Genba Sopanrao Moze College Of Pharmacy, Wagholi
One of the main causes of death from cancer and the most prevalent cancer among women worldwide is breast cancer. It results from the uncontrolled growth of breast tissue epithelial cells, which is frequently impacted by environmental, hormonal, and genetic variables. Patient outcomes have been significantly improved by early detection using screening techniques like mammography, ultrasonography, and molecular diagnostics. Family history, BRCA1/BRCA2 gene mutations, longer exposure to estrogen, lifestyle choices, and aging are risk factors. The many stages and A variety of therapies are required in various subtypes of breast cancer, including triple-negative, HER2-positive, and hormone receptor-positive breast cancer. Current treatments include immunotherapy, targeted therapy, chemotherapy, radiation, and surgery. modalities; tailored medicine is given priority to increase effectiveness and minimize side effects.
One of the most frequent cancers in women, breast cancer poses a serious risk to world health. It is differentiated by abnormal, insecure growth of breast cells and starts in The breast tissue, usually in The ducts (ductal cancer) or lobules (lobular carcinoma). Although it mostly effects women, breast cancer can strike men as well, but considerably less frequently. The World Health Organization (WHO) reports that, with millions of new cases each year, breast cancer has overtaken lung cancer as The most common disease diagnosed globally.
Genetic, hormonal, environmental, and psychological factors all play a role in The multifactorial growth of breast cancer. Known risk factors include family history, obesity, alcohol use, lack of movement, extended exposure to estrogen, and mutations in cancer suppressive genes including BRCA1 and BRCA2. Hormone receptor-positive (ER/PR+), HER2-positive, and triple-negative breast cancer (TNBC) belong to the subtypes of the disease; each has unique biochemical features, treatment responses, and prognoses
Treatments like hormone treatment, targeted therapy, chemotherapy, and radiation therapy, and immunotherapy are a few examples of multidisciplinary treatment techniques. Precision healthcare, which seeks to customize therapies based on the patient's genetic profile and the biological characteristics of the tumor, has gained interest in recent years. Despite These developments, treating drug-resistant and advanced-stage breast cancers—especially TNBC, which lacks targeted therapy options—remains difficult. Comprehensive care for breast cancer needs to tackle psychosocial factors such emotional distress, quality of life, and survivorship concerns in addition to medical interventions. Raising awareness, encouraging preventive actions, and boosting access to early detection and cutting-edge treatment choices are The main goals of global initiatives.
WHAT IS BREAST CANCER:
Everyone has known from ancient times that cancer is an incredibly horrible disease that can damage the entire body or kill an entire organ. It is becoming an increasingly common illness in both industrialized and developing nations. The cells in our body number in the billions. We need a microscope to see these cells because they are so small that we cannot see them with the naked eye. The tissues and organs that make up our bodies are composed of cells. Cancer right now refers to the stage in which cells develop out of control because of physical or chemical effects within the body. Normal cells get signals all the time that tell them whether to divide or differentiate into another cell.
CHARACTERISTICS OF BREAST CANCER:
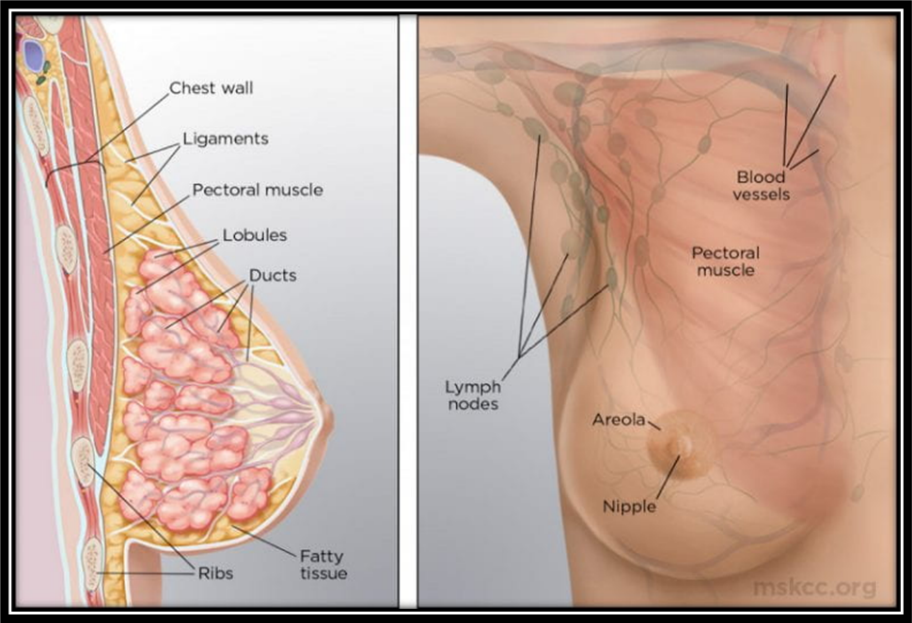
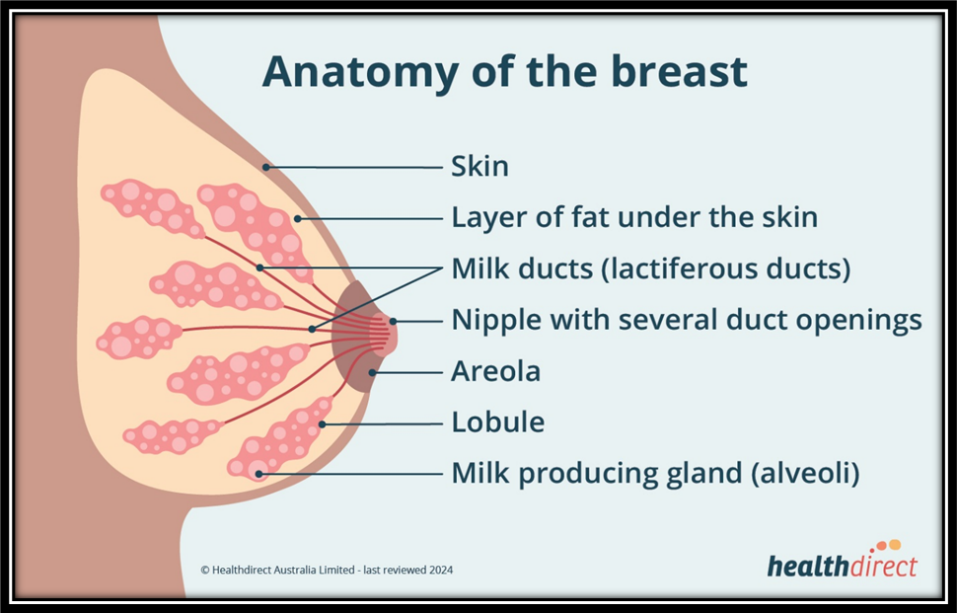
ANATOMY OF BREAST CANCER:
The glands on the front of the chest wall that produce milk are called the breasts in an adult woman. On either side of the sternum, they are connected by ligaments to the front of the chest wall and supported by the pectoralis major. There are 15–20 lobes in a circular pattern in each breast. The size and shape of the breast are determined by the fat covering the lobes. Many lobules make up each lobe, and at the end of each are glands that, in reaction to hormones, produce milk.
Mammography, ultrasound, breast magnetic resonance imaging (MRI), and breast-specific gamma-ray imaging are some of the imaging modalities that can be used to examine the anatomy of the breasts in both men and women. The rest of the article focuses on the female breast and describes breast anatomy and how it appears on different imaging modalities.
|
Sr.No. |
ORIGIN |
SITES |
|
1. |
Ductal Origin |
Milk Ducts |
|
2. |
Lobular Origin |
Lobules |
|
3. |
Nipple/ Areolar Origin |
Cells of the nipple, areola, usually within ducts. |
|
4. |
Connective tissue Origin |
Stroma, fibrous tissue, fat, blood vessels of the breast. |
|
5. |
Inflammatory breast cancer |
Arises from ductal cells but presents in dermal lymphatics of the skin. |
|
6. |
Metaplastic breast cancer |
Originates in epithelial cells but shows mixed features. |
DIFFERENT TYPES OF BREAST CANCER:
|
Sr. No. |
LOCATION |
CHARACTERISTICS |
|
1. |
Ductal Carcinoma |
|
|
|
a. Ductal Carcinoma in situ |
Non-Invasive. Abnormal cells are confined within the milk ducts. High chance of becoming invasive if untreated. |
|
|
b. Invasive ductal carcinoma |
Most common type. Cancer cells break through the duct walls. Can spread to lymph nodes & other organs. |
|
2. |
Lobular Carcinoma |
|
|
|
a. Lobular carcinoma in situ |
Not a true cancer but a risk factor. Abnormal cells confined within lobules. |
|
|
b. Invasive lobular carcinoma |
Starts in lobules & spreads to nearby tissue. Tends to affect both breasts more often than. |
|
Sr. No. |
SPECIAL HISTOLOGICAL VARIANTS |
CHARACTERISTICS |
|
1. |
Medullary Carcinoma |
Rare, soft, fleshy tumour with distinct borders. Often linked with BRCA1 mutations. |
|
2. |
Mucinous Carcinoma |
Produces mucus, which surrounds the cancer cells. Tends to have a better prognosis. |
|
3. |
Tubular Carcinoma |
Small, tube shaped structures. Usually slow-growing with good outcomes. |
|
4. |
Papillary Carcinoma |
Rare, finger-like projections. Seen more often in older women. |
|
5. |
Metaplastic Carcinoma |
Very rare, cancer cells change into different cell types. More aggressive. |
|
Sr. No. |
MOLECULAR |
CHARACTERISTICS |
|
1. |
Hormone receptor positive |
Driven by hormones. Responds well to hormone therapy. |
|
2. |
HER2 positive |
Overexpression of HER2 protein. More aggressive but treatable with targeted with drugs. |
|
3. |
Triple negative breast cancer |
Lacks ER, PR & HER2. More aggressive , higher recurrence risk. |
SUB-TYPES OF BREAST CANCER:
1) LUMINAL A:
Luminal A cancers are distinguished by lower expression of the cell proliferation marker Ki-67 (less than 20%), the presence of ER and/or PR, and the absence of HER2. Clinically, they have the greatest prognosis, are low-grade, slow-growing, and have a higher survival rate and a lower relapse rate. Chemotherapy is less beneficial against these cancers than hormonal therapy, such as tamoxifen or aromatic inhibitors.
2) LUMINAL B:
Luminal B malignancies are of higher grade and have a worse prognosis than Luminal A. They are ER positive, may be PR negative, and exhibit strong Ki67 expression (over 20%). They often have an intermediate to high histologic grade. Hormonal therapy may be useful for some cancers in addition to chemotherapy. Due to their raised Ki67, they grow faster than luminal A and have a worse prognosis.
3) HER2:
Since HER2-targeted therapy has improved the prognosis, 10–15% of breast cancers are HER2-positive, meaning they have no ER or PR and strong HER2 expression. The HER2-positive subtype of breast cancers grows faster and more quickly than luminal ones.
4) TNBC:
Triple-negative breast cancer has HER2, PR, and ER negative characteristics. About 20% of all incidences of breast cancer are of this type. Women under 40 and African-American women are most affected. Additional subgroups into which the TNBC subtype is further separated contain basal-like (BL1 and BL2), claudin-low, mesenchymal (MES), luminal androgen receptor (LAR), and immunomodulatory (IM); the first two are the most prevalent, usually comprising 50–70% and 20–30% of cases, respectively. Also, the phenotypes, clinical outcomes, and pharmacological sensitivities of each of them vary. Due to the tumor suppressor genes BRCA1 and BRCA2, TNBC causes 80% of breast cancer tumors and exhibits aggressive activity.
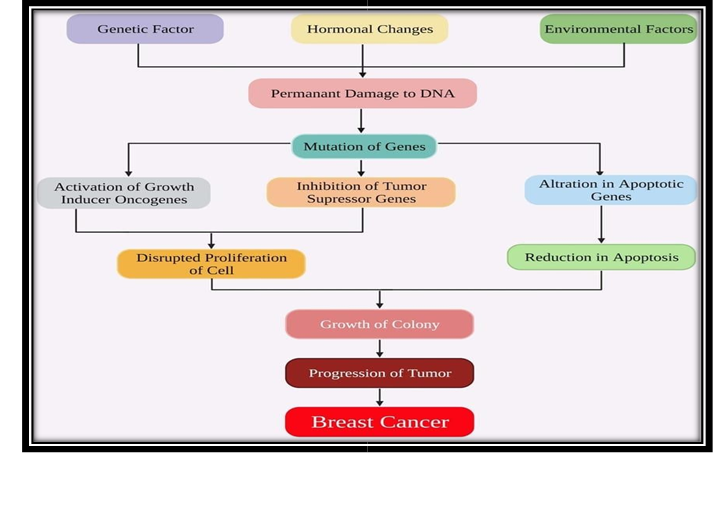
PATHOPHYSIOLOGY:
According to current research of the etiopathogenesis of breast cancer, invasive tumors develop as a result of a number of molecular changes that occur at the cell level. Breast epithelial cells with immortal characteristics and unchecked development are the result of these changes. The existence of various breast cancer subtypes with unique clinical and natural histories characteristics has been shown by genomic profiling. Although the precise number of disease subtypes and the molecular changes that give rise to them are yet unknown, they typically correspond with the presence or lack of the human epidermal growth factor receptor 2 (HER2), progesterone receptor (PR), and estrogen receptor (ER). This point of view on breast cancer, which sees it as a small group of distinct diseases with different molecular and cellular causes rather than as a collection of random molecular occurrences, has changed how breast cancer prevention, type-specific risk factors, and correlation, and has significantly influenced breast cancer research and treatment approaches. The following four primary subtypes of breast tumors, each with unique genetic and epigenetic abnormalities, are confirmed by data from The Cancer Genome Atlas Network (TCGA).
About 84% of all in situ illness is DCIS, or ductal carcinoma in situ, while the bulk of the remaining cases are lobular carcinoma in situ (LCIS). The broad category of proliferative lesions known as DCIS is limited to ducts and lobules and does not result in basement membrane invasion. While DCIS typically affects women, it can also occur in men. In DCIS, there is a very high chance of invasive tumors. Invasive cancer does not usually originate from preinvasive lesions. In situ lobular carcinoma (LCIS) originates in the lobular unit of the terminal ducts.
The lobular structure remains because LCIS has a more homogeneous look than DCIS. Cells usually grow in non-cohesive clusters due to a lack of the tumor-suppressive adhesion protein E-cadherin.
Although pregnancy must happen early in life, parous women have a lower lifetime risk of breast cancer than nulliparous women. Pregnancy's impact on cancer risk is additionally influenced by postpartum lactation, general parity, and family history. During involution during pregnancy and breastfeeding, the breast glands use Many of the same processes responsible for tissue remodeling that are stimulated when wounds heal.
DIAGNOSIS:
1. Mammography:
Mammography Diagnostic mammography creates a picture of the breast with modest doses of radiation. It serves to inquire into unexpected results from clinical breast exams or screening mammography. During a biopsy, difficulties can also be found using mammograms.
2. Ultrasonography:
An ultrasound uses high-frequency sound waves to produce images of different bodily parts. It is employed to identify if a breast bulge is a cyst or a solid tumor. Medical practitioners can also use ultrasonography to guide them to the biopsy site. To find out if liver metastases have occurred, patients with advanced breast cancer may have an ultrasound.
3. A biopsy:
The only accurate way to identify breast cancer is through biopsy. The purpose of a biopsy is to remove bodily tissues or cells of the patient for study in a lab. The pathologist's report will indicate whether or not the sample contained cancer cell. The type of biopsy carried will depend on whether the lump is palpable, meaning It is either palpable or not, means you cannot. The area to be tested may be located by the physician using ultrasound or mammography. Biopsies frequently occur in a hospital, and once they are complete, you can go.
4. The core biopsy:
makes use of a special hollow needle to remove tissue from the body. Physicians use it to take a sample from an area of the breast that they believe to be suspicious. They may collect many samples from the area throughout the process. Doctors sometimes employ a special vacuum to extract additional tissue through the hollow needle. It is called vacuum-assisted core biopsy.
TREATMENT:
The use of chemotherapy combined with cytotoxic drugs for both advanced and early-stage breast cancer has advanced significantly over the past 10 years, as indicated by several important studies that clearly indicate the survival benefits of more modern treatments. With recent developments, a literature review or decision-making algorithm alone cannot determine the optimal course of treatment for every patient. Most therapeutic decisions are based on established practices based on individual or group experience and local treatment history. New treatment targets could emerge as our understanding of the molecular biology of breast cancer develops.
2. RADIATION THERAPY:
According to current treatment trends, radiation therapy (RT) is still a crucial component of complex breast cancer therapy, which is determined by the patient's input as well as their risk status and the specific RT approach they choose. Radiation therapy clinical practice has not changed significantly as a result of results published in the three years since the third Breast Cancer Consensus Conference; yet, new scientific knowledge has led to the need to update and modify radiation therapy guidelines. In ductal carcinoma in situ (stage 0), radiation therapy (RT) following breast-conserving surgery (BCS) is recommended because it reduces the incidence of local recurrence (LR) by 50–60%.
3. IMMUNOTHERAPY:
There is a wide range of clinical symptoms and molecular subtypes of breast cancer, each with unique treatment outcomes and prognostic effects. It has long been believed that breast cancer is an immunologically "cold" malignancy that cannot be treated with immunotherapy. Immunotherapy, however, has been shown in recent years to be a successful treatment choice for a small number of patients. A variety of subtypes of breast cancer exist, from the most prevalent positive hormone receptor (HR+) type, known as human epidermal growth factor receptor 2 (HER2)-negative breast cancer, to the less common HER2-positive and triplenegative breast cancers (TNBC). This underscores the need for specific therapies that optimize patient outcomes.
4. HORMONE THERAPY:
Usually, hormone therapy (tamoxifen, an aromatase inhibitor (AI), or both) is administered if the malignancy is hormone receptor-positive. It can begin before to surgery; but, as it lasts for at least five years, it must also be administered following surgery.
5. TARGETED THERAPY:
After surgery, women with early-stage, HER2-negative, hormone receptor-positive breast cancer that has a tendency to recur can receive the targeted medication abemaciclib together with tamoxifen or an AI. After surgery, the targeted medication ribociclib administered with an AI is an additional choice for this patient group. In order to reduce the likelihood of cancer spreading, women with a hormone receptor-positive, HER2-negative tumor with a BRCA mutation that still has cancer in the tissue resected after surgery after neoadjuvant chemotherapy may be prescribed the targeted medication olaparib for a year. In this form, it can prolong the life of some women.
CONCLUSION:
In short, breast cancer continues to be the most prevalent cancer in women worldwide and a major contributor to cancer-related death. Despite its high prevalence, survival rates and quality of life have increased significantly due to advances in early identification, diagnostic methods, and multimodal therapies. Reducing the burden of disease is largely dependent on early symptom identification and timely mammography screening . Besides traditional surgery, chemotherapy, and radiation therapy, a more thorough understanding of the molecular and genetic causes of breast cancer has made it possible to create customized and targeted treatments. Results have changed with the rise of immunotherapy, HER2-targeted drugs, hormonal therapy, and genomic-guided treatment, in particular for aggressive subtypes like triple-negative and HER2-positive breast cancer.
Prognosis remains influenced by issues like late-stage presentation, recurrence, metastasis, treatment resistance, and unequal access to care, particularly in low- and middle-income nations. Public awareness, preventive measures, genetic counseling, lifestyle changes, and fair access to healthcare must therefore also be prioritized . In summary, breast cancer is a worldwide public health risk additionally to a medical illness. The war against breast cancer is gradually evolving from just surviving to a long-term cure and enhanced quality of life thanks to ongoing research, individualized therapy, and extensive patient support.
REFERENCES


Revati Latane, Jyoti Kolpe, Chitra Naik, Dr. Tushar Shelke, Breast Cancer: Pathophysiology and Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2195-2204. https://doi.org/10.5281/zenodo.17397972
 10.5281/zenodo.17397972
10.5281/zenodo.17397972
