Akshaya Institute of Pharmacy, Tumkur.
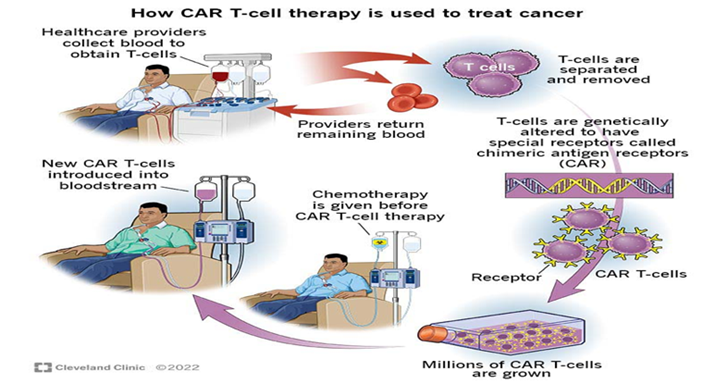
Cancer is the world’s top cause of death. Numerous cytotoxic immunotherapies and traditional treatments have been created and introduced to the market. The development of a viable immunotherapy that targets cancers at both the cellular and genetic levels is necessary due to the complicated behaviour of tumours and the involvement of multiple genetic and cellular variables in tumorigenesis and metastasis. The major histocompatibility complex is not involved in these; instead, the tumour antigen is directly identified. CAR T Cell therapy is a revolutionary new pillar in cancer treatment. CAR-T cell therapy is a groundbreaking cancer treatment that reprograms T cells to recognize and attack cancer cells. It involves extracting T cells from a patient's blood, genetically modifying them to produce chimeric antigen receptors (CARs) that target specific cancer cells, and reinfusing them into the body. The car T cells are work by T cells are collected from the patient's blood and genetically modified to produce CARs that bind to specific antigens on cancer cells. The modified T cells are then infused back into the patient's bloodstream, where they target and kill cancer cells. CAR-T cells can keep multiplying in the body, producing lasting anticancer results. Types of Cancer Treated by car T cell therapy is Blood cancers, such as leukaemia, lymphoma, and multiple myeloma. Specific types of lymphoma, including diffuse large B-cell lymphoma, follicular lymphoma, and mantle cell lymphoma. Next-generation CAR-T cell therapies are being developed to improve efficacy and safety. This review discusses current challenges, future directions, applications, structure, evolution of chimeric antigen receptors and finally working and production of CAR T Cells.
Chimeric antigen receptor T-cell therapy (CAR-T cell therapy) is a novel immunotherapy with promising results in the treatment of relapsed or refractory B cell malignancies.[1]
Chimeric antigen receptor (CAR) is a modular fusion protein comprising extracellular target binding domain usually derived from the single-chain variable fragment (scFv) of antibody, spacer domain, transmembrane domain, and intracellular signalling domain containing CD3z linked with zero or one or two costimulatory molecules such as CD28, CD137, and CD134. [2]
Chimeric antigen receptors (CARs) are receptor protein’s that have been modified to allow T cells to target a particular antigen. They are also referred to as chimeric immune receptors, chimeric T cell receptors, or artificial T cell receptors in the field of biology. The receptors are chimeric, combining into a single receptor the ability to attach to antigen and activate T cells.[3]
A CAR T cell product defined by the structure of the CAR protein expressed, the viral vector that mediates gene transfer, and elements of the cell culture process used to grow the number of cells ex vivo before reinfusion into the patient.[4]
Generic CAR T cell products generally have names with 2 words: the first indicates the gene component and the second describes the cell component.[4]
BACKGROUND:
Chimeric antigen receptors (CARs) are engineered receptors that provide immune effector cells (T cells) with a customised specificity.[5]
CARs consist of three components: an extracellular domain for antigen recognition derived from a single-chain variable fragment (scFv) of antibody, a transmembrane segment, and an intracellular T cell activation domain known as CD3.[6]
The purpose of CAR T cell therapy is to guide a patient’s or donor’s T cells to precisely locate and eliminate cancer cells. This approach holds significant potential for treating hematologic cancers as well as solid tumours, without being restricted by major histocompatibility complex.[7]
Immunotherapy has revolutionized cancer treatment, offering a flash of hope to patients facing late-stage metastatic tumours. science magazine acknowledged its impact, designating it as the “Breakthrough of the Year” in 2019. [8]
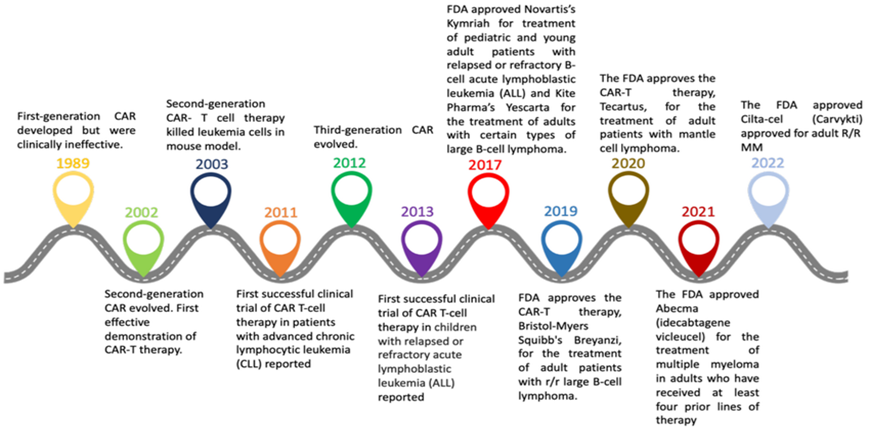
HISTORY OF CAR T CELL:[9]
|
Year |
Achievement |
|
1989 |
Production of effector T cells that express the receptor for chimeric T cells |
|
1993 |
CAR T cells from the first generation are not therapeutically effective |
|
2002 |
The first CAR T cells that are efficient against the prostate cancer antigen in the lab |
|
2003 |
Second generation CARs: CD19 directed CAR T cells have the ability to eradicate mice leukaemia cells |
|
2009 |
Relapsed or resistant leukaemia is treated using CD19 CAR |
|
2011 |
Patients with chronic lymphocytic leukaemia using CD19 CAR |
|
2013 |
Paediatric acute lymphoblastic leukaemia using CD19 CAR T cells |
|
2013 |
Cancer immunotherapy was named the “Breakthrough of the year” by science magazine |
|
2014 |
Inducible caspase-9 suicide gene system as a “safety switch” to reduce on-target, off-tumour toxicities in third-generation CAR T cells |
|
2015 |
Fourth-generation CARs that generate different compounds being explored for ovarian cancer, such as armoured CARs or TRUCKs (CAR redirected T cells that deliver a transgenic product to the targeted tumour tissue) |
|
2015 |
The CAR-NK cell concept |
|
2017 |
Clustered regularly interspaced short palindromic repeats (CRISPR) used to optimize CAR placement in T cells |
|
2017
|
For children and young adults with relapsed or resistant acute lymphoblastic leukaemia, the FDA has approved CD19-CAR-T cells |
|
2017 |
FDA approves CD19-CAR-T cells for adult DLBCL patients with relapses or resistance |
|
2018 |
For relapsed or resistant acute lymphoblastic leukaemia in children and young adults as well as relapsed or resistant DCBCL in adults, the EMA has approved CD19-CAR-T cell |
|
2019 |
In both adults and children with acute lymphoblastic leukaemia, dual CD19/CD22 CAR T cells are present |
|
2023 |
CDSCO made nexCAR19, India’s first approved CAR T cell therapy |
EVOLUTION:
Based on the endodomain’s structure, CAR T cells can be categorized into four generations since the first creation of CARs in 1989. A great illustration of how fundamental research can be clinic is the development of CAR treatment.[10]
NEED OF CAR T CELL THERAPY:
STRUCTURE OF CAR-T CELL:
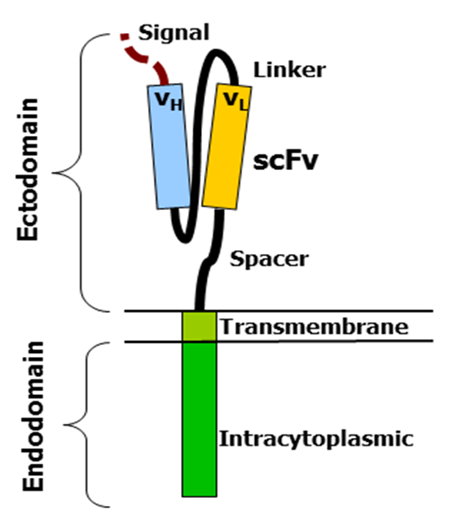
[15]
CARs involves mainly;
MECHANISM OF CAR-T CELLS
PRODUCTION OF CAR-T CELL:
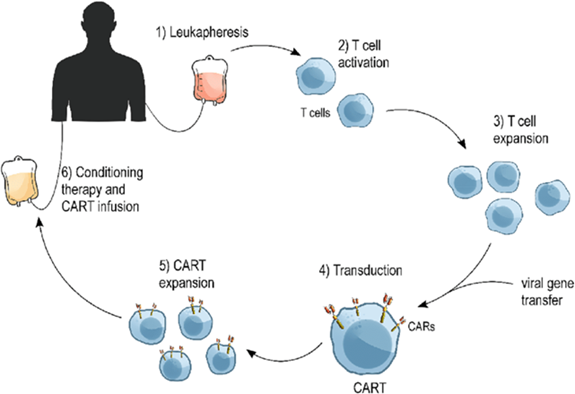
Steps involved in the Production of CAR T cell:[20]
PROCEDURE FOR CAR-T CELL THERAPY:[22]
patients frequently go through a conditioning programme prior to receiving a CAR T cell injection. Chemotherapy or other therapies to get the body ready for the injection of T cells that have been changed may be part of this. The conditioning regimen aids in fostering an environment that is more conductive to the proliferation and assault of cancer cells by the modified t cell.
The keystone of the process is the CAR T cell infusion. The patient receives the altered T cells intravenously. These cells are designed to express chimeric antigen receptors (CARs) on their surface. Typically, the infusion happens in a hospital environment so that the patient may be continuously watched for any negative responses.
Patients are constantly watched for any adverse responses or acute side effects following the infusion. Vital signs are monitored often, and the patient’s health is continuously watched for indications of neurotoxicity or cytokine release syndrome (CRS), two possible side effects of CAR T cell treatment.
Depending on their unique response and any potential consequences, patients usually stay in the hospital for a while after receiving a CAR T cell infusion. This duration might range from a few days to a few weeks. They get expert attention and supervision throughout this period to handle any negative effects and guarantee their safety.
patients get supportive treatment to manage side effects and maximise their comfort and well-being during the surgery and hospital stay. This might involve supportive therapy to address certain issues like CRS or neurotoxicity, as well as drugs to reduce symptoms like fever, nausea, and discomfort.
patients undergo CAR T cell therapy, a complex procedure requiring careful monitoring and supportive care to optimize outcomes. The treatment is tailored to each patient’s individual needs, aiming to achieve a durable, effective anti-cancer response while minimizing risks and complications.
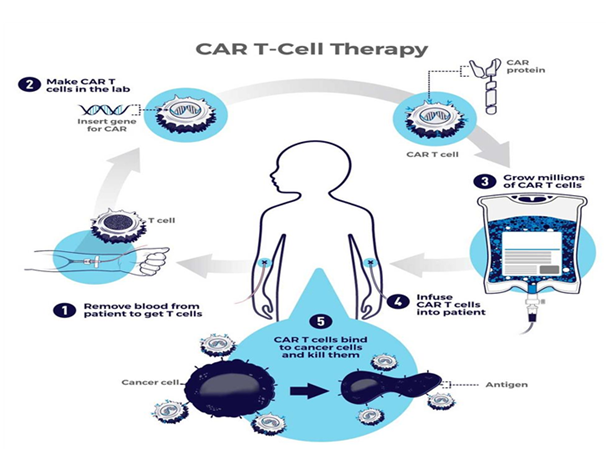
WORKING OF CAR T CELL:
[23]
CURRENT CHALLENGES IN THE CAR-T CELL THERAPY:[25]
FUTURE PERSPECTIVES:[26]
CD19-expressing blood cancers are most suitable for CAR T cell therapy due to their high tumour expression, easy access, and tolerability of B cell aplasia. However, only 5% of new cancer diagnosis are CD19-targetable by licensed products. Innovative strategies to improve tumour killing efficacy, CAR T cell persistence, and activity control are being pursued to bring CAR T cell therapies to other diseases.
The future of CAR T cell therapy is promising, with ongoing research and development aimed at overcoming current challenges and enhancing its therapeutic potential. Some potential prospects for CAR T cell treatment include:
CAR T-cell therapy’s future is marked by continuous innovation, with potential to transform cancer treatment and expand its use to other diseases.
Collaboration between academics, industry, and regulatory authorities is needed.
CLINICAL SUCCESS OF CAR-T CELL THERAPY:[27]
A patient at NCI suffering from advanced follicular lymphoma and patients at MSKCC with refractory CLL and relapsed B-cell ALL both demonstrated progress following second-generation CAR T cell therapy. A retroviral vector named MSGV was utilized to deliver a CD19 specific CAR as part of the treatment at NCI. This CAR was designed to target the CD19 protein found on the surface of B-lineage cells, using an anti-CD19 scFv derived from the murine monoclonal antibody FMC63. It incorporated both a CD3z endodomain and CD28 costimulatory endodomain. Following lymphodepletion, the patient two infusions of CAR T cells and eight doses of IL-2. As a result of this therapy, patient underwent selective elimination of B-lineage cells and achieved a partial remission of the lymphoma. Autologous CD19-targeted CAR T cells featuring the second-generation CAR (19-28z) were evaluated for safety and long-lasting effects in patients with B-ALL and CLL that had either relapsed or were resistant to chemotherapy in the MSKCC phase 1 trial. Patients who had previously received cyclophosphamide training exhibited a partial response, whereas those who had not been trained showed no measurable reactions to their disease.
When Dr. Carl June and his team at university of pennsykvania shared their findings that three adult patients suffering from advanced chronic lymphocytic leukaemia (CLL) achieved either complete or partial remission after undergoing CD19-specific CAR T cell therapy, it represented a major breakthrough in the application of CAR T cell therapy.
The construct utilized in this trial included the 4-1BB costimulatory endodomain, the CD3z signalling endodomain, and an anti-CD19 scFv derived from FMC63. An EF1-a promoter-driven lentiviral vector was employed to express this construct. Following injection, the CAR T cell counts in patients increased significantly, often by a factor of 1,000. These results enabled the treatment of advanced cases of CLL and other B-cell malignancies using second-generation CAR T cell therapy.
The outcomes of these clinical studies revealed that lymphodepletion prior to treatment-specifically a type of chemotherapy that reduces the immune cell count is essential for the success of CAR T cell therapy. Conversely, it appears that IL-2 is not necessary. Dr. steven Rosenberg’s team was the first to demonstrate that lymphodepleting chemotherapy is effective. They found that the combination of cyclophosphamide and fludarabine led to the in vivo growth and movement of injected tumour-reactive T cells toward tumour locations. The process of lymphodepletion might include reducing the count of native lymphocytes that compete with the infused T cells and increasing the circulating levels of T cell growth factors such as IL-15. This would promote more effective growth of the administered T cells within the host’s body.
FDA APPROVED CAR T CELLS THERAPIES:[28]
The US food and drug administration (FDA) has authorized CAR T-cell therapy for the treatment of multiple myeloma and certain types of leukaemia and lymphomas. Usually, CAR T-cell therapy is employed following the failure of conventional forms of treatment. Currently authorized CAR T-cell treatment include the following:
|
Generic Name |
Brand Name |
Target Antigen |
Targeted Disease |
Patient Population |
|
Tisagenlecleucel |
Kymriah |
CD19 |
B-cell acute lymphoblastic leukaemia (ALL)
B-cell non-Hodgkin lymphoma (NHL) |
Children and young adults with refractory or relapsed B-cell ALL
Adults with refractory or relapsed B-cell NHL |
|
Axicabtagene ciloleucel |
Yescarta |
CD19 |
B-cell non-Hodgkin lymphoma (NHL)
Follicular lymphoma |
Adults with refractory or relapsed B-cell NHL Adults with refractory or relapsed follicular lymphoma |
|
Brexucabtagene autoleucel |
Tecartus |
CD19 |
Mantle cell lymphoma (MCL)
B-cell acute lymphoblastic leukaemia (ALL) |
Adults with refractory or relapsed MCL
Adults with refractory or relapsed B-Cell ALL |
|
Lisocabtagene maraleucel |
Breyanzi |
CD19 |
B-cell non-Hodgkin lymphoma (NHL) |
Adults with refractory or relapsed B-cell NHL |
|
Idecabtagene vicleucel |
Abecma |
BCMA |
Multiple myeloma |
Adults with refractory or relapsed multiple myeloma |
|
Ciltacabtagene autoleucel |
carvykti |
BCMA |
Multiple myeloma |
Adults with refractory or relapsed multiple myeloma |
DIFFERENT TYPES OF CANCER ON WHICH CAR T CELL THERAPY ACTS:[29]
Since the U.S food and drug administration (FDA) initially authorized CAR T Cell therapy in 2017, the treatment has become accessible. Six iterations of CAR T cell therapy have been authorized by the FDA thus far to treat various forms of blood cancer, including:
APPLICATIONS OF CAR-T CELL THERAPY:[30]
Chimeric antigen receptor T-cell therapy (CAR T Cell therapy) is an immunotherapy method that uses the patient’s immune system to target and eliminate cancer cells. It requires genetic modification to express chimeric antigen receptors on cancer cells surface. CAR T cell therapy has shown remarkable results in treating certain cancers, particularly those with haematological malignancies. The following are some important clinical uses:
CONCLUSION:
CAR T Cell therapy is an FDA approved therapy that has Improved progression free survival for multiple myeloma, improved overall survival for large B-cell lymphoma and attained high rates of cancer remission for other hematologic malignancies such as ALL, Follicular lymphomas and mantle cell lymphoma
CAR T Cell therapy (Chimeric antigen receptor T-cell therapy) is a form of immunotherapy that involves modifying a patient’s T cells to attack cancer cells.
CAR T treatment for patients with tumors has shown promising outcomes, however many remaining challenges need to be considered.
CAR T Cell therapy shows breakthrough in cancer treatment like effective for certain hematologic malignancies and challenges such as toxicities (CRS, neurotoxicity), relapses, solid tumor, efficacy, accessibility and cost.
CAR T Cell therapy reveals ongoing efforts such as improving safety, expanding indications, enhancing efficacy, addressing manufacturing complexities and shows future directions like next-gen CAR’s, combination therapies, allogenic CAR T, solid tumor and showing potential impact on improving outcomes and focusing key areas such as mitigating toxicities, improving response durability, broadening patient access.
The future of CAR T cell therapy is bright, with continuing research and development targeted at overcoming present obstacles and increasing therapeutic potential and long term safety requires future study.
REFERENCES





Dr. Nagarjuna D, Dr. R. S Meghasri, Dr. Shivaraj D. R, Shrinivas Patil, Kavyashree D, Manu S. T, CAR T Cell Therapy: Current Challenges and Future Direction, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3920-3934. https://doi.org/10.5281/zenodo.18761526
 10.5281/zenodo.18761526
10.5281/zenodo.18761526
