1Department of Pharmaceutics, OM Bio Sciences & Pharma College, Roorkee-247667, Uttarakhand, India.
2Department of Pharmacology, Kharvel Subharti College of Pharmacy, Swami Vivekanand Subharti University, Meerut-250005, Uttar Pradesh, India.
3Medicamen Biotech Limited, Haridwar-249403, Uttarakhand, India.
4Department of Pharmacy, Yogendra Nath Saxena College of Pharmacy & Research Centre, Amroha-244241, Uttar Pradesh, India.
5Department of Pharmacology, Metro College of Health Sciences & Research, Greater Noida-201310, Uttar Pradesh, India
Gouty arthritis, or gout, is a chronic inflammatory condition characterized by the deposition of monosodium urate crystals in joints due to elevated serum uric acid levels (hyperuricemia). Once considered a ‘disease of kings’ gout is now recognized as a widespread metabolic disorder with increasing prevalence worldwide, particularly due to modern lifestyle factors such as poor diet, obesity, and sedentary habits. This review explores the current understanding of gouty arthritis in the context of its pathophysiology, clinical features, prevention strategies, and evolving therapeutic approaches. The review begins with a discussion of uric acid metabolism and the inflammatory cascade triggered by urate crystal deposition. Risk factors, including genetic predisposition, comorbidities such as hypertension and diabetes, and dietary contributors, are examined. Clinical diagnosis, based on symptomatology, laboratory findings, and imaging, is highlighted alongside the differentiation between acute attacks and chronic tophaceous gout. Current management includes both pharmacological agents, such as Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), colchicine, corticosteroids, and uric acid-lowering drugs like allopurinol and febuxostat, and non-pharmacological measures like dietary modifications, weight control, and hydration. Preventive strategies are emphasized, especially for at-risk populations, with a focus on early intervention and patient education. Emerging therapies, including biologics targeting interleukin-1 (IL-1) and investigational agents in urate-lowering and anti-inflammatory categories, are discussed, along with the role of personalized medicine and genomic insights. An integrated approach combining lifestyle interventions, evidence-based pharmacotherapy, and future-oriented research is essential to improve patient outcomes and reduce the global burden of this painful yet manageable disease
Gouty arthritis (Gout) is a chronic, recurrent inflammatory disease that results from the deposition of monosodium urate crystals in joints and surrounding tissues (Figure 1) [1]. It primarily arises due to sustained hyperuricemia, which leads to the formation and deposition of crystals in the synovial fluid and connective tissue. Clinically, gout presents with sudden and severe episodes of joint pain, swelling, redness, and tenderness, most commonly affecting the first metatarsophalangeal joint, although other joints can also be involved [2]. Gout has been historically perceived as a ‘disease of affluence’ often associated with excessive consumption of rich foods and alcohol. However, contemporary research has clarified that its etiology is multifactorial, encompassing genetic predisposition, metabolic disorders, renal dysfunction, lifestyle factors, and use of certain medications [3]. Gout is not merely an episodic condition but a progressive disease that, if left untreated, can lead to chronic arthropathy, joint deformities, and kidney damage due to urate crystal accumulation. The global burden of gout has risen significantly over the past few decades, making it the most common form of inflammatory arthritis in developed countries [4,5]. Prevalence rates vary geographically but have been reported to range from 1 to 4 percent in the adult population. In the United States alone, it is estimated that over 9 million individuals suffer from gout. This rise is attributed to factors such as the aging population, increasing rates of obesity, sedentary lifestyles, and widespread consumption of purine-rich diets [6]. Gout is more common in males than females, with onset typically occurring in middle-aged men [7]. Postmenopausal women are also at increased risk due to declining estrogen levels, which affect uric acid excretion. The disease significantly impacts quality of life and contributes to loss of productivity, absenteeism from work, and increased healthcare costs due to frequent physician visits, diagnostic tests, and long-term medication use [8]. Moreover, gout is frequently associated with comorbidities like cardiovascular disease, hypertension, metabolic syndrome, chronic kidney disease (CKD), and type 2 diabetes, further amplifying its health and economic impact [9]. Early diagnosis of gouty arthritis is critical for effective disease management and long-term joint preservation. The initial symptoms of gout are often dramatic and easily mistaken for infections or other forms of arthritis. Misdiagnosis or delayed diagnosis can lead to repeated attacks, chronic inflammation, tophi formation, and irreversible joint damage [10]. Therefore, prompt recognition and confirmation through clinical history, serum uric acid levels, synovial fluid analysis, and imaging are essential steps in minimizing disease progression. Equally important is the implementation of preventive strategies, particularly in individuals at high risk due to genetic factors, diet, or co-existing metabolic disorders [11]. Lifestyle interventions such as weight reduction, limiting alcohol and purine-rich foods, increasing fluid intake, and regular physical activity play a vital role in both primary and secondary prevention of gout. Pharmacological prevention, through the use of urate-lowering therapies like allopurinol and febuxostat is essential in patients with recurrent gout, tophaceous disease, or urate nephrolithiasis [12]. Despite being a highly treatable condition, gout remains underdiagnosed and undertreated globally. Patient education, improved awareness among healthcare professionals, and adherence to evidence-based treatment guidelines are crucial to improving outcomes. With the emergence of newer therapeutic agents and personalized medicine, the future of gout management holds promise for more targeted and effective interventions [13].


Figure No. 1: Illustration of gout in the big toe and knee joints, highlighting inflammation due to monosodium urate crystal buildup.
Pathophysiology:
Gout is a metabolic disorder primarily caused by abnormalities in uric acid metabolism, resulting in hyperuricemia and the deposition of monosodium urate crystals in joints and tissues [14]. Uric acid is the end product of purine metabolism in humans due to the lack of uricase, an enzyme present in most other mammals that converts uric acid to the more soluble allantoin. The purines can be derived from both endogenous synthesis and dietary intake. Under normal physiological conditions, uric acid is dissolved in the blood and excreted primarily via the kidneys, with a smaller portion eliminated through the gastrointestinal tract [15]. However, when production increases or excretion decreases, serum urate levels rise, leading to a state known as hyperuricemia. Persistent hyperuricemia increases the risk of urate crystal formation, notably in less warm regions of the body, like the big toe, where the solubility of uric acid is reduced [16]. The deposition of monosodium urate crystals in the joint space is the trigger for the acute inflammatory response seen in gout. These crystals are recognized as danger-associated molecular patterns by the innate immune system. They are phagocytosed by resident macrophages, leading to activation of the NLRP3 inflammasome. This inflammasome complex promotes the cleavage of pro-interleukin-1β (pro-IL-1β) into its active form, IL-1β, a potent pro-inflammatory cytokine [17]. The release of IL-1β initiates a cascade of inflammatory mediators, including tumor necrosis factor-alpha, interleukin-6, and chemokines that attract neutrophils to the site of crystal deposition. Neutrophils, upon encountering the crystals, attempt to ingest them, which leads to the release of lysosomal enzymes and reactive oxygen species, further amplifying tissue inflammation and damage [18]. This acute inflammatory process results in the classical signs and symptoms of a gout flare: sudden onset of intense pain, redness, warmth, swelling, and loss of function in the affected joint (Figure 2) [19]. Repeated and untreated episodes of gout can lead to chronic gouty arthritis, characterized by the formation of tophi and progressive joint destruction. The chronic inflammation not only causes pain and deformity but also contributes to joint erosion and cartilage degradation. Moreover, sustained hyperuricemia has systemic implications, being associated with comorbid conditions such as hypertension, CKD, diabetes, and cardiovascular disease [21]. The pathophysiology of gout, therefore, involves a complex interplay between metabolic imbalance, immune activation, and inflammatory tissue damage. Understanding these mechanisms provides a strong foundation for developing targeted therapies aimed at interrupting the inflammatory cascade, improving uric acid excretion, or reducing uric acid production, all of which are essential components of effective gout management [22].
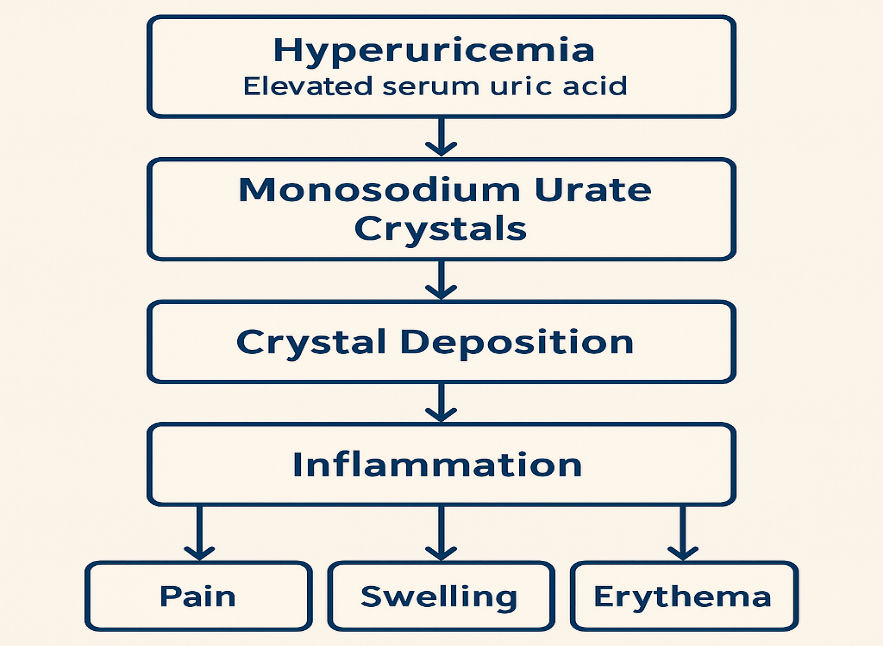
Figure No. 2: Illustrating the pathogenesis of gout.
Risk Factors and Triggers:
Gout is a multifactorial disease influenced by a combination of genetic, environmental, and metabolic factors. Understanding the risk factors and triggers is essential for developing effective prevention and management strategies (Figure 3) [23].
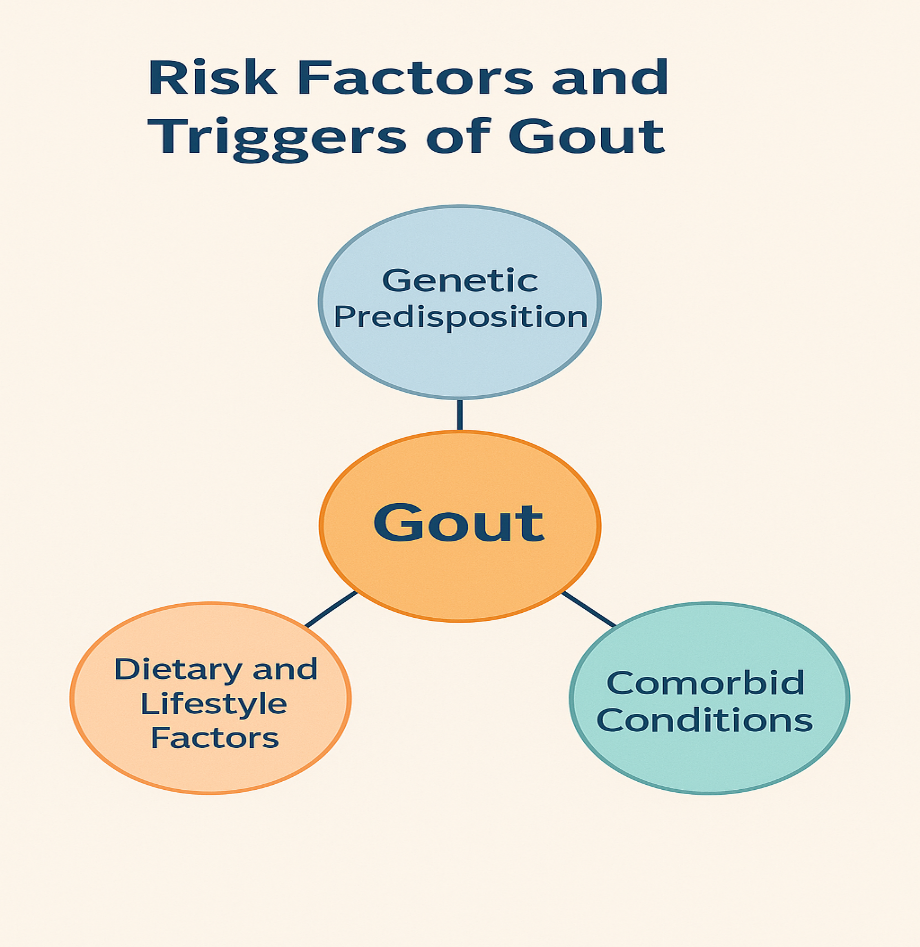
Figure No. 3: Illustration showing key risk factors contributing to gout.
1. Genetic Predisposition: Genetics plays a significant role in uric acid metabolism and the development of gout. Variations in genes involved in renal urate transport, such as SLC2A9, ABCG2, and SLC22A12, are associated with altered uric acid excretion and increased susceptibility to hyperuricemia. Individuals with a family history of gout are at a higher risk, especially in populations with high prevalence rates such as Pacific Islanders, African Americans, and certain Asian groups. Genetic studies also suggest that polymorphisms may influence the response to urate-lowering therapies, making personalized treatment increasingly relevant [24].
2. Dietary and Lifestyle Factors: Diet is a well-established modifiable risk factor for gout. Foods high in purines, such as red meat, organ meats, and certain seafood (anchovies and sardines), can increase serum uric acid levels. Alcohol and sugar-sweetened beverages rich in fructose are also known to raise uric acid production. Overeating, lack of physical activity, and excess body weight contribute to insulin resistance and decreased renal urate clearance, aggravating hyperuricemia. In contrast, a diet rich in vegetables, low-fat dairy, and whole grains has shown protective effects [25].
3. Comorbid Conditions: Several metabolic and renal conditions are strongly associated with gout. Obesity, particularly central obesity, increases uric acid production and reduces excretion. Hypertension and cardiovascular diseases are common in gout patients, and many antihypertensive drugs (thiazide diuretics) can further increase urate levels. CKD impairs uric acid excretion, making gout both a consequence and a contributing factor to renal dysfunction. Type 2 diabetes mellitus, metabolic syndrome, and dyslipidaemia are other common comorbidities that elevate gout risk [26].
Clinical Features and Diagnosis:
Gout is a common and increasingly prevalent inflammatory arthropathy resulting from monosodium urate crystal deposition in joints and soft tissues, secondary to chronic hyperuricemia. Accurate diagnosis and understanding of its clinical spectrum are essential for effective prevention and management [27].
1. Symptoms and Stages: Gout is a form of inflammatory arthritis caused by excess uric acid in the blood, which leads to the formation of sharp urate crystals in the joints. It typically affects one joint at a time, most commonly the big toe. The condition progresses through four key stages, each with distinct symptoms [28].
Stage 1-Asymptomatic Hyperuricemia: In this stage, uric acid levels are high, but no symptoms are present. It may go unnoticed for years unless detected through blood tests [29].
Stage 2-Acute Gout Attack: This stage is marked by sudden, intense pain in the affected joint, often occurring at night. The joint becomes red, swollen, warm, and extremely tender. Attacks may last from a few days to a week and can resolve on their own [30].
Stage 3-Intercritical Gout: This is the symptom-free period between attacks. Although the joint feels normal, urate crystals remain in the joint and may cause future attacks if not managed [31].
Stage 4-Chronic Tophaceous Gout: If untreated, gout can progress to this stage, where tophi form under the skin. Joints become permanently damaged, leading to pain, stiffness, and decreased mobility [32].
2. Diagnostic Criteria: Gout is diagnosed through a combination of clinical evaluation, laboratory tests, and imaging. The gold standard is the identification of monosodium urate crystals in synovial fluid using polarized light microscopy. Clinically, the sudden onset of joint pain, especially in the big toe, redness, swelling, and warmth are key indicators. Elevated serum uric acid levels support the diagnosis but are not definitive alone. Imaging techniques like ultrasound may reveal a “double contour sign” and dual-energy CT can detect urate deposits. The 2015 ACR/EULAR classification criteria also aid diagnosis, assigning points based on clinical, laboratory, and imaging findings to confirm gout [33].
3. Role of Imaging and Laboratory Tests: Imaging and laboratory tests play a crucial role in the accurate diagnosis and management of gout. Laboratory tests begin with serum uric acid measurement, which is often elevated in gout patients, though normal levels do not rule it out. The most definitive test is synovial fluid analysis, where monosodium urate crystals are identified under polarized light microscopy, confirming the diagnosis [34]. Imaging techniques complement laboratory findings. Dual-energy computed tomography is more advanced, enabling visualization of urate crystal deposits in joints and soft tissues, even in early disease. X-rays are less sensitive in early stages but are useful in chronic gout to show joint erosion, tophi, and bone damage [35]. These diagnostic tools are essential not only for confirming gout but also for ruling out other causes of joint pain, such as septic arthritis or pseudogout. Additionally, they guide treatment decisions, monitor response to therapy, and assess progression, especially in chronic or atypical cases. Together, imaging and lab tests ensure accurate, timely, and effective management of gout [36].
Current Management Strategies:
Gout management involves both pharmacological and non-pharmacological strategies.
1. Pharmacological Treatments: Gout management begins with controlling acute flares using NSAIDs, colchicine, or corticosteroids to reduce inflammation and pain. For long-term control, urate-lowering therapies like allopurinol and febuxostat are prescribed to maintain serum uric acid below target levels, preventing future flares and joint damage (Table 1) [37-41].
Table 1: Pharmacological treatments in gout management.
|
S. No. |
Category |
Details |
|
1 |
NSAIDs, Colchicine, Corticosteroids |
Used to manage acute gout flares by reducing inflammation and pain |
|
2 |
Uric Acid-Lowering Therapy |
Drugs like Allopurinol and Febuxostat help lower serum urate levels and prevent recurrent attacks |
2. Non-Pharmacological Approaches: Effective management also involves dietary modifications-reducing intake of purine-rich foods, alcohol, and sugary beverages. Adequate hydration and healthy lifestyle practices, such as weight control and regular exercise, support uric acid regulation. Patient education on disease understanding and the importance of medication adherence is vital to improving outcomes and preventing complications (Table 2) [42-45].
Table 2: Non-pharmacological approaches in gout management.
|
S. No. |
Approach |
Details |
|
1 |
Dietary Modifications |
Limit intake of purine-rich foods, alcohol, and sugary drinks, and promote low-fat dairy and vegetables |
|
2 |
Hydration and Lifestyle Interventions |
Encourage fluid intake, weight management, and regular physical activity |
|
3 |
Patient Education and Compliance |
Educate patients on treatment adherence, lifestyle choices, and recognition of symptoms |
Prevention of Gout:
Primary and secondary prevention of gout focus on reducing serum uric acid through lifestyle modifications, early diagnosis, and treatment of hyperuricemia [46]. Dietary interventions, nutraceuticals, and regular screening of at-risk individuals support long-term management and prevent disease progression (Figure 4) [47].
1. Primary Prevention: Primary prevention aims to reduce the risk of developing gout in healthy individuals. Key strategies include:
2. Secondary Prevention: Secondary prevention focuses on avoiding gout flares in those already diagnosed or with hyperuricemia:
3. Role of Diet and Nutraceuticals: Diet plays a critical role in managing and preventing gout:
4. Screening and Monitoring of At-Risk Individuals:

Figure No. 4: Illustration showing key strategies for gout prevention, including risk screening, lifestyle modifications, and early intervention.
Emerging Therapies and Future Perspectives:
Innovative approaches are shaping the future of gout management and treatment. Biologics and monoclonal antibodies, such as IL-1 inhibitors (canakinumab), are being explored for their potent anti-inflammatory effects in severe or refractory gout [62]. Gene therapy and personalized medicine offer promise in identifying genetic predispositions and tailoring treatment based on individual urate metabolism profiles, improving both efficacy and safety [63]. Additionally, advances in drug delivery systems, including nano-formulations and targeted delivery mechanisms, aim to enhance bioavailability, reduce side effects, and ensure more precise action of urate-lowering and anti-inflammatory drugs [64]. These developments hold significant potential to transform gout therapy in the coming years (Table 3) [65-71].
Table 3: Emerging therapies and future perspectives in gout management.
|
S. No. |
Area |
Description |
Examples |
Future Perspectives |
|
1 |
Biologics and Monoclonal Antibodies |
Target specific components of the immune response to reduce inflammation and uric acid levels |
IL-1 inhibitors (anakinra, canakinumab) and Tumor necrosis factor inhibitors |
Improved efficacy in resistant gout cases; fewer side effects compared to conventional therapies |
|
2 |
Gene Therapy and Personalized Medicine |
Modifies or regulates genes to treat hyperuricemia or personalize therapy based on genetic profiles |
CRISPR/Cas9-based approaches and pharmacogenomics-guided drug selection |
Tailored treatment with improved outcomes and reduced adverse effects |
|
3 |
Advances in Drug Delivery Systems |
Innovative delivery methods to improve drug bioavailability and patient compliance |
Nanoparticles, liposomes, transdermal patches |
Sustained release, targeted delivery, and minimized systemic exposure. |
Challenges and Gaps in Current Practice:
Despite being a well-understood and treatable condition, gout continues to present several challenges in clinical practice, particularly in the areas of treatment adherence, diagnosis, and healthcare access [72, 73]. Treatment adherence remains a major issue, with many patients failing to consistently take urate-lowering therapy due to misconceptions, lack of symptoms between flares, fear of side effects, or inadequate patient education [74]. This non-adherence leads to recurrent attacks and progression to chronic gout with joint damage [75]. Underdiagnosis and mismanagement are also common. Many cases are missed, especially in early or atypical presentations. Primary care providers may overlook gout in the absence of classic symptoms or fail to confirm the diagnosis via synovial fluid analysis [76]. Furthermore, there is often a lack of long-term management following acute flare treatment, with limited use of uric acid monitoring or dose titration of urate-lowering therapy to achieve target serum urate levels [77]. Mismanagement is also seen in the use of medications that elevate uric acid and inadequate patient counseling on lifestyle changes [78]. Additionally, socioeconomic and healthcare access issues contribute to disparities in gout care. Patients in low-income or underserved areas may face barriers such as limited access to rheumatologists, the cost of medications, or insufficient insurance coverage [79, 80]. These factors can delay diagnosis and hinder continuous care. Cultural beliefs and low health literacy further impact understanding and compliance with treatment [81]. Together, these gaps highlight the need for improved education of both patients and healthcare providers, more widespread use of evidence-based guidelines, and healthcare system reforms to ensure equitable access and continuity of care [82, 83]. Addressing these challenges is essential for reducing the burden of gout and improving patient outcomes through sustained, targeted, and accessible management strategies [84].
CONCLUSION:
Gouty arthritis remains a prevalent and impactful inflammatory condition, deeply intertwined with modern lifestyle factors, metabolic disorders, and genetic predispositions. Despite its ancient recognition, the disease continues to pose clinical challenges due to its chronicity, painful flares, and strong association with comorbidities such as hypertension, cardiovascular disease, and CKD. This review has highlighted the multifaceted nature of gout, encompassing its pathophysiology driven by monosodium urate crystal deposition, immune activation through inflammasome pathways, and the resulting intense inflammatory response. Early diagnosis and individualized treatment remain cornerstones in preventing disease progression and joint damage. The current management approach includes a combination of pharmacological therapies-such as NSAIDs, colchicine, corticosteroids, and urate-lowering agents like allopurinol and febuxostat-alongside non-pharmacological interventions such as dietary modifications, weight control, hydration, and patient education. Preventive strategies, including the identification and monitoring of at-risk individuals and the use of nutraceuticals, are critical in reducing disease burden. Importantly, the future of gout management lies in embracing personalized medicine, exploring novel biologics targeting inflammatory cytokines (IL-1 and TNF-α), and improving drug delivery systems for better adherence and efficacy. Molecular and genetic research, including the study of urate transporters and inflammasome regulators, holds promise for developing targeted and curative therapies. Integrating emerging therapeutic tools with patient-centered care can enhance outcomes, reduce complications, and ultimately improve quality of life.
REFERENCES





Ayushi Chauhan, Rohit Kumar, Akhil Chauhan, Gosiya, Saurabh Nimesh, Gouty Arthritis in the Modern Era: Prevention, Management, and Future Directions, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2510-2523. https://doi.org/10.5281/zenodo.15651456
 10.5281/zenodo.15651456
10.5281/zenodo.15651456
