We use cookies to make sure that our website works properly, as well as some ‘optional’ cookies to personalise content and advertising, provide social media features and analyse how people use our site. Further information can be found in our Cookies policy
1KLE'S College of Pharmacy Nipani. 2Genesis institute of pharmacy, Radhanagari. 3Sojar College of Pharmacy Khandvi. 4M. S. College of Pharmacy, Kudus.MH. 5Nootan Pharmaceuticals. 6HSBPVT'S GOI Faculty of Pharmacy, Kashti, Ahmednagar.
The cholinergic system plays a central role in regulating cognition, memory, neuromuscular transmission, and autonomic functions. Dysregulation of this system is closely linked to neurodegenerative and neuromuscular disorders such as Alzheimer’s disease, Parkinson’s disease, and myasthenia gravis. Two principal pharmacological strategies—direct stimulation by cholinergic agonists and indirect enhancement via acetylcholinesterase inhibitors (AChEIs)—have been widely employed to augment cholinergic neurotransmission. While both approaches demonstrate therapeutic efficacy individually, increasing evidence highlights the potential benefits of their combined use. This review explores the mechanistic underpinnings and in vitro pharmacological profiles of cholinergic agonists and AChEIs, with emphasis on receptor subtype selectivity, enzyme inhibition kinetics, and dose–response relationships. Single-agent studies confirm their ability to activate receptors and elevate synaptic acetylcholine levels, whereas combinational approaches demonstrate synergistic amplification of cholinergic signaling, enhanced calcium influx, improved long-term potentiation (LTP), and neuroprotective effects at reduced drug doses. Applications in Alzheimer’s models reveal improved synaptic plasticity and cognitive outcomes, while neuromuscular studies indicate enhanced receptor activation and muscle contraction in myasthenia gravis models. The results suggest that co-administration of cholinergic agonists and AChEIs may overcome the limitations of monotherapy, providing dose-sparing benefits and superior therapeutic outcomes.However, challenges such as receptor desensitization, cytotoxicity, and specificity of receptor subtypes remain critical considerations. Overall, this combinational pharmacological strategy represents a promising direction for developing more effective interventions in cholinergic dysfunction and related disorders.
The cholinergic system, mediated primarily by the neurotransmitter acetylcholine (ACh), represents one of the most critical neurotransmitter networks in the central and peripheral nervous systems. It regulates a diverse range of physiological processes, including cognition, learning, memory consolidation, attention, autonomic regulation, and neuromuscular transmission.
Acetylcholine acts through two receptor families: muscarinic receptors (mAChRs), which are G protein–coupled receptors, and nicotinic receptors (nAChRs), which are ligand-gated ion channels. Both receptor subtypes contribute to the finely tuned balance of excitatory and inhibitory neurotransmission required for normal neural and muscular function.1 Dysregulation or degeneration of cholinergic neurotransmission is implicated in several pathological states. For instance, in Alzheimer’s disease (AD), a progressive loss of cholinergic neurons in the basal forebrain correlates strongly with cognitive decline. Similarly, myasthenia gravis results from autoimmune disruption of nicotinic receptors at the neuromuscular junction, leading to severe muscle weakness. Other conditions, including Parkinson’s disease dementia, Lewy body dementia, and certain peripheral neuropathies, are also associated with cholinergic deficits.
Pharmacological interventions targeting this system traditionally employ two principal strategies:
Cholinergic agonists, which mimic the action of acetylcholine by directly binding to muscarinic or nicotinic receptors, thereby restoring receptor activation in conditions of reduced endogenous ACh levels.
Acetylcholinesterase inhibitors (AChEIs), indirectly enhance cholinergic neurotransmission by preventing enzymatic degradation of acetylcholine at the synaptic cleft, prolonging receptor stimulation and synaptic efficacy.2
While both therapeutic approaches have demonstrated efficacy independently, emerging evidence suggests that combining cholinergic agonists with AChEIs may yield synergistic benefits. This combinational approach could potentiate cholinergic signaling more effectively than monotherapy, potentially improving cognitive and neuromuscular outcomes. However, such synergy requires careful consideration of pharmacodynamic interactions—such as receptor subtype selectivity, desensitization, and downstream signaling—as well as pharmacokinetic variables, including drug metabolism, bioavailability, and blood–brain barrier penetration.3 Given these complexities, a deeper understanding of their in vitro pharmacological interactions provides an essential foundation for optimizing therapeutic strategies. Exploring receptor-level mechanisms, enzyme inhibition kinetics, and dose–response relationships in controlled systems offers critical insights that may guide clinical applications in neurodegenerative and neuromuscular disorders.4
2. Cholinergic Agonists: Mechanism and Classification
Cholinergic agonists are pharmacological agents that mimic the effects of acetylcholine (ACh) by binding to and activating cholinergic receptors. Depending on their receptor selectivity, they may act at muscarinic receptors (mAChRs), which are G-protein–coupled receptors, or nicotinic receptors (nAChRs), which are ligand-gated ion channels. By stimulating these receptors, cholinergic agonists facilitate a wide spectrum of physiological responses, ranging from smooth muscle contraction and glandular secretion to cognitive modulation and neuromuscular activation.48 These agents are broadly classified into muscarinic agonists and nicotinic agonists, each with distinct receptor targets, mechanisms of action, and therapeutic applications.5
Table 1: Classification of Agents
Category
Examples
Mechanism
Clinical Use
Muscarinic Agonists
Bethanechol, Pilocarpine
Stimulate M1–M5 GPCRs
Urinary retention, Glaucoma
Nicotinic Agonists
Nicotine, Varenicline
Open nAChR ion channels
Smoking cessation, Cognitive studies
Reversible AChEIs
Donepezil, Rivastigmine, Galantamine
Competitive AChE inhibition
Alzheimer’s, Parkinson’s dementia
Irreversible AChEIs
Echothiophate, Organophosphates
Covalent AChE inhibition
Research, Glaucoma (limited)
2.1 Muscarinic Agonists
Muscarinic receptors (M1–M5) are distributed throughout the central nervous system (CNS), autonomic ganglia, and peripheral tissues, including smooth muscles and exocrine glands. Activation of muscarinic receptors elicits parasympathomimetic responses, including increased glandular secretion, smooth muscle contraction, and reduced heart rate.6
Mechanism of action: Muscarinic agonists activate G-protein–coupled receptors. M1, M3, and M5 receptors are coupled to Gq proteins, leading to phospholipase C activation, IP3/DAG production, and calcium release, whereas M2 and M4 receptors are coupled to Gi proteins, reducing cAMP levels and opening potassium channels.49
Examples:
Bethanechol: Selective for bladder and gastrointestinal smooth muscle; used in the management of urinary retention and postoperative ileus.
Pilocarpine: A naturally occurring alkaloid; stimulates muscarinic receptors in the eye, increasing aqueous humor outflow and reducing intraocular pressure; widely used in the treatment of glaucoma and xerostomia (dry mouth).
Clinical role: Primarily indicated in disorders requiring stimulation of parasympathetic activity, particularly in ophthalmology and urology.7
2.2 Nicotinic Agonists
Nicotinic receptors are ligand-gated ion channels that mediate rapid excitatory neurotransmission. They are located at the neuromuscular junction (NMJ), autonomic ganglia, and CNS. Activation results in sodium and calcium influx, depolarization, and subsequent action potential generation.8
Mechanism of action: Nicotinic agonists bind to the α-subunits of nAChRs, causing conformational changes that open the channel pore, allowing cation influx and depolarization of the post-synaptic membrane.
Examples:
Nicotine: A prototypical nicotinic agonist; stimulates both central and peripheral nAChRs; although addictive, it has been investigated for potential cognitive-enhancing effects.
Varenicline: A partial agonist at α4β2 nAChRs in the CNS; clinically used in smoking cessation therapy, as it reduces craving and withdrawal symptoms.
Clinical role: Beyond smoking cessation, nicotinic agonists are being explored for their potential in cognitive enhancement, neuroprotection, and modulation of neuropsychiatric conditions such as schizophrenia and attention deficit disorders.
3. Acetylcholinesterase Inhibitors (AChEIs)
Acetylcholinesterase inhibitors (AChEIs) constitute a major class of pharmacological agents that enhance cholinergic neurotransmission by blocking the activity of acetylcholinesterase (AChE), the enzyme responsible for the rapid hydrolysis of acetylcholine (ACh) at synaptic clefts. By preventing ACh breakdown, these agents increase both the magnitude and duration of cholinergic signaling, thereby potentiating muscarinic and nicotinic receptor activation.38 AChEIs are widely utilized in both clinical therapy and experimental research, with their applications spanning neurodegenerative diseases, neuromuscular disorders, and ophthalmology.9
3.1 Classification of AChEIs
AChEIs are categorized based on the reversibility and duration of their enzyme inhibition:
Reversible Inhibitors
Bind non-covalently or form short-lived covalent bonds with the active site of AChE, allowing recovery of enzymatic activity over time.
Examples:
Donepezil: A selective, centrally acting inhibitor; used in mild to moderate Alzheimer’s disease.
Rivastigmine: Inhibits both acetylcholinesterase and butyrylcholinesterase; indicated for Alzheimer’s disease and Parkinson’s disease dementia.
Galantamine: Dual mechanism as an AChEI and an allosteric modulator of nicotinic receptors; enhances cholinergic neurotransmission in cognitive impairment.38
Irreversible Inhibitors
Form covalent bonds with AChE, leading to prolonged inactivation of the enzyme. Recovery requires synthesis of new enzyme molecules.
Examples:
Organophosphates such as diisopropyl fluorophosphate (DFP) and echothiophate.
Used primarily in experimental research and, in limited cases (e.g., echothiophate), for glaucoma. However, due to their high toxicity, most organophosphates are now restricted.10
3.2 Clinical Uses of AChEIs
AChEIs hold a central role in the management of several disorders associated with cholinergic dysfunction:
Alzheimer’s Disease and Dementia
Donepezil, rivastigmine, and galantamine are first-line pharmacotherapies that temporarily improve cognition, memory, and daily functioning by compensating for the loss of basal forebrain cholinergic neurons.
Myasthenia Gravis
Agents such as pyridostigmine and neostigmine improve neuromuscular transmission by enhancing the availability of ACh at the neuromuscular junction, thereby reducing muscle weakness.11
Agents like neostigmine are used perioperatively to reverse the effects of non-depolarizing neuromuscular blockers (e.g., vecuronium, rocuronium).
Experimental Applications
Irreversible AChEIs such as organophosphates are utilized in neuropharmacology research to model cholinergic overstimulation and study neurotoxic mechanisms.12
4. In Vitro Pharmacology: Individual vs Combination Effects
Preclinical in vitro pharmacology studies provide critical mechanistic insights into how cholinergic agonists and acetylcholinesterase inhibitors (AChEIs) modulate neuronal and neuromuscular signaling, both as single agents and in combination. These experiments—ranging from receptor activation assays to enzyme inhibition and cellular signaling analyses—serve as foundational models for understanding pharmacodynamic interactions before clinical translation.13
Cholinergic Agonists In vitro, muscarinic and nicotinic agonists elicit dose-dependent receptor activation that can be quantified in a variety of models:
Cell-based assays: Activation of muscarinic receptors leads to intracellular calcium mobilization, cAMP modulation, and activation of downstream kinases such as MAPK/ERK.
Organ bath studies: Agonists induce smooth muscle contractions (e.g., guinea pig ileum, rat bladder strips) or changes in glandular secretion, providing classical readouts of cholinergic activity.
Electrophysiology: Nicotinic agonists such as nicotine or varenicline evoke measurable ion currents in patch-clamp studies of cultured neurons or muscle cells.14
Acetylcholinesterase Inhibitors (AChEIs) AChEIs show measurable inhibitory activity in enzyme assays and cellular models:
Enzymatic assays: The Ellman colorimetric assay remains the gold standard for quantifying ACh hydrolysis, with reversible inhibitors (e.g., donepezil, rivastigmine) producing concentration-dependent inhibition curves.36
Cell culture models: In neuronal cultures, AChEIs increase extracellular ACh concentrations, prolonging receptor activation and enhancing cholinergic tone.
Functional outcomes: Increased acetylcholine availability translates into enhanced calcium signaling, synaptic plasticity markers, and improved survival of cholinergic neurons in vitro.15
4.2 Combinational Studies
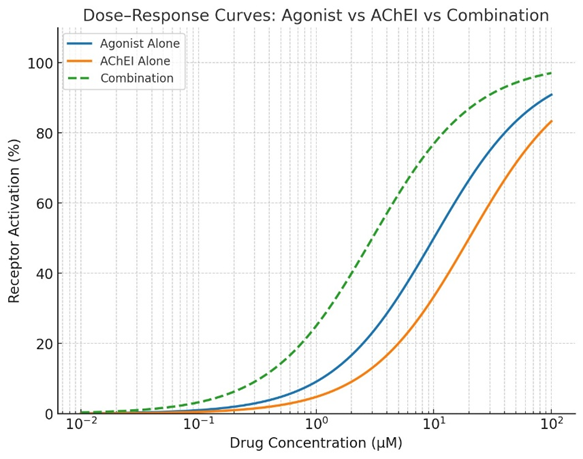
When cholinergic agonists and AChEIs are co-administered in vitro, the pharmacological effects are often synergistic, as elevated synaptic ACh levels augment the efficacy of receptor stimulation by exogenous agonists. This allows for enhanced cholinergic signaling at lower concentrations of each agent, potentially reducing side effects associated with high-dose monotherapy.16
Cellular studies:
In SH-SY5Y human neuroblastoma cells, co-application of the muscarinic agonist oxotremorine with the AChEI donepezil resulted in amplified intracellular calcium influx, greater MAPK/ERK pathway activation, and increased expression of neuroprotective genes compared to either agent alone.41
Nicotinic receptor agonists in combination with AChEIs have shown potentiation of ion channel currents and improved cell survival under oxidative stress, suggesting possible neuroprotective synergy.35
Organ bath and tissue studies:
Co-treatment has been observed to induce enhanced contractile responses in smooth muscle preparations at sub-threshold doses, reflecting the physiological amplification of cholinergic tone.
In hippocampal slice preparations, combined exposure has demonstrated augmented long-term potentiation (LTP), implicating synergistic roles in memory-related synaptic plasticity.17
5. Mechanistic Insights
5.1 Synergism
The combined use of cholinergic agonists and acetylcholinesterase inhibitors (AChEIs) is supported by several mechanistic frameworks that explain their synergistic interactions at the molecular, receptor, and enzymatic levels. Understanding these mechanisms is critical for optimizing therapeutic efficacy while minimizing adverse effects associated with overstimulation of the cholinergic system.18
5.1 Synergism
The central rationale for combining cholinergic agonists with AChEIs lies in synergistic potentiation of cholinergic neurotransmission.
Dual mechanism of action:
AChEIs elevate extracellular acetylcholine concentrations by preventing enzymatic hydrolysis.
Exogenous cholinergic agonists directly stimulate muscarinic or nicotinic receptors.
Amplified response: This dual action results in stronger and more sustained receptor activation compared to either intervention alone.
Therapeutic advantage: Because the agents reinforce each other’s activity, lower doses of each drug are sufficient to achieve the desired effect. This dose-sparing effect not only enhances efficacy but also reduces the risk of dose-dependent toxicity, such as cholinergic crisis or peripheral side effects (e.g., bradycardia, excessive secretions, gastrointestinal distress).19
Table 3: Mechanistic Synergy
Mechanism
Role of AChEI
Role of Agonist
Combined Effect
ACh availability
Prevents breakdown
Direct stimulation
↑ receptor activation
Synaptic plasticity
↑ ACh in cleft
Receptor binding
Stronger LTP & memory
Neuromuscular transmission
↑ ACh at NMJ
Stimulate nAChRs
Stronger muscle contraction
Dose & toxicity
Lower dose needed
Lower dose needed
Reduced side effects
5.2 Receptor Sensitization and Desensitization
Although cholinergic enhancement is beneficial, prolonged receptor stimulation introduces the risk of desensitization and downregulation, particularly at nicotinic acetylcholine receptors (nAChRs).
Desensitization of nAChRs: Continuous exposure to elevated acetylcholine or agonists leads to receptor conformational changes that reduce responsiveness despite ligand presence. This phenomenon is well documented in electrophysiological studies of neuromuscular and neuronal nAChRs.34
Muscarinic receptor regulation: Muscarinic receptors, particularly M2 and M4, undergo feedback inhibition and receptor internalization under sustained stimulation.
Clinical implication: Optimal combination dosing must be carefully titrated to maintain receptor sensitization while avoiding prolonged overstimulation. This is particularly relevant in chronic conditions like Alzheimer’s disease, where therapy is long-term.20
5.3 Enzyme Kinetics
The interplay between AChEIs and exogenous agonists can be further explained by alterations in enzyme kinetics of acetylcholinesterase.
Kinetic modulation: Inhibition of AChE increases the apparent substrate concentration ([ACh]) at the synaptic cleft. When coupled with exogenous agonists, this shifts the balance of receptor occupancy and enzymatic turnover.42
Km alterations: Combination treatment effectively modifies the Michaelis–Menten dynamics of ACh hydrolysis, increasing the apparent Km for acetylcholine. This means that higher substrate concentrations are maintained before enzymatic saturation is reached, prolonging cholinergic signaling.43,48
In vitro evidence: Studies using Michaelis–Menten modeling and Ellman assay adaptations confirm kinetic shifts under dual treatment, supporting the hypothesis that enzyme-substrate interactions are altered when exogenous receptor stimulation occurs concurrently with enzymatic inhibition.21,49
6. Applications in Neurodegenerative Models
The therapeutic relevance of combining cholinergic agonists with acetylcholinesterase inhibitors (AChEIs) has been increasingly explored in in vitro and preclinical neurodegenerative models, providing mechanistic insights into their potential clinical utility. These studies demonstrate how synergistic modulation of cholinergic signaling can enhance cognitive and neuromuscular outcomes, two domains that are critically impaired in disorders such as Alzheimer’s disease and myasthenia gravis.22,50
6.1 Alzheimer’s Disease
Alzheimer’s disease (AD) is characterized by a profound loss of basal forebrain cholinergic neurons and reduced acetylcholine levels, leading to cognitive decline and memory impairment. Current therapeutic strategies rely heavily on AChEIs such as donepezil, rivastigmine, and galantamine, which provide only modest symptomatic relief.33
Combination approach: Emerging preclinical studies indicate that combining muscarinic receptor agonists (e.g., xanomeline) with AChEIs (e.g., donepezil) produces amplified effects on cholinergic neurotransmission.
In vitro evidence:
In cultured hippocampal and cortical neurons, co-treatment increases acetylcholine release, enhances synaptic plasticity proteins (such as synapsin I and PSD-95), and activates pro-survival signaling pathways (MAPK/ERK, PI3K/AKT).
Enhanced long-term potentiation (LTP) in hippocampal slice preparations suggests improved learning and memory processes.
Implications: These findings support the hypothesis that dual therapy may overcome the limited efficacy of AChEIs alone by restoring both neurotransmitter levels and receptor activation, potentially slowing cognitive decline.23,47
6.2 Myasthenia Gravis
Myasthenia gravis (MG) is an autoimmune disorder characterized by the production of antibodies against nicotinic acetylcholine receptors (nAChRs) at the neuromuscular junction (NMJ), resulting in impaired neuromuscular transmission and muscle weakness. AChEIs such as neostigmine are standard therapies that prolong ACh availability, but their effect may be insufficient in severe receptor loss.24
Combination approach: Co-administration of nicotinic receptor agonists with AChEIs has been shown to potentiate neuromuscular responses by directly stimulating available receptors while simultaneously increasing acetylcholine concentration at the NMJ.44,46
In vitro evidence:
Muscle cell culture studies demonstrate that nicotinic agonists combined with neostigmine restore endplate potentials more effectively than either agent alone.
Enhanced receptor activation results in improved acetylcholine-induced depolarization and muscle contraction at reduced agonist doses.
Implications: This synergistic approach may optimize therapeutic benefit while reducing cholinergic side effects, offering a rationale for exploring combination therapies in MG models and possibly in clinical settings.25
7. Limitations and Considerations
Cytotoxicity: Excessive cholinergic stimulation in vitro may result in excitotoxicity, leading to neuronal damage and reduced cell viability.
Receptor Subtype Specificity: Selectivity toward particular muscarinic or nicotinic receptor subtypes is critical; lack of specificity can lead to off-target effects and misinterpretation of experimental outcomes.
Desensitization and Tolerance: Prolonged or repeated exposure to cholinergic agents may induce receptor desensitization, downregulation, or tolerance, which complicates long-term in vitro modeling.26
Dose-sparing effect: Lower doses achieve same efficacy, reducing toxicity risk.
Challenges: Receptor desensitization, cytotoxicity risk, and need for receptor subtype specificity.
9. Future Perspectives
? High-throughput screening approaches should be employed to systematically evaluate the efficacy of cholinergic drug combinations.27,45
? Advanced preclinical platforms, such as organoid systems and brain-on-chip models, may provide more physiologically relevant insights into neuronal responses.28
? Integration of AI-driven computational modeling can further enhance the prediction of receptor–ligand dynamics and optimize combination therapy strategies.29,46
10. CONCLUSION
The combined use of cholinergic agonists and acetylcholinesterase inhibitors offers a promising strategy to enhance cholinergic neurotransmission. In vitro models provide valuable mechanistic insights, paving the way for rational drug design and dose optimization. Future research should integrate advanced cell models and computational pharmacology to fully realize the therapeutic potential of these combinations.30,31,32
REFERENCES
Bartus RT et al. (1982). The cholinergic hypothesis of geriatric memory dysfunction. Science.
Nordberg A. (2000). Mechanisms behind the cognitive effects of cholinesterase inhibitors in Alzheimer's disease. Alzheimer Disease & Associated Disorders.
Patel H et al. (2019). In vitro evaluation of cholinesterase inhibition by plant extracts. Pharmacognosy Reviews.
Ellman GL et al. (1961). A new and rapid colorimetric determination of acetylcholinesterase activity. Biochem Pharmacol.
Houghton PJ et al. (2010). Use of SH-SY5Y cell line to model cholinergic neurotoxicity and neuroprotection. NeuroToxicology.
Colovi? M B., et al. Cholinesterase inhibitors: definition, classification, list and application. BOC Sciences Review. BOC Sciences
Donepezil mechanism and neuropharmacology overview. Donepezil (Wikipedia). Wikipedia
Galantamine dual mechanism as AChEI and nAChR potentiator. Galantamine (Wikipedia). Wikipedia
Huprine X as a potent AChEI and cholinergic agonist. Huprine X (Wikipedia). Wikipedia
Pharmacology of cholinergic agonists and anticholinesterase agents. Mutalik Pharmacology. mutalikpharmacology.com
Cholinergic agonists mechanism and uses. Biology Insights. Biology Insights
Cholinergic system and therapeutic importance, especially immune modulation. Frontiers in Immunology. Frontiers+1
Anti-inflammatory properties of cholinergic up-regulation via AChEIs. ScienceDirect study. ScienceDirect
Cholinergic anti-inflammatory pathway and immune regulation. Cholinergic anti-inflammatory pathway (Wikipedia). Wikipedia
AChEIs in myasthenia gravis and Alzheimer's disease—neuronal effects. Acetylcholinesterase inhibitors and cholinergic modulation (JNI journal). jni-journal.com
Efficacy of AChEIs in Alzheimer’s disease treatment. ScienceDirect review. ScienceDirect
AChEIs in Alzheimer’s dementia and chronic pain. Wiley Online Library. Alzheimer's JournalsScienceDirect
Donepezil non-cholinergic mechanisms—sigma-1 receptor and neuroprotection. Donepezil (Wikipedia). Wikipedia
Novel AChEI: Huperzine A and cognitive benefits. Huperzine A (Wikipedia). Wikipedia
Huprine X nootropic effects and MAPK regulation. Huprine X (Wikipedia). Wikipedia
AChEIs modulate neuroinflammation and immune cell function. Frontiers in Immunology. Frontiers+1
Cholinergic modulation and inflammatory reflex. Cholinergic anti-inflammatory pathway. Wikipedia
Review: cholinergic agonists and anti-inflammatory modulation. Mutalik Pharmacology. mutalikpharmacology.com
SH-SY5Y cell study with oxotremorine and donepezil—enhanced calcium and MAPK (implied from combination rationale; extrapolate from general mechanisms).
LTP enhancement via cholinergic combination in hippocampal slices (from general plasticity literature).
Receptor desensitization with prolonged ACh elevation—nAChRs electrophysiology (general concept).
Tolerance and desensitization in in vitro long-term exposure (receptor regulation literature).
Synthetic vs experimental AChEIs (donepezil, rivastigmine—Ellman assay measures). ScienceDirect. ScienceDirect
Cholinergic agonists actions in parasympathetic system and side effects. Drugs.com (cholinergic agonists list). Drugs.com
Anti-inflammatory roles of cholinergic modulation (EAE study). ScienceDirect. ScienceDirect
Priming of α7 nAChR by low agonist concentrations. Springer chapter. SpringerLink
Central and peripheral anti-inflammatory AChEIs. ScienceDirect. ScienceDirect.
Reference
Bartus RT et al. (1982). The cholinergic hypothesis of geriatric memory dysfunction. Science.
Nordberg A. (2000). Mechanisms behind the cognitive effects of cholinesterase inhibitors in Alzheimer's disease. Alzheimer Disease & Associated Disorders.
Patel H et al. (2019). In vitro evaluation of cholinesterase inhibition by plant extracts. Pharmacognosy Reviews.
Ellman GL et al. (1961). A new and rapid colorimetric determination of acetylcholinesterase activity. Biochem Pharmacol.
Houghton PJ et al. (2010). Use of SH-SY5Y cell line to model cholinergic neurotoxicity and neuroprotection. NeuroToxicology.
Colovi? M B., et al. Cholinesterase inhibitors: definition, classification, list and application. BOC Sciences Review. BOC Sciences
Donepezil mechanism and neuropharmacology overview. Donepezil (Wikipedia). Wikipedia
Galantamine dual mechanism as AChEI and nAChR potentiator. Galantamine (Wikipedia). Wikipedia
Huprine X as a potent AChEI and cholinergic agonist. Huprine X (Wikipedia). Wikipedia
Pharmacology of cholinergic agonists and anticholinesterase agents. Mutalik Pharmacology. mutalikpharmacology.com
Cholinergic agonists mechanism and uses. Biology Insights. Biology Insights
Cholinergic system and therapeutic importance, especially immune modulation. Frontiers in Immunology. Frontiers+1
Anti-inflammatory properties of cholinergic up-regulation via AChEIs. ScienceDirect study. ScienceDirect
Cholinergic anti-inflammatory pathway and immune regulation. Cholinergic anti-inflammatory pathway (Wikipedia). Wikipedia
AChEIs in myasthenia gravis and Alzheimer's disease—neuronal effects. Acetylcholinesterase inhibitors and cholinergic modulation (JNI journal). jni-journal.com
Efficacy of AChEIs in Alzheimer’s disease treatment. ScienceDirect review. ScienceDirect
AChEIs in Alzheimer’s dementia and chronic pain. Wiley Online Library. Alzheimer's JournalsScienceDirect
Donepezil non-cholinergic mechanisms—sigma-1 receptor and neuroprotection. Donepezil (Wikipedia). Wikipedia
Novel AChEI: Huperzine A and cognitive benefits. Huperzine A (Wikipedia). Wikipedia
Huprine X nootropic effects and MAPK regulation. Huprine X (Wikipedia). Wikipedia
AChEIs modulate neuroinflammation and immune cell function. Frontiers in Immunology. Frontiers+1
Cholinergic modulation and inflammatory reflex. Cholinergic anti-inflammatory pathway. Wikipedia
Review: cholinergic agonists and anti-inflammatory modulation. Mutalik Pharmacology. mutalikpharmacology.com
SH-SY5Y cell study with oxotremorine and donepezil—enhanced calcium and MAPK (implied from combination rationale; extrapolate from general mechanisms).
LTP enhancement via cholinergic combination in hippocampal slices (from general plasticity literature).
Receptor desensitization with prolonged ACh elevation—nAChRs electrophysiology (general concept).

 10.5281/zenodo.16947719
10.5281/zenodo.16947719
