Department of Pharmacy Practice, Shivlingeshwar College of Pharmacy, Almala, dist. Latur, Maharashtra.
In India, there are about 10 million people with epilepsy (PWE). Despite the availability of antiepileptic medications (AEDs), PWE have a significant treatment gap that ranges from 50 to 70%. Poor education, poverty, cultural beliefs, stigma, and inadequate healthcare infrastructure are the causes of this gap for curable epilepsy, while improper diagnosis and treatment are the causes of this gap for chronic epilepsy. Researchers from all across the world have made remarkable strides in the prevention, treatment, and cure of epilepsy. Significant advancements have also been made in Indian research, but the majority of these studies concentrate on the genetic correlations, epidemiological aspects of epilepsy, identification, and validation of novel AEDs in animal models of the condition.The dynamic process of epileptogenesis, in which neurons start to exhibit aberrant firing patterns that result in epileptic seizures, has been the subject of very few investigations. While studies on resected brain tissues from epilepsy patients are clinically useful, in-depth research can be done using animal epilepsy models. Lastly, to improve the caliber of epilepsy research in India, further financial assistance from the government and partnerships between basic research institutes, medical institutes, and companies are needed.The assessment of the present state of epilepsy research in India and the necessity of identifying viable anti-epileptogenic treatments are the main objectives of this review.
Epilepsy ranks among the most prevalent neurological disorders, leading to considerable medical and social challenges. This condition is defined by the occurrence of recurrent, typically unprovoked seizures, along with various cognitive, psychosocial, and societal repercussions. [1,2] Epilepsy encompasses a range of chronic, non-communicable neurological disorders characterized by spontaneous recurrent seizures.[3,4] Periods of aberrant electrical activity in the brain cause these seizures. Epileptogenesis is the process by which epilepsy arises in a brain that is otherwise normal. Head injuries, brain tumors, infections such as meningitis or encephalitis, stroke, birth defects, and occasionally even changes in blood sugar or sodium levels can all cause epilepsy. [5] The conditions can appear at any age and impact both male and female participants. Notwithstanding advancements in the treatment of epilepsy, there is still a significant treatment gap in India, which can be ascribed to a number of factors, including poverty, stigma, cultural beliefs, a lack of trained professionals, a lack of knowledge about antiepileptic medications (aeds),and cultural beliefs. [6] Pharmacoresistant epilepsy (PRE) is the term for epilepsy in which about three quarters of those with a diagnosis still have seizures despite the availability of various AEDs.[7] Therapeutic resection of the epileptogenic zone (EZ) is performed on a small percentage of PRE patients. Since the EZ is not distinct and focal, but rather because epileptogenic networks can disperse ictal activity to various parts of the brain, precise localization of the EZ is crucial in epilepsy surgery. The dynamic process of epileptogenesis must be understood in order to unravel the molecular clinical mechanisms underlying epilepsy, including PRE. [8] Around the world, 50 million people have epilepsy, and the majority of them live in developing nations. In India, there are thought to be over 10 million people with epilepsy (PWE). It affects about 1% of our population, with a higher prevalence in rural areas (1.9%) than in urban areas (0.6%). [9]. With 15 distinct seizure types and 30 distinct epilepsy syndromes, epilepsy is characterized by significant comorbidity, anxiety, depression, and increased mortality [10,11]. With the advent of more than 15 third-generation anti-epileptic medications (AEDs), the treatment of numerous seizure types has advanced significantly over the past 30 years [12].
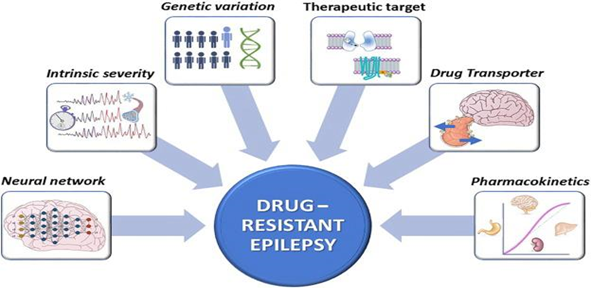
Fig. Drug resistant epilepsy [94]
About 70–80% of patients with newly diagnosed epilepsy who are currently taking AEDs achieve remission. These drugs are unable to control seizures in 20–30% of patients. Apart from that, no AED can stop the disease from developing before the first seizure occurs. Regretfully, drug-resistant epilepsy also exists, which is not managed by or responsive to AEDs. This demonstrates the pressing need to create suitable treatment plans to address the intricate case of epilepsy. A deeper comprehension of the various clinical and experimental strategies for the development and discovery of more effective treatment methods that can help prevent and control the diseases is necessary in order to develop better treatment paradigms for epilepsy using various pharmaceutical and therapeutic approaches [13,14,15].
This article's goal is to give a brief summary of some of the developments in drug treatment for epilepsy that have occurred over the past five years. It also discusses unmet needs that are currently present as well as developments that are probably going to happen in the near future.
Epidemiology
Prevalence
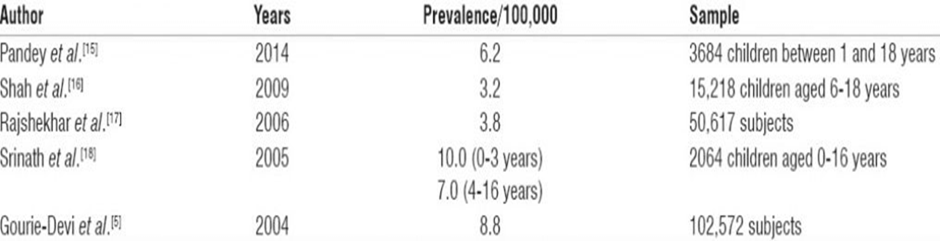
A prevalence rate of 8.8/1000 was noted in the Bangalore Urban-Rural Neuro-Epidemiological Survey, which included 102,557 participants. The estimated prevalence rate in rural communities was 11.9, nearly twice the rate found in urban areas (5.7). [16] India has published a number of prevalence studies on epilepsy. Table 1[17181920]
summarizes a few recent studies.
Table 1: Prevalence of epilepsy in various recent studies in India
Incidence
There is a dearth of information on epilepsy incidence in India. An age-standardized incidence rate of 27.3/100,000 annually was calculated by a study conducted in Kolkata. [21] There is still much to learn about the burden of drug-refractory epilepsy (DRE). An age-standardized incidence rate of 27.3/100,000 annually is suggested by the most recent of the very few incidence studies from India. [22] It is unknown how widespread medically intractable epilepsy is in India. According to reports from South India, the prevalence of hot water epilepsy (HWE), a type of reflex epilepsy in which seizures are brought on by quickly pouring hot water over the head, ranges from 1.14 to 2.99 cases/1000 population. [23, 24] According to reports, 3.6-3.9% of all epilepsy cases in rural South India are caused by HWE. [25]
Treatment Gap
The number of people with active epilepsy who are either not receiving treatment (diagnostic and therapeutic) or receiving insufficient treatment, expressed as a percentage of the total number of people with active epilepsy, is known as the treatment gap (TG), and it occurs in many developing nations.
[26] The two components of the TG are those who cannot or do not access biomedical facilities for diagnosis and treatment, as well as those who do not take their prescribed antiepileptic medications (AEDs) as directed. Numerous factors, such as poverty, cultural beliefs, stigma, lack of access to or knowledge of AEDs, inadequate infrastructure for health delivery, and a shortage of qualified professionals, are said to contribute to the gap. [26, 27] PWE seek treatment from traditional healers rather than allopathic practitioners due to superstitions and cultural beliefs.[28–31] In India, the percentage of people with epilepsy who receive treatment varies from 90% in rural areas to 22% in middle-class, urban areas. [32] It would be necessary to identify the primary cause of the gap for a given community and the most economical resource for a given circumstance in order to close this gap in the context of scarce resources. [33, 34-36] The distribution of epilepsy cases varies by socioeconomic status and geography, with a higher prevalence in males, rural areas, and those with lower socioeconomic status. There is a significant treatment gap (TG) for epilepsy in India. The percentage of PWE who do not receive treatment is known as TG. [37] According to reports, the TG in India varies from 22% in urban areas to up to 90% in rural areas. [38] Lack of awareness about AEDs, social stigma, cultural beliefs, indigenous treatment practices, and a significant lack of professionals with epilepsy management training are some of the factors contributing to the TG. Given the higher rates of epilepsy and the wide TG in rural areas, there is an urgent need to strengthen epilepsy healthcare in these areas. If left untreated, epilepsy can cause serious harm or even death. One potentially lethal consequence is status epilepticus (SE).
Etiology
The ILAE 2017 Classification divides seizure types into three categories based on the mode of onset: focal, generalized, and unknown.[39] Generalization, motor and nonmotor symptoms, and loss of consciousness are all possible outcomes of focal epilepsy. While symptomatic progressive epilepsy includes progressive disorders like tumors or neurodegenerative diseases, remote symptomatic epilepsy develops from a substrate after a single insult. According to a Bharucha et al. study [40], 23% of cases were symptomatic epilepsy, with 21% being remote symptomatic and 2% being progressive symptomatic. In this study, 46% experienced generalized seizures and 56% experienced focal seizures. In one study, the additional risk factors for epilepsy included head trauma, developmental delay, and a family history of epilepsy.[41] According to a population-based, case-control study, neonatal seizures, febrile seizures, complicated birth delivery, and a family history of epilepsy are all significant risk factors for developing epilepsy later on. [42] Hospital-based studies found that focal epilepsy was more common than other seizure types, accounting for up to 80% of all seizure types. [43] Nonetheless, generalized epilepsy was the most prevalent type in community-based studies, with generalized tonic-clonic epilepsy being the most prevalent subtype. [44, 45, 46] This could be as a result of community-based studies misrepresenting secondary generalization of focal epilepsy as primary generalization.
Neuroinfections
Pyogenic meningitis, tuberculosis of the central nervous system (CNS), viral encephalitides (such as dengue virus, Japanese encephalitis, and herpes simplex), neurocysticercosis (NCC), and a variety of other infections can cause acute seizures. In India, Japanese encephalitis has a regional tendency and can cause epilepsy as a result of postviral sequelae. [47] There are known Japanese encephalitis epidemic areas in some parts of India, where long-term sequelae lead to epilepsy. [48] Significant outbreaks of the disease occurred in 1978 and 2005, primarily in the Gorakhpur district of Eastern Uttar Pradesh, India. Reports of it have also come from West Bengal and Southern India. Infections (34%) were found to be the most common cause of fatal SE in a study that examined neuropathological correlates in fatal SE.
Neurocysticercosis
In India, NCC is one of the most frequent causes of epilepsy. It is caused by Taenia solium, a cestode tapeworm, in its larval stage. The feco-oral route of transmission happens when there is inadequate hygiene and sanitation. NCC can affect vegetarians as well, even though teniasis is caused by eating pork that has been infected with cysticerci. In India, 60% of NCC cases were solitary cysticercus granuloma (SCG), the most prevalent presentation. [49] More than 90% of SCG patients had seizures at first. [50] According to a large community-based survey with over 50,000 participants in the Vellore district of Tamil Nadu, Southern India, 30% of people had NCC as the cause of their active epilepsy. [51]
Head Trauma
Epilepsy is frequently caused by traumatic brain injury (TBI), particularly in young adults. Posttraumatic seizures are seizures that can occur after a head injury. If there are two or more unprovoked seizures, epilepsy is diagnosed. 11.4% of the 520 TBI patients in the cohort experienced seizures during the course of the study. 2.1% experienced early-onset seizures (less than one week), 2.7% experienced late-onset seizures (more than one week after head trauma), and 6.5% experienced immediate-onset seizures. [52]
Metabolic Conditions
Numerous metabolic disorders, such as hypoglycemia/hyperglycemia,hyponatremia/hypernatremia, and hypocalcemia/hypercalcemia, can cause epilepsy. Seizures in children can also result from inborn metabolic errors like phenylketonuria or aminoaciduria. However, there is a dearth of information on these causative factors from India. After stroke, metabolic factors were the second most frequent cause of epilepsy in the elderly population. [53]
Drug Resistant Epilepsy
Refractory epilepsy and pharmaco-resistant epilepsy are other names for drug-resistant epilepsy (DRE). It is characterized by the failure of two or more adequate trials of well-tolerated, carefully selected, and suitably employed AED regimens. These regimens can be used alone or in combination to treat seizures. DRE occurs in about one in four seizure patients [54]. Patients with DRE are more likely to sustain injuries, experience psychological issues, and pass away too soon [55,56,57]. The next section discusses a few of the theories regarding the mechanisms that underlie DRE.
1.Alterations in the Drug Targets
This hypothesis posits that the effectiveness of the treatment is diminished as a result of changes in the cellular targets of the medications. Research has indicated that the α2 subunit of the neuronal Na+ channel, encoded by the SCN2A gene, is associated with resistance to anti-epileptic drugs[54]
This theory, however, is unable to account for how changes in drug targets contribute to epilepsy in patients who are resistant to many medications with various mechanisms of action [58,59].
2.The Inability of the Drugs to Reach Their Targets
According to this transporter hypothesis, treatment resistance may be related to the overexpression of multidrug efflux transporters at the epileptic target. The most well studied efflux transporter is P-glycoprotein, whose major job is to keep the blood–brain barrier intact by reducing the build-up of the substrate medications in the brain [54]. Numerous investigations on DRE patients have reported aberrant expression in neural and glial cells as well as up-regulation of efflux transporters as P-glycoprotein in capillaries [60].
3.Real Targets Missed by the Drugs
Currently, the main purpose of AEDs is to prevent seizures, not to target the pathogenic processes that cause the disease. Patients with seizures have been found to have autoantibodies to ion channels linked to neuronal inhibition and excitation, such as voltage-gated ion channels and NMDA and GABA receptors; these cases have been observed primarily in various cases of occult cancer and encephalitis, but these patients typically do not respond to standard anti-epileptic medications [54,61,62].
General Principles of Pharmacological Treatment of Epilepsy
Antiseizure drugs (ASMs) are prescribed to epileptic patients as a preventative measure to lower their risk of experiencing more seizures. Freedom from seizures with negligible side effects is the aim. The therapy is symptomatic, which means that while the ASMs reduce the propensity to have seizures, they are not anticipated to affect the underlying process of the epileptogenic disease. Therefore, the development of epilepsy cannot be stopped by the medications currently on the market. This is the reason why "antiseizure medications" is now the preferred term and "antiepileptic drugs" has been deemed a misnomer.[63] A fundamental idea in the pharmacological management of epilepsy is individualization. ASMs vary in their effectiveness against various seizure and epilepsy types, and epilepsy is a heterogeneous disease with a variety of seizure manifestations. Therefore, the type of seizures the patient has must be taken into account when choosing the ASM, but other personal traits like age, sex, comorbidities, and current medications should also be taken into account. The first target dosage and the titration rate to achieve this dosage must be determined after the proper ASM has been chosen. Throughout the course of treatment, modifications may be required based on the clinical response. For instance, if the patient experiences side effects, the dosage may be reduced or the treatment may be stopped; if the patient continues to experience seizures, the dosage may be gradually increased. When an ASM has been used to its maximum potential without producing desired results, attempts are made to add another ASM or switch to a different ASM.
Research Progress in Epilepsy
Indian Epilepsy Association (IEA) affiliated to International Bureau of Epilepsy (IBE), Indian Epilepsy Society (IES) affiliated to International League Against Epilepsy (ILAE), are the two major epilepsy societies in India. IEA and IES consist of medical doctors and professionals from the fields of epilepsy. The role of IEA and IES is to form a task force to liaise with traffic authorities, public health officials, epidemiologists, and importantly, sister organizations, such as the Indian Academy of Paediatrics and Indian Medical Association, with the aim of preventing epilepsy. There are four medical institutes in India, All India Institute of Medical Sciences (AIIMS), New Delhi, National Institute of Mental Health and neurosciences (NIMHANS), Bengaluru, Sree ChitraTirunal Institute for Medical Sciences and Technology (SCTMIST), Thiruvananthapuram, and Christian Medical College (CMC), Vellore, that are extensively involved in clinical as well as basic epilepsy research.
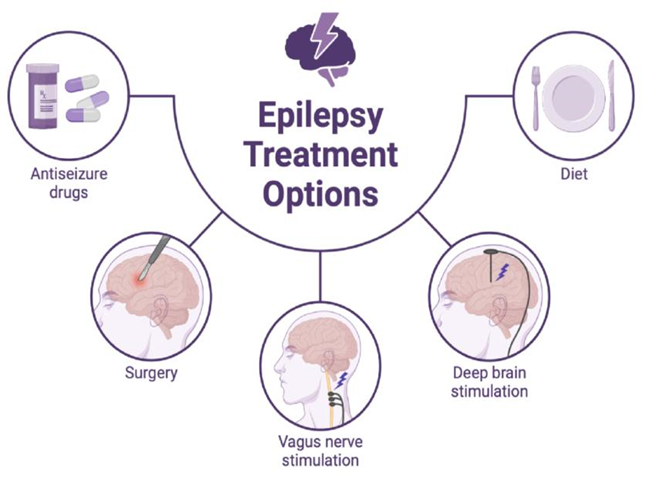
Fig. Epilepsy Treatment Options [95]
Research Progress in The Treatment of Epilepsy
New drug treatment
Synthetic drugs
Targets for the development of therapies are still being identified by ongoing fundamental research projects worldwide, including in India. The majority of research focuses on the function of either glutamate, an excitatory neurotransmitter, or gamma-aminobutyric acid (GABA), a crucial neurotransmitter that inhibits activity in the central nervous system. Because there are so many distinct underlying mechanisms involved in epilepsies, a single therapy will not work for everyone; instead, specialized techniques are required to handle particular syndromes. The anticonvulsant activity of the selective cyclooxygenase-2 (COX-2) inhibitor etoricoxib in pentylenetetrazole-kindled rats is linked to memory impairment, according to a study by Gupta et al. on seizures, oxidative stress, and learning and memory.[64] Using in-silico, in-vivo, and in-vitro methods, Mishra et al. employed the parameterizer and analytic software system [PASS] to ascertain the potential activity and mechanisms of piperine's anticonvulsant impact.[65] Using varying piperine dosages, the mortality rate and latency for convulsion development were noted in many experimental mice models of epilepsy. They used the whole cell patch clamp approach to assess how piperine affected the Na(+) and Ca(2+) channels. According to this study, piperine lowered related mortality, postponed the onset of tonic-clonic seizures upon pentylenetetrazole (PTZ) injection, and decreased mortality in the maximum electroshock seizure (MES) model. Lastly, they suggested that one of the components of piperine's intricate anticonvulsant processes is the Na(+) channel antagonist action. Another group proposed bezafibrate's potential for therapeutic uses in TLE and assessed its effectiveness as an anti-kindling agent in halting the onset of PTZ-induced seizures.[66] In a model of newborn status epilepticus caused by kainic acid, talampanel was demonstrated to be protective.[67] As new anticonvulsant drugs, N [4 (4 (alkyl/aryl/heteroaryl) piperazin 1 yl) phenyl] carbamic acid ethyl ester derivatives were recently created, produced, and pharmacologically assessed. Computer-aided identification of sodium channel blockers in the clinical treatment of epilepsy and ligand-based drug design of new heterocyclic imines of GABA analogues in the development of new GABA-AT inhibitors were described in studies based on in-silico analysis. [68,69]
Ayurvedic And Botanical Medications
Almost 60 different plants described in Ayurveda literature have been researched for their antiepileptic properties.Root extract from Asparagus racemosus has been demonstrated to have a positive impact on pentylenetetrazol-induced kindling, as well as related memory impairment and depression.[70] In mice with both acute and chronic epilepsy, aloe vera leaf extract showed anticonvulsive properties.[71] Anacyclus pyrethrum was found to have an impact on mice's oxidative stress, spatial memory, rhokinase II expression, and pentylenetetrazole-induced kindling, according to Pahuja et al. It was demonstrated that an aqueous extract of Anethum graveolens leaves may effectively lessen the seizures that mice had from pentylenetetrazole.[72,73] Indigenous populations in Uttarakhand's sub-Himalayan region have employed ethnomedical herbs to cure epilepsy.[74] The fraction that was separated from the Cedrusdeodara heartwood ethanolic extract exhibited anticonvulsant properties. [75] Research suggests that Ficusreligiosa L. figs may be used as a herbal adjuvant to phenytoin to help treat epilepsy and related behavioral comorbidities.[76] In albino rats with pentylenetetrazole-induced seizures, glycyrrhizaglabra root extract had anticonvulsant activity and reduced oxidative stress.[77] In rat models of epilepsy caused by maximum electroshock and pentylenetetrazole, Marsileaquadrifolia Linn shown antiepileptic effects.[78,79] When used as an adjuvant therapy for intractable epilepsies, black seed oil demonstrated encouraging clinical results.[80] Trichosanthestricuspidata prevented mice from developing pilocarpine-induced status epilepticus by regulating oxidative damage in the hippocampal region.[81] In experimental mice, ethanol preparations of Zingiberofficinale rhizomes and Veterinariazizanioides roots were shown to have anticonvulsant properties.[82,83]
In order to demonstrate the beneficial effects of yoga on epilepsy, Naveen et al. conducted psychological investigation.[84]
Optimizing Currently Used Treatments
Our group studied a total of 962 individuals with drug-refractory epilepsy (PRE) in order to assess the impact of lowering the amount of AEDs given to these patients during their hospitalization and to record any change in seizure frequency in the follow-up period. Our research demonstrated that optimizing or reducing the amount of AEDs in patients with PRE results in a considerable decrease in side effects and a drop in seizure frequency, or no change at all.[85] In a research comparing the safety and effectiveness of levetiracetam (LEV) and carbamazepine (CBZ) in treating partial epilepsy, Suresh et al. found that both LEV and CBZ monotherapy were well tolerated and showed comparable efficacy in treating partial epilepsy.[86] Nonintravenous routes of benzodiazepine administration should be taken into consideration for the management of acute seizures in children and adults when intravenous access is not available, according to a systematic review and meta-analysis study assessing the effectiveness and safety of AEDs in patients with active convulsive seizures.[87]
Surgical Management of Epilepsy
Up to 70% to 80% of people with newly diagnosed epilepsy eventually experience remission, and most of them do so within two years of the condition's inception. Even with the best AED treatment, over one-third of PWE still have seizures. Surgery is necessary to treat intractable epilepsy, which affects about one-third of epileptic patients. A unified framework involving neurology, neurosurgery, neuroradiology, psychiatric services, and the medical social worker is necessary for a comprehensive epilepsy surgical program. Furthermore, diagnostic instruments including magnetoencephalography, positron emission tomography, MRI, and SPECT are useful resources. In 1952, epilepsy surgery was first performed in India at CMC, Vellore. After temporal lobe epilepsy surgery, 70% of patients get seizure independence, and up to 30% of patients may stop taking their medications two years after the procedure. Approximately one-third of newly diagnosed epileptic patients undergoing long-term follow-up will experience inadequate seizure control with current AEDs. For PRE, surgery is still a viable option. Surgery could be either palliative (corpus callosotomy, vagal nerve stimulation, and repeated subpial transactions), functional (hemispherotomy), or curative (resective surgeries: amygdalohippocampectomy, lesionectomy, and multilobar resections). Compared to the less than 5% success rate with AEDs in PRE, the success range for epilepsy surgery in recommended patients is 50–86% in obtaining seizure freedom.[88] To make surgery less invasive and to avoid the neurological and cognitive impairments that surgery might cause, researchers are constantly improving surgical methods. The three main comprehensive epilepsy surgery centers in India are equipped with cutting-edge imaging technologies like magnetic resonance imaging (MRI), single photon emission computed tomography (SPECT), positron emission tomography (PET), and magnetoencephalography (MEG). They also have a multidisciplinary team of neurologists, neurosurgeons, neuroradiologists, electrophysiologists, psychologists, and psychiatrists working at Christian Medical College (CMC) in Vellore, Sree ChitraTirunal Institute for Medical Sciences and Technology (SCTMIST), Thiruvananthapuram, and the All India Institute of Medical Sciences (AIIMS) in New Delhi. These four institutes have conducted more than 4000 epilepsy surgeries over the past 20 years, with more than 2000 of the procedures taking place at AIIMS, New Delhi. The early detection of possible surgical candidates is essential to the success of any program including epilepsy surgery. Our team conducts a lot of research to improve surgical techniques. Our team conducts a lot of research to improve surgical techniques. According to our findings, a multidisciplinary strategy is required when making decisions on epilepsy surgery. This involves the collaboration of several program investigators to develop a comprehensive understanding of epileptogenesis and its effects on patients and caregivers. In a situation with limited resources, choosing which patients may benefit from surgery is just as crucial as knowing when not to operate due to the need for additional research. [88,89]
Prospects For the Future
Numerous fields are still undergoing intensive investigation, and significant developments that will improve the results for people with epilepsy are probably in the near future. We will talk about a few pertinent cases below. Increasing the use of technology in the treatment of epilepsy The increasing use of smartphones to record seizures in an out-of-hospital setting and the growing opportunities provided by Internet-based services in fields like telemedicine and distant education [89] demonstrate the growing use of information technology (IT)-based applications in epilepsy management in recent years. Additionally, the use of smartphone applications, or apps, to help individuals with epilepsy manage and cope with their condition is growing. The majority of these apps concentrate on topics including seizure tracking, medication adherence, treatment management, and health care communication [90]. Other applications, such as tools to enhance epilepsy diagnosis in non-specialist settings, are designed to support healthcare professionals (HCPs) [91, 92]. More sophisticated technology, such as machine learning (AI)-based methods, is anticipated to enable personalized ASM selection in the future. In a recent study, a computerized model that predicted a patient's reaction to a particular ASM was created using a machine learning technique that used clinical, genetic, and clinical trial data from individual patients [93].
This could pave the way to in-novative treatment strategies, such as the intermittent use of ASMs prior to the time at which a seizure is predicted to occur.
CONCLUSION
To better understand the biology behind epilepsy and help develop new treatments and a cure for chronic epilepsies, India has to improve the caliber of its epilepsy research. To carry out high-quality research in India, funding agencies' assistance and national and international partnerships are required. In order to comprehend the process of epileptogenesis, research should concentrate on the utilization of underutilized resected brain tissues from individuals with focal epilepsy following surgery. Knowing the epileptogenesis process may help find indicators for early epilepsy detection and treatment.
Improvements in the medication treatment of epilepsy persist even though second-generation ASMs have not significantly lessened the problem of pharmacoresistance. These developments are largely the consequence of additional medications and creative formulations, as well as a better understanding of the relative safety and effectiveness of currently available ASMs. Additional advancements can be attributed to telemedicine, patient empowerment, and remote learning technologies made feasible by smartphone apps for self-management. In the upcoming years, it is expected that more significant therapeutic advancements will take place. Advances in IT technology, the creation of novel precision therapies, the identification of biomarkers to direct drug development and routine clinical management, and, eventually, the introduction of truly innovative disease-modifying therapies are all expected to improve the clinical outcome for individuals with epilepsy thanks to continuous multidisciplinary efforts.
REFRENCES




Qureshi Khulood Mohammad Saifullah*, Dr. Ashok Giri, Mulgir Aachal, Pathan Asma, Patil Sakshi, Epilepsy Care in India: A Review of Recent Therapeutic Advances, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 877-891. https://doi.org/10.5281/zenodo.15006094
 10.5281/zenodo.15006094
10.5281/zenodo.15006094
