Shivlingeshwar College Of Pharmacy, Almala, dist. Latur, Maharashtra.
Globally, cardiovascular disease continues to be a major cause of morbidity and mortality. Cardiovascular care has greatly improved recently thanks to developments in evidence-based medicine, which have also improved patient outcomes and quality of life. The most recent evidence-based developments in cardiovascular medicine, including pharmacological treatments, interventional procedures, and lifestyle changes, are thoroughly reviewed in this review article. We review the state of cardiovascular care today, emphasizing important discoveries from seminal meta-analyses and clinical trials. Our research shows how important evidence-based medicine is in influencing cardiovascular treatment plans, enhancing clinical judgment, and minimizing healthcare inequities. In order to promote optimal patient management and enhanced cardiovascular health, this review attempts to educate researchers, policymakers, and healthcare professionals about the most recent advancements in cardiovascular care by synthesizing the best available evidence.
With almost 20 million deaths per year, cardiovascular diseases (CVDs), especially ischemic heart disease and stroke, continue to be the world's leading cause of death [1]. Low- and middle-income environments account for three-quarters of cardiovascular-related deaths [2]. With a 93% prevalence, 54% mortality, and 60% disability-adjusted life years (DALY), cardiovascular diseases (CVDs) have accounted for the majority of the world's disease burden over the last three decades [3,4,5]. Disparities in the disease burden within and between continents, which cost USD 147 billion and USD 216 billion yearly for lost productivity and healthcare, respectively, further compound this [6,7,8]. The adoption of lifestyle changes, such as dietary, tobacco, and exercise interventions, as well as evidence-based therapies that seek to alter a recognizable and widely shared cardiovascular or at-risk phenotype, has contributed to the advancement of the fight against cardiovascular disease over the past 50 years. Notwithstanding the effectiveness of this strategy, the associated problems of illness prevention and treatment have proven difficult to resolve, most likely as a result of inaccurate deep phenotyping of individuals required to describe disease subgroups. The problem's scope is still quite large. It is estimated that by 2030, at least 44% of the adult population in the United States will have been diagnosed with cardiovascular disease, with 92.1 million adults (>1 in 3) currently having this diagnosis [9]. The sex-, age-, race-, ethnic-, regional-, and economic-based disparities in disease burden are likely caused by the well-established contribution of attendant comorbidities and traditional risk factors (e.g., hyperlipidemia, hypertension, diabetes mellitus, metabolic syndrome, chronic kidney disease), health behaviors (smoking and tobacco use, physical inactivity, nutrition, overweight and obesity), and other immutable factors (family history) to morbidity and mortality [10]. Even though the precise pathogenic landscape of CVDs is still not fully understood, atherosclerosis is thought to be the primary cause of this debilitating condition and has been identified as a deadly, complex, and multifaceted illness [11,12] Atherosclerosis, which leads to acute myocardial infarction (AMI), is thought to be primarily caused by lipid deposition in the coronary arteries and the inflammatory responses that follow [13]. Atherosclerotic plaque is primarily caused by lipid-laden macrophages, smooth muscle cells, T lymphocytes, and defective endothelium. Numerous cardiovascular problems may result from pathological remodeling of these components [14,15]. In order to achieve this, a thorough knowledge base for biomarker identification and personalized disease prevention and treatment prognosis prediction will be built using information from traditional clinical monitoring or observations of the various types of risk factors (e.g., diet, medication, other diseases or disorders) and data-driven systematic characterization of the genome, proteome, lipidome, metabolome [16,17,18].
Importance Of EBM In Cardiovascular Care:
Cardiovascular care has undergone a revolution thanks to evidence-based medicine (EBM), which has changed how medical professionals identify, treat, and manage cardiovascular diseases [19]. EBM helps medical professionals make well-informed decisions by combining clinical knowledge with the best available research evidence, which improves patient outcomes and quality of life [20]. Significant progress has been made in the treatment of heart failure, arrhythmias, coronary artery disease, and other cardiovascular disorders as a result of the application of EBM principles in cardiovascular care [21]. An outline of the significance of EBM in cardiovascular care, as well as its uses and difficulties, will be given in this article. In cardiovascular care, EBM is essential because it empowers medical professionals to make well-informed decisions that improve patient outcomes and quality of life.
Improved Patient Outcomes:
One of the main causes of morbidity and death in the world is cardiovascular disease (CVD). Even with advancements in technology and medical treatment, CVD continues to pose a serious threat to public health. Nonetheless, it has been demonstrated that evidence-based medicine (EBM) enhances patient outcomes in CVD by lowering hospitalizations, mortality rates, and enhancing quality of life [22].
1. Lower death rates: EBM has been demonstrated to lower death rates in patients with cardiovascular disease (CVD), including those who have atrial fibrillation, heart failure, and acute coronary syndromes [23].
2. Better symptom management: EBM helps medical practitioners better manage symptoms like exhaustion, shortness of breath, and chest pain [24].
3. Improved quality of life: EBM helps patients regain their independence and resume their regular activities by offering evidence-based treatments, which enhances their overall quality of life [25].
4. Decreased hospitalizations: EBM has been demonstrated to lower readmissions and hospitalizations among patients with CVD, which lowers medical expenses and enhances patient outcomes [26].
Better Decision-Making
1. Well-informed treatment decisions: EBM gives medical practitioners access to the best available data to help them make well-informed treatment decisions [27].
2. Fewer needless procedures: EBM minimizes harm and lowers expenses by assisting in the reduction of needless tests and procedures [28].
Enhanced Patient Safety
1. Decreased adverse events: EBM has been demonstrated to lower adverse events, including hospital-acquired infections and medication errors [29].
2. Better medication management: EBM lowers the risk of negative interactions and side effects by assisting medical professionals in managing medications [30].
Cost-Effective Care
1. Lower healthcare costs: EBM has been demonstrated to lower healthcare costs by reducing needless tests and procedures [31].
2. Better resource allocation: Evidence-based treatments are given priority when healthcare professionals use EBM to better allocate resources [32].
The State of Cardiovascular Therapies Today
The management of cardiovascular diseases (CVDs) involves a variety of approaches, including medication, surgery, and lifestyle changes. Over the years, there have been notable decreases in morbidity and mortality due in large part to the effectiveness of these current therapeutic approaches in controlling and lessening the effects of CVDs [33]. The cornerstone of managing CVD is pharmacological treatment. Because of their ability to lower cholesterol, statins are frequently prescribed and have played a significant role in lowering the incidence of atherosclerotic cardiovascular disease [34]. Statins successfully reduce low-density lipoprotein (LDL) cholesterol levels by blocking the enzyme HMG-CoA reductase, which lowers the risk of MI and stroke [35,36]. Another important class of medications, beta-blockers, lower blood pressure, slow the heartbeat, and prevent the effects of adrenaline on the heart [37]. Furthermore, because they dilate blood vessels and enhance blood flow, angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are frequently used to treat hypertension and heart failure [38]. However, patients with advanced or refractory CVD frequently require surgical interventions. By rerouting blood around blocked arteries, the well-known procedure known as coronary artery bypass grafting (CABG) increases blood flow to the heart muscle [39]. Patients with severe coronary artery disease benefit most from this surgery. In order to treat valvular heart diseases like aortic stenosis and mitral regurgitation, valve replacements—including mechanical and biological prostheses—are essential [40]. Affected patients' quality of life and survival rates can be considerably raised by these interventions. Because they have shorter recovery periods and lower risk profiles than open heart surgery, minimally invasive procedures like transcatheter aortic valve replacement (TAVR) are also becoming more and more popular [41]. Nevertheless, changing one's lifestyle is crucial to managing and preventing CVD. Dietary modifications, consistent exercise, quitting smoking, and weight control are some of these strategies [42]. Rich in fruits, vegetables, whole grains, and lean proteins, a heart-healthy diet can help lower risk factors like obesity, hypertension, and hyperlipidemia. Frequent exercise, such as strength training and aerobic activities, enhances general health and cardiovascular fitness. Given that smoking is a significant risk factor for many cardiovascular diseases, quitting is imperative. Comprehensive smoking cessation programs that include medication and counseling work well to help people stop smoking. Regular health screenings and the appropriate treatment of comorbid conditions like diabetes and hyperlipidemia through medication and lifestyle modifications are also considered preventative measures.
Emerging Pharmacological Treatments
As new drug classes with novel mechanisms of action are developed, the treatment landscape for CVD is changing quickly. By meeting unmet needs in the management of CVD, these new pharmaceutical treatments have the potential to greatly improve patient outcomes.
New Classifications of Drugs and How They Work
Inhibitors of PCSK9: Lipid management has been transformed by a novel class of medications known as proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors [43]. The liver's low-density lipoprotein (LDL) receptors are broken down by the enzyme PCSK9. These medications dramatically reduce LDL levels by blocking PCSK9, which increases the number of LDL receptors available to remove LDL cholesterol from the bloodstream [44]. Prominent examples of PCSK9 inhibitors are the monoclonal antibodies evolocumab and alirocumab, which have shown strong effectiveness in lowering cardiovascular events in patients with hypercholesterolemia and those who are statin intolerant [45]. SGLT2 inhibitors: By encouraging the excretion of glucose in the urine, sodium-glucose co-transporter 2 (SGLT2) inhibitors were first created to treat type 2 diabetes [46]. Nonetheless, they have demonstrated impressive advantages in lowering cardiovascular events and enhancing the results of heart failure [46]. These medications, which include dapagliflozin, empagliflozin, and canagliflozin, slow the progression of chronic kidney disease and lower the risk of heart failure hospitalization [47]. Osmotic diuresis, lowering the heart's preload and afterload, and possible direct myocardial benefits are some of their modes of action. New anticoagulants: Patients who need anticoagulation now have safer and more convenient options thanks to the development of novel oral anticoagulants (NOACs). NOACs like dabigatran, rivaroxaban, apixaban, and edoxaban have predictable pharmacokinetics in contrast to conventional vitamin K antagonists (like warfarin) [48]. Because these anticoagulants don't interact much with food or other drugs, they can be taken in a fixed dosage without requiring frequent monitoring [49]. These drugs also have a short plasma half-life, a generally predictable pharmacokinetic profile, and a rapid onset of action. Anticoagulant therapy can be started, continued, and stopped much more easily as a result [49]. These medications function by directly blocking important coagulation cascade components, such as factor Xa (rivaroxaban, apixaban, edoxaban) or thrombin (dabigatran). They are used to treat and prevent venous thromboembolism and to prevent stroke in atrial fibrillation.
Interventional Procedures For CVD
To increase heart blood flow, a non-surgical procedure called an interventional procedure is used to widen constricted coronary arteries. Since the recovery period following catheterization is significantly shorter than that following surgery, and because no large incision is made to open the chest, interventional procedures are not regarded as surgical procedures. An interventional procedure may be planned after a diagnostic cardiac catheterization has confirmed the presence of coronary artery disease, or it may be carried out when a blockage is discovered during the catheterization.
The Impact of Historical Innovative Technology:
1. Echocardiography
Cardiac catheterization was first used to measure pressures in the heart's chambers and great vessels. Later, it was used as a diagnostic technique to assess congenital heart conditions. Catheterization laboratory procedures underwent significant changes when echocardiography became available to offer the same information noninvasively. As data from echocardiographic studies became more accessible, transseptal catheterization volumes and skills decreased [50].
2. Percutaneous transluminal coronary angioplasty
Catheterization laboratories used to only perform diagnostic procedures, but with the advent of percutaneous transluminal coronary angioplasty (PTCA) in 1977, their role was drastically altered to include therapeutic procedures [51]. Training fellows and diagnostic angiographers to carry out these procedures was crucial in the beginning. This included preceptorships, proctored cases, and demonstration courses. In addition to requiring competency metrics and certifying exams, professional societies created specific guidelines. New problems emerged as PTCA gained popularity and was improved with the development of coronary stenting (percutaneous coronary intervention [PCI]). It was necessary to create heart teams and reinterpret the relationships between cardiologists and surgeons. The establishment of institutional and individual competencies as well as the concept of "centers of excellence" were significant outcomes.
3. Balloon valvuloplasty
With the development of balloon aortic valvuloplasty (BAV) and percutaneous mitral balloon valvuloplasty, a third wave with potentially broad implications emerged. Percutaneous mitral balloon valvuloplasty was accepted as a primary strategy for many patients due to its encouraging early results. However, centers of referral emerged at institutions where transseptal skills had been maintained, as rheumatic disease was rare in the United States. Otherwise, significant adjustments to evolving care and training systems were not required. . However, considering the high incidence of calcific aortic stenosis in the elderly and the significant risk of surgical valve replacement, the emergence of BAV was believed to have distinct implications. As a result, BAV was well received, and training sessions were usually completely booked [52]. However, by 6 to 9 months, almost universal restenosis was discovered by subsequent follow-up data, which resulted in a sharp decline in procedural performance. This reduced the impact of BAV on educational initiatives or the requirement to retrain practicing physicians. Modern Innovative Technology's Effect on Invasive Cardiology.
1.Transcatheter aortic valve replacement
Due to the significant unmet clinical needs, this procedure has experienced exponential growth. In order to promote the "rational dispersion" of the technology to carefully chosen locations with wide geographic distribution, professional societies in the early stages of transcatheter aortic valve replacement (TAVR) proposed guidelines for organizations and individual operators as well as a requirement for a national registry. The successful completion of additional randomized trials that demonstrated TAVR to be noninferior and, in certain respects, superior to surgical replacement regardless of surgical risk [53] was in line with these efforts and contributed to the field's rapid advancement. Important questions about its indication, administration, and regulation will continue to surface as this game-changing technology continues to have a significant impact on care over the next ten years.
2. Transcatheter interventions for stroke prevention
Transcatheter interventions have historically had a limited role in preventing strokes. Nonetheless, there have been two significant advancements in the field lately. First, the first left atrial appendage closure device (Watchman, Boston Scientific, Marlborough, Massachusetts) was approved by the U.S. Food and Drug Administration to prevent stroke in a subset of patients with nonvalvular atrial fibrillation. Second, the approval of PFO closure was made possible by a number of pivotal trials that showed that PFO closure was superior to medical therapy in patients with cry` ptogenic stroke and PFO [54,55]. Given the sizeable patient base that could benefit from these procedures, it is feasible to predict a notable increase in IC practices in this area. Interventional stroke prevention is still a relatively new field, though, and there are still many unresolved clinical needs and unanswered questions at the center of numerous ongoing studies. These include the relative effectiveness of direct anticoagulants, the impact of peridevice leak and device thrombus, post-procedural medical therapy, shared decision-making processes, and the potential for expanded indications and concurrent procedures [55].
4. Noncoronary endovascular interventions
Dotter's 1964 percutaneous transluminal angioplasty (PTA) marked the beginning of endovascular interventions, which have since expanded to include a variety of operations in several vascular beds. Other endovascular interventions flourished, such as PTA/stenting for lower extremity peripheral arterial disease, graft stenting for aneurysmal disease, and catheter-directed thrombolysis for thromboembolic disease, despite the initial enthusiasm surrounding PTA/stenting of carotid and renal arteries being dampened by the limited efficacy data, which resulted in a significant decline in their numbers. Many interventional cardiologists have become increasingly interested in endovascular interventions as a result of the decrease in PCIs for stable less extensive CAD over the past 20 years. In fact, there was a noticeable change in the mix of specialists performing endovascular procedures; in 2011, cardiologists performed 45% of all endovascular procedures [56]. Over the past ten years, transcatheter mechanical thrombectomy for acute stroke has gained attention. Despite being used for more than ten years, the publication of five successful landmark trials in 2015 solidified the importance of mechanical thrombectomy in contemporary stroke care and resulted in a significant rise in the number of procedures performed [57]. There are growing discussions regarding the possible inclusion of interventional cardiologists in the growing workforce for stroke interventions, given the significant unmet need and the existence of a generally recognized infrastructure for primary PCI [57]. Given the requirement for intricate training and cross-specialty collaboration, advancements in this field could have significant practical ramifications.
5. Interventions with Transcatheter Tricuspid Valve
1. Tricuspid Valve Repair: Using a catheter-based system, transcatheter tricuspid valve repair fixes the tricuspid valve by clipping the valve leaflets together [58].
2. Tricuspid Valve Replacement: Transcatheter tricuspid valve replacement is the process of replacing the tricuspid valve with a bioprosthetic valve using a catheter-based system [59].
Artificial Intelligence in Cardiovascular Disease:
The prevalence of CVDs is still increasing despite major advances in medical science and healthcare, which calls for creative approaches to prevention, early detection, accurate diagnosis, individualized treatment, and efficient management [60]. Integrating artificial intelligence (AI) into cardiology has become a game-changer, with previously unheard-of possibilities to completely alter the way cardiovascular diseases are perceived, identified, and managed [61], [62]. Machine learning, deep learning, natural language processing, and predictive analytics are just a few of the technologies that fall under the umbrella of artificial intelligence (AI) and have quickly advanced to support human decision-making and tackle important issues in cardiovascular care [63].
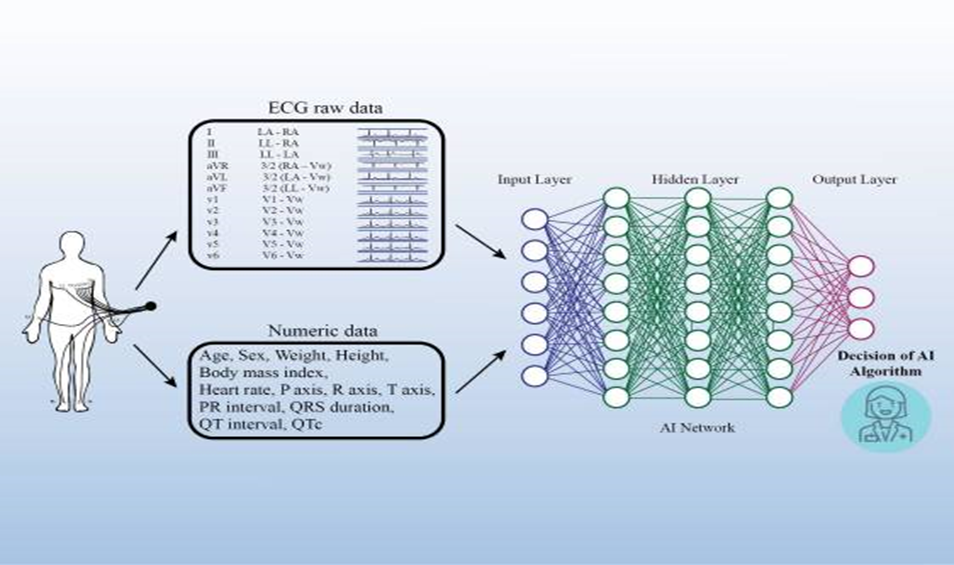
Fig01: Ai Algorithm for CVD [85]
Cardiovascular diseases have traditionally been diagnosed and treated primarily using traditional methods, which frequently have shortcomings in terms of accuracy, early detection, and customized treatment plans [64]. However, a new era marked by data-driven insights, predictive algorithms, and personalized medicine catered to each patient's particular characteristics has been brought about by the development of AI technologies [65], [66]. The application of AI in cardiology leverages vast amounts of data generated through various sources such as electronic health records (EHRs), imaging studies, genetic profiles, wearable devices, and continuous monitoring systems [67], [68]. These datasets, which are frequently distinguished by their volume and complexity, serve as the basis for creating AI-driven algorithms that are able to learn, adapt, and extract valuable insights from the data [68]. Enhancing clinical decision-making, increasing diagnostic precision, optimizing treatment plans, and improving patient outcomes are the goals of integrating AI into cardiology [69]. In addition to enhancing the skills of medical personnel, AI-driven solutions may also improve workflow, lower diagnostic errors, and facilitate preventative measures, all of which could result in more efficient and individualized patient care [70], [71]. Significant progress has been made in a number of areas as a result of the quick development and uptake of AI technologies in cardiology. Early detection and characterization of cardiovascular diseases are facilitated by the increased accuracy with which diagnostic algorithms can now analyze electrocardiograms (ECGs), echocardiograms, cardiac imaging, and other diagnostic modalities [72]. Additionally, by combining various patient data, such as genetic profiles, lifestyle factors, and imaging results, AI makes it easier to create individualized treatment plans and enable customized therapeutic interventions [62], [73]. Continuous real-time monitoring outside of clinical settings is now possible thanks to the convergence of AI with wearable technology and remote monitoring technologies [74]. These developments have the potential to improve long-term results by increasing patient engagement and enabling timely anomaly detection, early intervention, and individualized management of chronic cardiovascular conditions. AI-driven technologies have the potential to revolutionize cardiology research and clinical practice as they develop. AI is driving a paradigm shift in cardiovascular healthcare, emphasizing accuracy, efficiency, and better patient-centric care in everything from drug discovery and development to risk stratification, predictive analytics, and the development of clinical decision support systems. But even with the encouraging developments, there are a number of complex obstacles to overcome when incorporating AI in cardiology. Data security, algorithmic biases, ethical issues, regulatory compliance, and the successful integration of AI tools into current healthcare infrastructures are all crucial areas that require thoughtful analysis and calculated solutions [75]. The goal of this thorough review is to highlight the importance and innovation of incorporating artificial intelligence (AI) into cardiology while outlining its diverse effects on the transformation of cardiovascular healthcare.
Lifestyle Modification:
Fig02: Various Lifestyle Changes [86]
A healthy weight must be maintained in order to lower cardiovascular risk. A diet high in nutrients and low in calories, bad fats, and added sugars is the foundation of a heart-healthy diet. It promotes the consumption of lean proteins, foods high in fiber, and healthy fats while highlighting portion control. When paired with consistent exercise, these dietary patterns help people manage their weight and avoid obesity, which is a major risk factor for CVDs [76]. Two well-researched dietary regimens that have shown notable advantages for cardiovascular health are the DASH diet and the Mediterranean diet. The evidence in favor of these diets and other dietary patterns is summarized here. Mediterranean diet: The traditional eating practices of people in Mediterranean countries, including Greece, Italy, and Spain, served as the inspiration for this dietary pattern. Fruits, vegetables, whole grains, legumes, nuts, and seeds are among the many plant-based foods that define it. The main fat source in this diet is olive oil. Red meat should be consumed in smaller amounts, while fish and poultry should be consumed in moderation. Compared to a control group that followed a low-fat diet, people who followed a Mediterranean diet supplemented with extra-virgin olive oil or mixed nuts had a 30% lower risk of cardiovascular events, according to the PREDIMED study (Prevencio?n con Dieta Mediterra?nea) [77]. Following the Mediterranean diet is linked to a lower risk of CVDs, such as coronary heart disease, stroke, and overall mortality, according to meta-analyses [78]. By raising levels of high-density lipoprotein (HDL) cholesterol and decreasing levels of LDL cholesterol, the Mediterranean diet has been shown to improve lipid profiles. Additionally, it improves insulin sensitivity, inflammation markers, endothelial function, and blood pressure [79].
DASH diet: The effects of the DASH diet on blood pressure have been thoroughly investigated. It places an emphasis on fruits, vegetables, whole grains, low-fat dairy products, lean proteins, and a low sodium intake. Blood pressure significantly decreased for those who followed the DASH diet, especially those with hypertension, according to the original DASH trial [80]. According to later research, the DASH diet can also lower the risk of type 2 diabetes, improve lipid profiles, and lower the risk of CVDs [81].
Plant-based diets: Vegetarian and vegan diets are examples of plant-based diets that have been linked to a decreased risk of CVDs. In comparison to non-vegetarian diets, vegetarian and vegan diets are linked to lower blood pressure, better lipid profiles, decreased body weight, and a lower risk of ischemic heart disease, according to a systematic review and meta-analysis [82]. Vegetarians were 13% less likely than meat eaters to develop ischemic heart disease, according to the EPIC-Oxford study [83].
Dietary approaches: The combination of a heart-healthy diet (like the Mediterranean or DASH diet), low sodium intake, minimal added sugars, and avoiding trans fats is one of the dietary strategies for cardiovascular health that the American Heart Association (AHA) has recommended. A substantial lower risk of CVDs has been linked to the AHA's "Life's Simple 7" recommendations, which include diet, exercise, quitting smoking, controlling weight, blood pressure, cholesterol, and glucose [84].
CONCLUSION:
In order to diagnose, treat, and manage cardiovascular disease (CVD), evidence-based medicine, or EBM, is essential. EBM encourages better patient outcomes, better decision-making, increased patient safety, and cost-effective care by fusing clinical knowledge with the best available research evidence. With developments in cardiovascular health, pharmacological treatments, artificial intelligence, and empirical data, the future of EBM in CVD is bright, despite obstacles and constraints. In the end, EBM could revolutionize cardiovascular medicine and enhance the quality of life for millions of people globally.
REFRENCES





Syed Afnaan Naaz*, Dr. Ashok Giri, Shinde Akanksha, Upase Narsing, Wadekar Vishal, Yadav Anil, Cardiovascular Care Evolved: A Review Of Evidence-Based Advances, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 838-854. https://doi.org/10.5281/zenodo.15005100
 10.5281/zenodo.15005100
10.5281/zenodo.15005100
