation, and viability. This is especially useful in distinguishing tumor recurrence from treatment-related changes such as radiation necrosis, a common diagnostic challenge in neuro-oncology. Hybrid imaging systems, including PET/CT and PET/MRI, have further enhanced diagnostic accuracy by combining structural and functional data within a single examination6.
The integration of multimodal imaging approaches represents a significant advancement in the field, allowing clinicians to overcome the limitations of individual techniques. By combining anatomical, functional, and molecular information, multimodal imaging provides a more holistic assessment of brain tumors. This approach not only improves diagnostic confidence but also supports more precise tumor delineation, which is critical for surgical planning and radiotherapy targeting. Moreover, it facilitates longitudinal monitoring of treatment response and disease progression, enabling timely adjustments in therapeutic strategies7.
In parallel with these technological developments, the emergence of artificial intelligence (AI) and radiomics has introduced new dimensions to brain tumor imaging. AI-driven algorithms, particularly those based on deep learning, are increasingly being used for automated tumor detection, segmentation, and classification. Radiomics, which involves the extraction of quantitative features from medical images, offers the potential to uncover imaging biomarkers that reflect underlying tumor biology. These innovations hold promise for enhancing diagnostic accuracy, reducing interobserver variability, and advancing personalized medicine in neuro-oncology8.
Despite these advancements, several challenges remain. Variability in imaging protocols, limited accessibility to advanced imaging modalities, and difficulties in differentiating tumor progression from treatment-related effects continue to hinder optimal diagnosis. Furthermore, the translation of emerging technologies such as AI into routine clinical practice requires rigorous validation and standardization. Addressing these challenges will be essential for fully realizing the potential of imaging in brain tumor management.
Magnetic resonance imaging (MRI) is widely regarded as the primary imaging modality for the diagnosis and characterization of brain tumors, owing to its superior soft tissue resolution and versatility. Unlike ionizing radiation-based techniques, MRI provides detailed anatomical and physiological information without exposing patients to radiation, making it particularly suitable for repeated imaging during diagnosis and follow-up. Its ability to acquire images in multiple planes further enhances its utility in assessing tumor extent and its relationship with adjacent critical brain structures9.
2.1 Conventional MRI Sequences
Conventional MRI forms the foundation of brain tumor imaging and includes several standard sequences:
These sequences collectively enable clinicians to assess tumor size, morphology, and surrounding edema. However, they may not reliably distinguish between tumor types or accurately determine tumor grade, particularly in heterogeneous lesions10.
2.2 Advanced MRI Techniques
To overcome the limitations of conventional imaging, several advanced MRI techniques have been developed, offering insights into tumor biology beyond structural abnormalities.
Diffusion-Weighted Imaging (DWI)
DWI measures the diffusion of water molecules within tissues and is particularly useful in evaluating tumor cellularity. Highly cellular tumors, such as high-grade gliomas, often demonstrate restricted diffusion due to densely packed cells. Apparent diffusion coefficient (ADC) values derived from DWI can aid in tumor grading and differentiation from non-neoplastic lesions11.
Perfusion-Weighted Imaging (PWI)
Perfusion imaging assesses tumor vascularity by measuring parameters such as cerebral blood volume (CBV) and cerebral blood flow (CBF). High-grade tumors typically exhibit increased perfusion due to angiogenesis. PWI is therefore valuable in distinguishing low-grade from high-grade gliomas and in evaluating treatment response, particularly in differentiating tumor recurrence from radiation-induced changes12.
Magnetic Resonance Spectroscopy (MRS)
MRS provides metabolic information by analyzing biochemical compounds within brain tissue. Key metabolites include:
MRS can assist in tumor characterization, grading, and differentiation from non-neoplastic conditions, offering a non-invasive “biochemical profile” of lesions13.
2.3 Functional MRI and Emerging MRI-Based Techniques
Functional MRI (fMRI) and diffusion tensor imaging (DTI) have become increasingly important in preoperative planning. fMRI identifies eloquent brain regions responsible for critical functions such as language and motor activity, while DTI maps white matter tracts. These techniques are essential for minimizing postoperative neurological deficits by guiding surgical approaches9.
In addition, newer approaches such as radiomics and quantitative MRI are gaining attention. These methods extract high-dimensional data from images to identify patterns that may not be visible to the human eye. When combined with machine learning algorithms, they hold promise for improving tumor classification and predicting clinical outcomes14.
2.4 Clinical Applications of MRI in Brain Tumors
MRI plays a central role in multiple aspects of brain tumor management:
Despite its strengths, MRI has limitations, particularly in distinguishing tumor recurrence from post-treatment effects such as pseudoprogression or radiation necrosis. This has led to increasing reliance on complementary imaging modalities such as PET15.
2.5 Limitations of MRI
While MRI is indispensable, several challenges persist:
These limitations highlight the need for multimodal imaging approaches that integrate MRI with metabolic and molecular imaging techniques.
Computed tomography (CT) continues to hold an important, though more targeted, role in the imaging of brain tumors. Its primary strength lies in its ability to provide rapid and reliable evaluation of intracranial pathology, which is particularly crucial in emergency settings where immediate clinical decisions are required. CT imaging is widely available and relatively cost-effective, making it a practical first-line modality in many healthcare systems16.
One of the key advantages of CT is its high sensitivity for detecting acute intracranial hemorrhage, calcifications, and osseous involvement, features that can provide important diagnostic clues in brain tumors. For instance, calcifications are commonly associated with certain tumor types such as oligodendrogliomas, while hemorrhagic components may be seen in high-grade tumors or metastatic lesions. Additionally, CT is effective in identifying mass effect, midline shift, and hydrocephalus, all of which are critical for assessing disease severity and guiding urgent intervention17.
CT also plays a vital role in situations where MRI is contraindicated or not feasible. Patients with implanted medical devices, severe claustrophobia, or unstable clinical conditions may not tolerate MRI, making CT the preferred alternative. Furthermore, CT is frequently used in preoperative planning to evaluate bone involvement and surgical landmarks, complementing MRI findings18.
Despite these advantages, CT has inherent limitations that restrict its use as a standalone modality for brain tumor characterization. Its relatively poor soft tissue contrast compared to MRI limits its ability to delineate tumor margins and detect small or infiltrative lesions, particularly low-grade tumors. Moreover, CT provides minimal information about tumor physiology, such as cellularity, vascularity, or metabolic activity, which are essential for accurate tumor grading and differentiation. As a result, CT is generally used in conjunction with MRI and other advanced imaging techniques to achieve a comprehensive evaluation19.
Positron emission tomography (PET) has become an increasingly important modality in the evaluation of brain tumors by providing functional and metabolic insights that are not accessible through conventional imaging techniques. Unlike CT and MRI, which primarily depict anatomical structures, PET enables the visualization of biochemical processes such as glucose metabolism, amino acid transport, and cellular proliferation, thereby offering a more comprehensive understanding of tumor biology20.
4.1 PET Tracers in Brain Tumor Imaging
The diagnostic utility of PET largely depends on the choice of radiotracer. The most widely used tracer is 18F-fluorodeoxyglucose (FDG), which reflects glucose metabolism. High-grade tumors often exhibit increased FDG uptake due to their elevated metabolic activity. However, the use of FDG in brain imaging is limited by the inherently high glucose metabolism of normal brain tissue, which can reduce contrast and obscure lesions, particularly low-grade tumors21.
To overcome these limitations, amino acid-based tracers such as 18F-fluoroethyltyrosine (FET) and 18F-fluorodopa (FDOPA) have gained prominence. These tracers demonstrate higher tumor-to-background contrast because normal brain tissue exhibits relatively low amino acid uptake. As a result, they are more effective in detecting gliomas, delineating tumor margins, and identifying tumor recurrence 22.
4.2 Clinical Applications of PET
PET imaging has several important clinical applications in neuro-oncology:
Studies have shown that integrating PET with MRI significantly improves diagnostic accuracy compared to either modality alone, particularly in complex cases23.
4.3 Hybrid Imaging: PET/CT and PET/MRI
The development of hybrid imaging systems, such as PET/CT and PET/MRI, represents a major advancement in brain tumor imaging. PET/CT combines metabolic and anatomical data, improving lesion localization and diagnostic confidence. However, PET/MRI offers additional advantages, including superior soft tissue contrast and reduced radiation exposure.
Recent research suggests that PET/MRI is particularly valuable in glioma imaging, as it allows simultaneous acquisition of structural, functional, and metabolic data. This integrated approach enhances tumor characterization, improves delineation of tumor boundaries, and supports personalized treatment planning24.
4.4 Limitations of PET Imaging
Despite its advantages, PET imaging has certain limitations:
These challenges necessitate the use of PET as part of a multimodal imaging strategy, rather than as a standalone diagnostic tool25.
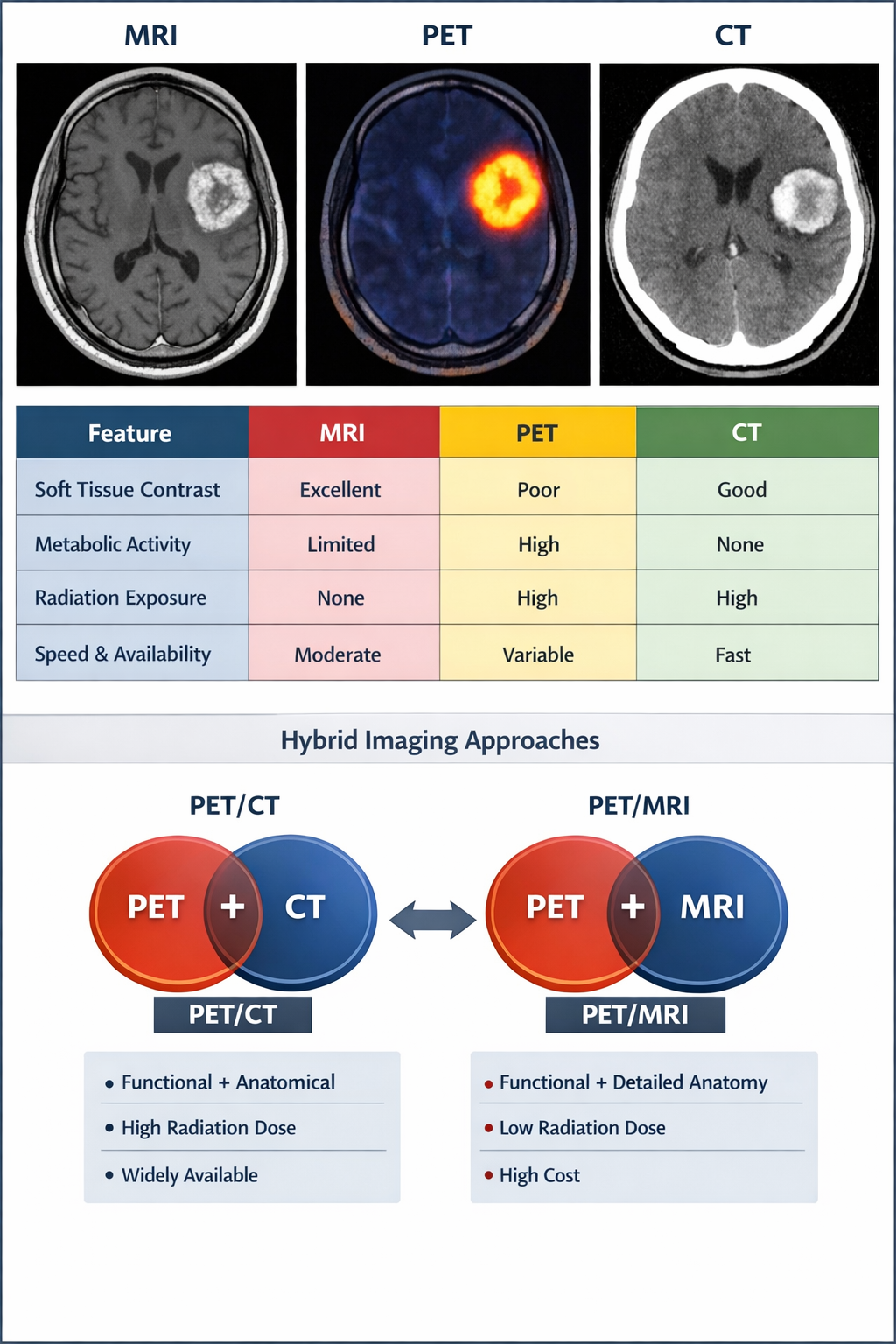
Figure 1. Comparative visualization of MRI, PET, and CT imaging modalities in brain tumor diagnosis.25
Hybrid imaging technologies have revolutionized brain tumor diagnostics by integrating anatomical and functional information within a single examination. Among these, positron emission tomography/computed tomography (PET/CT) and positron emission tomography/magnetic resonance imaging (PET/MRI) are the most widely utilized systems. These modalities aim to overcome the limitations of standalone imaging techniques by combining metabolic data from PET with high-resolution structural imaging, thereby enhancing diagnostic accuracy and clinical decision-making4.
5.1 PET/CT Imaging
PET/CT is the most established hybrid imaging modality and is widely available in clinical practice. It combines the metabolic sensitivity of PET with the anatomical detail provided by CT, allowing for accurate localization of metabolically active lesions. This integration is particularly useful in identifying tumor extent, detecting metastases, and guiding biopsy or radiotherapy planning20.
In neuro-oncology, PET/CT is commonly used with tracers such as FDG or amino acid analogs to evaluate tumor metabolism. The CT component contributes to attenuation correction and provides structural reference, although its relatively limited soft tissue contrast compared to MRI can restrict detailed brain tumor characterization. Despite this limitation, PET/CT remains a practical and efficient tool, especially in settings where MRI is not readily accessible26.
5.2 PET/MRI Imaging
PET/MRI represents a more recent and advanced hybrid imaging approach that combines the metabolic information of PET with the superior soft tissue contrast and multiparametric capabilities of MRI. This modality enables simultaneous acquisition of anatomical, functional, and molecular data, offering a more comprehensive evaluation of brain tumors27.
One of the key advantages of PET/MRI is its ability to incorporate advanced MRI sequences—such as diffusion-weighted imaging, perfusion imaging, and spectroscopy—alongside PET data. This allows for improved tumor delineation, more accurate grading, and better differentiation between tumor recurrence and treatment-related changes. Additionally, PET/MRI reduces radiation exposure compared to PET/CT, which is particularly beneficial for younger patients and those requiring repeated imaging28.
Clinical studies have demonstrated that PET/MRI provides higher diagnostic confidence in glioma assessment, particularly when using amino acid tracers. It is also increasingly used in treatment planning and monitoring, supporting a more personalized approach to neuro-oncology.
Table 1: Comparative Analysis: PET/CT vs PET/MRI
|
Feature |
PET/CT |
PET/MRI |
|
Availability |
Widely available |
Limited availability |
|
Imaging speed |
Faster |
Longer acquisition time |
|
Soft tissue contrast |
Moderate |
Superior |
|
Radiation exposure |
Higher (CT component) |
Lower |
|
Functional integration |
Limited |
Advanced (multiparametric MRI) |
|
Cost |
Relatively lower |
High |
|
Clinical utility in brain tumors |
Good for general assessment |
optimal for gliomas and detailed characterization |
PET/MRI is generally considered superior for brain tumor imaging, particularly in complex cases where detailed characterization is required. However, PET/CT continues to play a vital role due to its accessibility, speed, and cost-effectiveness15.
5.4 Limitations and Challenges
Despite their advantages, hybrid imaging modalities face several challenges:
These factors currently limit the widespread adoption of PET/MRI, although ongoing technological
Despite significant technological progress, several challenges continue to limit the effectiveness of imaging modalities in brain tumor diagnosis and management. One of the primary concerns is the limited specificity of conventional imaging techniques, particularly MRI, in differentiating tumor progression from treatment-related changes such as pseudoprogression and radiation necrosis. These phenomena often present with similar imaging characteristics, leading to diagnostic uncertainty and potentially inappropriate clinical decisions17.
Another major limitation is the heterogeneity of brain tumors, both at the histological and molecular levels. This complexity makes it difficult for a single imaging modality to fully characterize tumor behavior. Even advanced MRI techniques and PET imaging may not capture all aspects of tumor biology, necessitating a multimodal approach. However, integrating multiple imaging modalities introduces additional challenges, including increased cost, longer acquisition times, and complexity in data interpretation11.
The lack of standardized imaging protocols and biomarkers further complicates clinical practice. Variations in imaging acquisition parameters, analysis methods, and reporting standards across institutions can lead to inconsistencies in diagnosis and limit the reproducibility of research findings. This issue is particularly relevant for emerging fields such as radiomics and artificial intelligence, where model performance heavily depends on data quality and standardization (Bouhafra & El Bahi, 2025).
Accessibility and cost also remain significant barriers, especially in low- and middle-income countries. Advanced imaging modalities such as PET/MRI and molecular imaging techniques are expensive and not widely available, restricting their use to specialized centers. Additionally, PET imaging involves exposure to ionizing radiation and requires access to radiotracers, further limiting its routine application (Dunet et al., 2015).
Finally, the integration of artificial intelligence into clinical workflows presents its own set of challenges, including the need for large annotated datasets, regulatory approval, and clinician acceptance. Ensuring the interpretability and reliability of AI models is essential before they can be widely adopted in neuro-oncology.
FUTURE DIRECTIONS
The future of brain tumor imaging is closely aligned with the broader movement toward precision medicine, where diagnostic and therapeutic strategies are tailored to individual patient characteristics. One of the most promising developments is the integration of radiomics and artificial intelligence, which enables the extraction of quantitative imaging features and the identification of patterns that may not be visible to the human eye. These approaches have the potential to improve tumor classification, predict treatment response, and estimate patient prognosis with greater accuracy8.
Another important area of advancement is radiogenomics, which seeks to correlate imaging features with underlying genetic and molecular profiles of tumors. This integration can provide non-invasive biomarkers for tumor characterization and help guide targeted therapies. As genomic profiling becomes more accessible, combining it with advanced imaging techniques is expected to significantly enhance diagnostic precision1.
The development of novel PET tracers targeting specific molecular pathways represents another key direction. Unlike traditional tracers such as FDG, these newer agents can provide more specific information about tumor biology, including proliferation, hypoxia, and receptor expression. This will improve the ability to distinguish between tumor subtypes and assess treatment response more accurately27.
Hybrid imaging modalities, particularly PET/MRI, are also expected to gain wider adoption as technology advances and costs decrease. These systems offer comprehensive imaging by combining structural, functional, and molecular data in a single session, making them highly valuable for personalized treatment planning.
Efforts to standardize imaging protocols and reporting systems will be crucial for improving reproducibility and facilitating multicenter studies. International collaborations and consensus guidelines are expected to play a key role in this process.
CONCLUSION
In conclusion, imaging modalities are fundamental to the diagnosis, characterization, and management of brain tumors. Over the years, advancements in imaging technology have transformed neuro-oncology from a purely anatomical discipline to one that incorporates functional and molecular insights. MRI remains the cornerstone of brain tumor imaging due to its superior soft tissue resolution and versatility, while CT continues to play an important role in acute and complementary settings. PET and molecular imaging provide critical metabolic information, enhancing diagnostic accuracy and aiding in complex clinical decision-making.
The emergence of hybrid imaging techniques, particularly PET/CT and PET/MRI, has further improved the ability to integrate structural and functional data, enabling more precise tumor characterization and treatment planning. However, challenges such as limited specificity, high costs, and lack of standardization persist and must be addressed to fully realize the potential of these technologies.
Looking ahead, the integration of artificial intelligence, radiomics, and molecular imaging is expected to drive the next generation of neuro-oncological imaging. These innovations will support more personalized and data-driven approaches to patient care, ultimately improving clinical outcomes. Continued research, technological development, and global collaboration will be essential to overcome existing limitations and advance the field of brain tumor imaging.
AUTHORS CONTRIBUTION
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. All the authors are eligible to be an author as per the international committee of medical journal editors (ICMJE) requirements/guidelines.
ACKNOWLEDGMENT
It’s our privilege to express profound sense of gratitude and cordial thanks to our respected chairman Mr. Anil Chopra, Vice Chairperson Ms. Sangeeta Chopra, St. Soldier Educational Society, Jalandhar for providing the necessary facilities to complete this work.
CONFLICTS OF INTEREST
No Conflict of interest
REFERENCES


Sarika, Dr. Saruchi, Dr. Ajeet Pal Singh, Dr. Amar Pal Singh, Imaging Modalities in the Diagnosis of Brain Tumors: A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 32-43, https://doi.org/10.5281/zenodo.19368795
 10.5281/zenodo.19368795
10.5281/zenodo.19368795
