Department of Quality Assurance, Shri Sarvajanik Pharmacy College, Mehsana, Gujarat
Candesartan is classified as an angiotensin II receptor type 1 antagonist. Angiotensin II receptor type 1 antagonists are widely used in treatment of diseases like hypertension, heart failure, myocardial infarction and diabetic nephropathy. Candesartan is an orally active lipophilic drug and possesses rapid oral absorption. It causes reduction in blood pressure and is used in treatment of hypertension. It is also used in the treatment of congestive heart failure and given as prophylaxis to reduce the severity and duration of migraine. Candesartan cilexetil, a prodrug of Candesartan, is available in the market under the trade names- Blopress®, Atacand®, Amias® and Ratacand®. Candesartan is also available in a combination formulation with a low dose thiazide diuretic, invariably hydrochlorothiazide, to achieve an additive antihypertensive effect. This paper reviews the pharmacological and pharmaceutical properties of Candesartan. Candesartan could be an attractive target for the generic industries.
Candesartan is an angiotensin II receptor blocker (ARB). ARBs are widely used in treatment of diseases like hypertension, heart failure, myocardial infarction and diabetic nephropathy. Candesartan is an orally active non-peptide tetrazole derivative. It finds most significant clinical use in the treatment of hypertension of all grades. Candesartan is a potent, highly selective ARB that is devoid of agonist activity. Candesartan cilexetil is an ester prodrug of its active metabolite Candesartan, to which it owns its therapeutic effect. It is also used in the treatment of congestive heart failure. Candesartan is used experimentally in preventive treatment of migraine. Hypertension is one of the most prevalent cardiovascular diseases in the world, affecting a big proportion of the adult population. Furthermore, hypertension is an independent risk factor for cardiovascular disease and is associated with an increased incidence of stroke and coronary heart disease. Although there have been many advances in the treatment over the past several decades, less than 25% of all hypertensive patients have their blood pressure adequately controlled with available therapies. The angiotensin II angiotensin blockers (ARBs) represent a newer class of antihypertensive agents. Candesartan is indicated in the treatment of hypertension and congestive heart failure. Candesartan cilexetil is marketed by AstraZeneca and Takeda Pharmaceuticals, commonly under the trade names of Biopress®, Atacand®, Amias® and Ratacand®. Candesartan is also available in a combination formulation with a low dose thiazide diuretic, invariably hydrochlorothiazide, to achieve an additive antihypertensive effect. Candesartan/hydrochlorothiazide combination preparations are marketed under various trade names including Atacand HCT®, Hytacand®, Biopress Plus®, Advantec® and Ratacand Plus®.
Physicochemical Properties
Candesartan is a tetrazole derivative (five-membered heterocyclic ring with 4 nitrogen atoms). Clinically it is used in the form of an ester prodrug- Candesartan cilexetil. Candesartan cilexetil is chemically 2-ethoxy-3-[21-(1H-tetrazol-5-yl) biphenyl-4 ylmethyl]-3H-benzoimiadazole-4-carboxylic acid 1-cyclo hexyloxycarbonyloxy ethyl ester (Structure 1), with chemical formula C33H34N6O6 and molecular weight 610.67. It is white to off-white powder with melting point 157-160° C. It is practically insoluble in water and sparingly soluble in methanol.
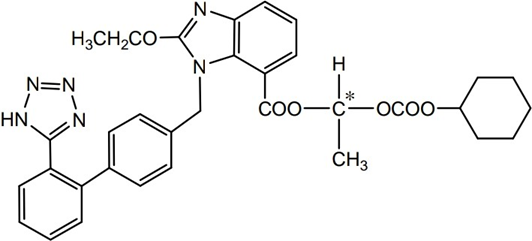
Structure 1: Candesartan cilexetil
Pharmacology
Mechanism of Action
Candesartan selectively blocks the binding of angiotensin II to angiotensin I in many tissues including vascular smooth muscle and the adrenal glands. This inhibits the angiotensin I mediated vasoconstrictive and aldosterone-secreting effects of angiotensin II and results in an overall decrease in blood pressure. Candesartan is greater than 10,000 times more selective for angiotensin I than angiotensin II. Inhibition of aldosterone secretion may increase sodium and water excretion while decreasing potassium excretion.
Hypertension
Studies with Candesartan cilexetil in healthy volunteers and patients with hypertension have shown a significant and long-lasting decrease of systolic and diastolic blood pressure. In multiple-dose studies with hypertensive patients, there were no clinically significant changes in metabolic function, including serum levels of total cholesterol, triglycerides, glucose, or uric acid. Same observations were observed in a 12-week study of 161 patients with non-insulin-dependent (type 2) diabetes mellitus and hypertension (ATACAND® product monograph)
Heart Failure
In heart failure patients, Candesartan ≥8 mg resulted in decreased systemic vascular resistance and pulmonary capillary wedge pressure.
Pharmacokinetic & Pharmcodynamic Profile
Candesartan cilexetil is rapidly and completely bioactivated by ester hydrolysis during absorption from the gastrointestinal tract to Candesartan, a selective AT1 subtype angiotensin II receptor antagonist. Candesartan is mainly excreted unchanged in urine and feces (via bile). It undergoes minor hepatic metabolism by o-de-ethylation to an inactive metabolite. The elimination half-life of Candesartan is approximately 9 hours. After single and repeated administration, the pharmacokinetics of Candesartan is linear for oral doses up to 32 mg of Candesartan cilexetil. Candesartan and its inactive metabolite do not accumulate in serum upon repeated once-daily dosing.
Absorption
Administration of the Candesartan cilexetil prodrug, the absolute bioavailability of Candesartan was estimated to be 15%. Food with a high fat content has no effect on the bioavailability of Candesartan from Candesartan cilexetil.
Distribution
The volume of distribution of Candesartan is 0.13 L/kg. Candesartan is highly bound to plasma proteins (>99%) and does not penetrate red blood cells. The protein binding is constant at Candesartan plasma concentrations well above the range achieved with recommended doses. In rats, it has been demonstrated that Candesartan crosses the blood-brain barrier poorly. It has also been demonstrated in rats that Candesartan passes across the placental barrier and is distributed in the fetus.
Metabolism and Excretion
Total plasma clearance of Candesartan is 0.37 mL/min/kg, with a renal clearance of
0.19 mL/min/kg. When Candesartan is administered orally, about 26% of the dose is excreted unchanged in urine. Following an oral dose of 14C-labeled Candesartan cilexetil, approximately 33% of radioactivity is recovered in urine and approximately 67% in feces. Following an intravenous dose of 14C-labeled Candesartan, approximately 59% of radioactivity is recovered in urine and approximately 36% in feces. Biliary excretion contributes to the elimination of Candesartan.
Pharmacodynamics
Candesartan inhibits the pressor effects of angiotensin II infusion in a dose- dependent manner. After 1 week of once-daily dosing with 8 mg of Candesartan cilexetil, the pressor effect was inhibited by approximately 90% at peak with approximately 50% inhibition persisting for 24 h. Plasma concentrations of angiotensin I and angiotensin II, and plasma renin activity, increased in a dose dependent manner after single and repeated administration of Candesartan cilexetil to healthy subjects and hypertensive patients. ACE activity was not altered in healthy subjects after repeated Candesartan cilexetil administration. The once-daily administration of up to 16 mg of Candesartan Cilexetil to healthy subjects did not influence plasma aldosterone concentrations, but a decrease in the plasma concentration of aldosterone was observed when 32 mg of Candesartan cilexetil was administered to hypertensive patients.
USES
Candesartan cilexetil is widely used for the treatment of hypertension and heart failure in clinical application. Lowering high blood pressure helps prevent strokes, heart attacks, and kidney problems. This drug works by relaxing blood vessels so blood can flow more easily. Candesartan belongs to a class of drugs called angiotensin receptor blockers. This medication is also used to treat congestive heart failure. This section contains uses of this drug that are not listed in the approved professional labelling for the drug but that may be prescribed by your health care professional. Use this drug for a condition that is listed in this section only if it has been so prescribed by your health care professional. This drug may also be used to help protect the kidneys from damage due to diabetes.
Dosage
The recommended starting dosage of Candesartan for most adults with high blood pressure (hypertension) is Candesartan 16 mg once a day. Based on the blood pressure response or Candesartan side effects, the dosage may be increased or decreased. With each change in dosage, it may take several weeks to see the full effects of Candesartan on lowering blood pressure.
Most people require a final dose of Candesartan 2 mg to 32 mg either as one daily dose or two smaller doses. It is available in 4 mg, 8 mg, 16 mg, and 32 mg.
Adverse effects
Common adverse effects are as follows:
CNS: Headache, dizziness, syncope, muscle weakness
Cardiovascular: Hypotension
Dermatologic: Rash, inflammation, urticaria, pruritus, alopecia, dry skin
Gastro-intestinal: Diarrhea, abdominal pain, nausea, constipation, dry mouth, dental pain
Respiratory: URI symptoms, cough, sinus disorders
Other: Cancer in preclinical studies, back pain, fever, gout.
CONCLUSION
Candesartan is a potent, long-acting, non-peptide tetrazole derivative, angiotensin II receptor antagonist having high selectivity for the AT1 subtype (angiotensin I). Candesartan reduces the blood pressure and is an effective antihypertensive agent in patients with mild to moderate hypertension. The drug also reduces blood pressure when used as monotherapy in patients with severe hypertension or when used adjunctively in patients with resistant hypertension. Importantly, Candesartan is safer, more tolerable and as effective as other commonly used antihypertensive agents. The drug therefore represents a useful therapeutic option in the management of patients with hypertension and congestive heart failure will be particularly useful in patients not responding to, or intolerant of, anti-hypertensive agents from other drug classes. It could be an attractive target for the generic industries.
REFERENCES


Jignesh Parmar*, Dr. Khushbu Patel, Dr. Pruthviraj Chaudhary, Dr. C. N. Patel, Candesartan Cilexetil: A Review of its Pharmacology and Therapeutic Uses, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2278-2282. https://doi.org/10.5281/zenodo.15239811
 10.5281/zenodo.15239811
10.5281/zenodo.15239811
