Sree Chaitanya Institute of Pharmaceutical Sciences, LMD colony, Karimnagar, Telangana
Cardiovascular diseases (CVD's) contribute for the world’s leading cause of mortality and leads to health loss and excessive health care expenses. Cardiovascular disease is a term covers many diseases which affects heart or circulatory vessels. Risk assessment of cardiovascular diseases with traditional risk factors such as age, gender, blood pressure, smoking, lipids, Diabetes remained relatively fixed over the past decades. The purpose of FRS is to estimate the 10-year risk of growing cardiovascular diseases and CARRF-KL scale helps to assess knowledge about cardiovascular diseases in patients.A prospective observational study was performed on 133 patients in General Medicine Department. A questionnaire was designed to determine the cardiovascular risk by Framingham risk score and level of knowledge on CVD risk factors by using CARRF-KL scale. Data was analysed by using Odds ratio, Pearson Co-relation co-efficient. Statistics.In our hospital based observational study, collected data of 133 patients demonstrated that age, gender, alcohol, smoking are the common risk factors for CVD’s. We found that age >50yrs (51) patients at high risk 13, low and moderate risk 38. Males are at high risk (71) when compared to females (62) followed by Smoking (37), Alcohol (60), Diabetic (29), Hypertension (46) respectively. We also found that participants with High, Moderate, low knowledge are at cardiovascular risk. The overall study concluded that there is no relation between cardiovascular risk and knowledge. Patients with High and moderate, low knowledge
Cardiovascular diseases (CVD’s) continue to be the world’s leading cause of death and contribute to health care expenses. It is the crucial cause of death in all parts of India with the turn of the century. Cardiovascular disease is a term covers many diseases which affects heart or circulatory vessels which includes Hypertension, Angina Pectoris,Ischemic heart disease (IHD), Acute Myocardial Infarction (AMI), Atherosclerosis and Stroke. Risk assessment for cardiovascular diseases with traditional risk factors remained relatively fixed over the past decades (1).
EPIDEMIOLOGY:
CVD is a leading source of premature mortality accounting for 18.6 million deaths in 2019 worldwide. IHD & Stroke are top-ranking cause of global deaths accounting for 9.1 million & 6.5 million deaths in the year 2019. An estimate for 2030 shows that, CVD related mortality could be greater than 23 million globally (1). In India, addressing the significant burden requires understanding the complex dynamics underlying both biological and social determinants and their interactions are the reasons for high susceptibility to CVD, high mortality, and high premature mortality (1).

Fig. 01. Schematic representation of the unmodifiable and modifiable risk factors.
RISK FACTORS:
Table 01: Tabulation of Risk factor
|
NON-MODIFIABLE (22): |
MODIFIABLE (22): |
|
Age: increases the risk for Women of age, over 55years and Men over 45years are more vulnerable. |
Smoking: Significant independent risk factor. Quitting smoking significantly reduces risk. |
|
Sexual: Early in life, men are more at risk |
Diet: Risk increases having a diet rich in saturated fats, trans fats and sodium, A Mediterranean or DASH diet is recommended. |
|
Hormonal Changes: Postmenopausal women are at higher risk. |
Physical Inactivity: Lack of regular physical activity contributes to obesity and high blood pressure. |
|
Genetics: Premature CVD in the family (Men under 55 years, Women under 65years). |
Obesity: Central obesity (high waist-to-hip ratio) is a significant risk factor. |
FRAMINGHAM RISK SCORE SCALE
The Framingham heart consider has been a front-runner with the advancement of multi-variable measurable pattern to assess chance of coronary heart illness. These patterns are used to evaluate the effect of quantifiable, modifiable chance components and measures hazards of coronary heart diseases utilized over a predetermined period for following 10years for the improvement. This system defines an exertion to create accessible a device for clinicians to aid in their decision-making with respect to treatment, and helps in inducing patients towards solid conduct this framework is additionally promptly accessible to patients who can effectively assess their claim coronary heart infection’s chance and screen this hazard over time (2). Rules for the avoidance of coronary heart infections prescribe the utilize of chance scores to recognize grown-ups at higher hazard of CHD for whom preventive treatment by lipid bringing down drugs has higher supreme benefits (3). Since cardiovascular diseases are the leading cause of death worldwide, the FRS is the most widely used method for assessing the risk of CVD. Low risk individuals have a 10% or lower chance of developing coronary heart disease after 10yeras. 20% or more have high risk, whereas 10% to 20% have intermediate risk. (3). Each subject's age, gender, smoking status,
diabetes mellitus, systolic blood pressure, hypertension therapy, blood cholesterol, and high-density lipoprotein levels were used to determine their Framingham risk score(4). The concept of risk assessment and diminishment are the foundation in preventive cardiology practice. the Framingham heart study is considered as the milestone achievement that contributed a comprehensive knowledge on coronary heart disease risk prediction (4).
CARDIOVASCULAR DISEASE RISK FACTORS KNOWLEDGE LEVEL SCALE (CARRF-KL)
There are abundant risk factors contributing to the advancement of CVD but, a few of these risk components are modifiable (such as dyslipidaemia, hypertension, smoking, diabetes, lacking physical movement, and obesity), a few are non-modifiable (such as sex, age, race, hereditary predisposition). In spite of the fact that CVDs are not totally preventable, it is probability to diminish the threat of CVDs impressively by incorporating a healthy lifestyle (5). People may embrace a modern way of life by giving up a recognizable behaviour as it were upon having adequate knowledge level on the subject. It is detailed that the selection of healthy way of life behaviours may be low in patients with low knowledge level (6). Furthermore, the low level of knowledge around the disease may cause numerous negative circumstances such as inappropriate medication use, medication without indications, and expanded presentation to risk factors. Study says that patients with a low level of knowledge are more unsuccessful in portraying assault indications. In this case, it drags out the patients get to treatment and may antagonistically influence the victory of the treatment (7). Knowledge improving methods can contribute to reducing the risk by making a variation in patient to receive healthy way of life behaviours permanently (8). 10 In expansion, the disease-related information level of 2 patients having comparable illness characteristics may to change depending on individual beliefs, financial status, and social status (9). Subsequently, it is exceptionally vital to decide the current knowledge level of the patients and illuminate them about the required issues. The aim of study was to decide the knowledge levels of people appearing to cardiology outpatient clinic around risk factors for CVDs and the impacting variables. Cardiovascular disease is the one of the major causes of disabilities, high mortality and raising wellbeing care fetched in the world (9). CARRF-KL is used to degree knowledge levels around risk factors for CVDs. The scale created and evaluated for its validity and determined quality. Cardiovascular disease risk factors mindfulness and knowledge are accepted to be prerequisites for embracing wellbeing way of life practices the reason of study was to look at knowledge of CVD risk factors and risk recognition among people with high CVD risk (10).
METHODOLOGY:
STUDY DESIGN: Prospective, observational study.
SAMPLE SIZE: 133
STUDY SITE: Government District General Hospital, Karimnagar
STUDY DURATION: 6 months
INCULSION CRITERIA:
EXCLUSION CRITERIA:
STUDY PROCEDURE:
A data collection form is designed to collect the data which includes patient demographics, medication history, past medical history, social history, laboratory parameters (lipid profile), Blood pressure. Cardiovascular disease risk will be measured using the Framingham risk score scale, scoring will be based on standards of the scale providing the outcomes as either low /moderate/high.
Cardiovascular disease knowledge will be measured using the CVD risk factors knowledge level scale (CARRF-KL). Odd’s ratio, Pearsons’s co-relation statistics was analyzed for knowing the significance of study.Study was conducted by communicating with patients and their representatives, who met both inclusion and exclusion criteria, and data was collected by checking their previous medical records.
PRIMARY OUTCOMES:
To find out the cardiovascular disease risk and knowledge and to educate the patient in regard to assessment of risk of cardiovascular disease, and to provide knowledge on management of disease symptoms.
RESULTS:
Data was collected from 133 patients, at Government District General hospital from General Medicine Department. The following evaluation was made based on the collected data and it includes:
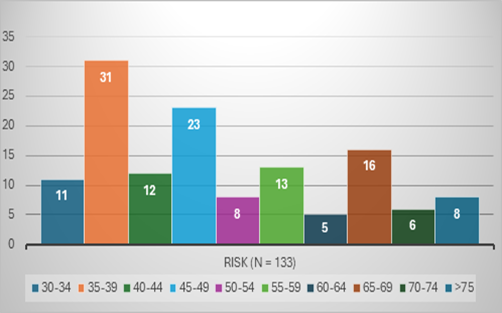
Graphical representation of patient’s data based on Age Group
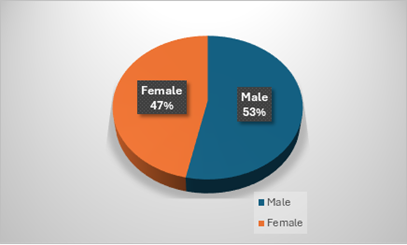
Graphical representation of patient’s data according to Gender Distribution
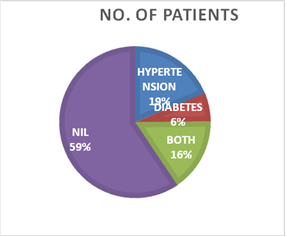
Graphical representation of patient’s data according to Past Medical History
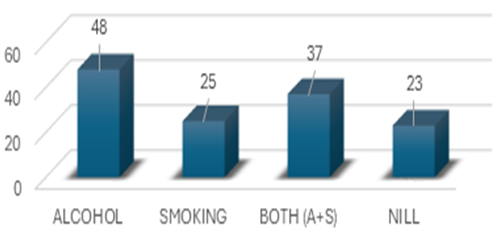
Graphical representation of patient’s data according to Social History
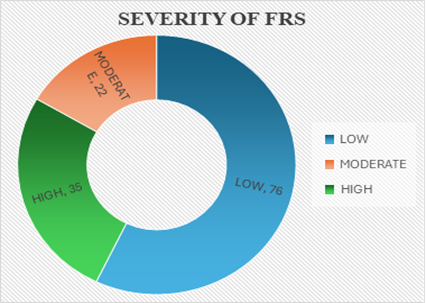
Graphical representation of patient’s data based on Framingham risk score.
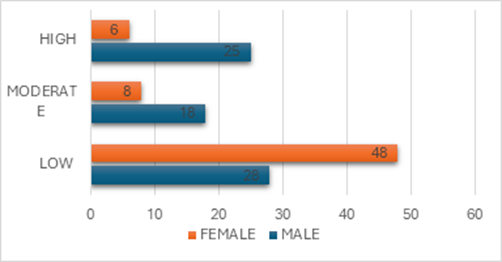
Graphical representation of patient’s data according to FRS based on gender
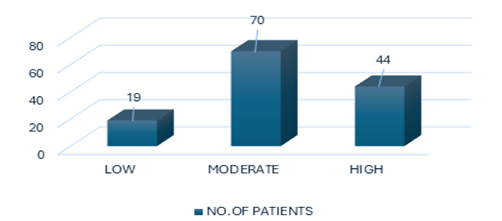
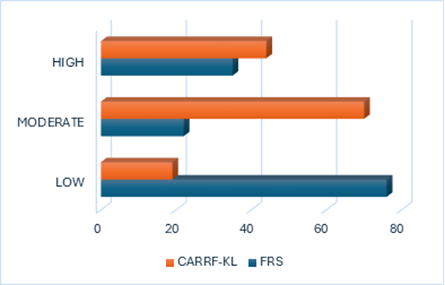
Graphical representation of patient’s data according to CARRF-KL scale
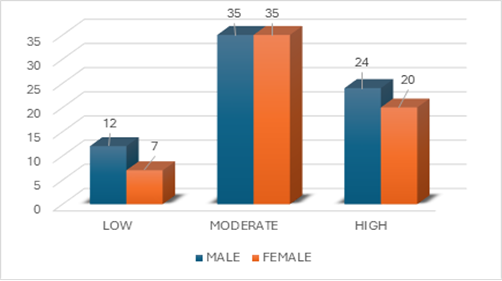
Graphical representation of patient’s data by using CARRF-KL scale based on gender
Graphical representation of patient’s data based on impact of Framingham risk score & CARRF-KL scale
ODDS RATIO:
OR =
Odds that the diseased were exposed (A/C) = AD
Odds the controls were exposed (B/D) BD
If OR = I both expected and outcome are same
If OR =>1 expected is greater than the outcome
If OR=<1 expected is lower than the outcome
Summarisation of patient’s data according to Odds Ratio
|
CHARACTERISTICS |
HIGH RISK |
LOW AND MODERATE |
ODDS RATIO |
|
Smoking Status |
|||
|
Smokers |
17 |
20 |
3.68 |
|
Non-Smokers |
18 |
78 |
|
|
Alcohol |
|||
|
Alcoholic |
21 |
39 |
2.26 |
|
Non alcoholic |
14 |
59 |
|
|
Diabetes |
|||
|
Diabetic |
23 |
6 |
29.38 |
|
Normal |
12 |
92 |
|
|
Hypertension |
|||
|
Hypertension |
27 |
19 |
14.03 |
|
Normal |
8 |
79 |
|
PEARSON CORRELATION COEFFICIENT:
Summarisation of patient’s data according to Pearson Correlation Coefficient
|
RISK |
NO. OF CANDIDATES |
KNOWLEDGE |
||
|
HIGH |
MODERATE |
LOW |
||
|
HIGH |
35 |
5 |
22 |
8 |
|
MODERATE |
22 |
4 |
12 |
6 |
|
LOW |
76 |
36 |
35 |
5 |
|
Pearson Correlation Coefficient (r) |
0.979012702 |
0.976824436 |
-0.584569 |
|
Upon submitting these value the p value obtained for high is 0.06 and for low and moderate is 0.03.
DISCUSSION:
Cardiovascular system consists of heart & its blood vessels, Numerous issues may come up with cardiovascular system. CHD is one of the most prevalent, non-communicable disease. Many factors can predispose to circulatory diseases, which include age, gender, increased blood pressure, high cholesterol, smoking, obesity, insufficient physical activities, the use of tobacco products & heavy alcohol.
This study was conducted on 133 patients with a duration of 6 months period to assess the Risk & knowledge of the Patients about the cardiovascular diseases in District Government Hospital, Karimnagar. FRS is a scale used to calculate the 10 years risk of cardiovascular diseases using elements such as Systolic Bp, lipid levels, social & past medical History.
In the present study the distribution of the risk of CVD in out of 133 participants low risk 76 patients (57.1%), moderate risk 22 patients (16.5%), and high risk 35 patients (26.3%) which is similar to the study conducted by Ashit Kumar Paul et.al which shows in which 290 subject participants 61.7% low, 18.6% intermediate and 19.7% high.
According to present study conducted the past medical history of the patients which hypertension, diabetes and both includes 25, 8, and 21 respectively which is similar to the study conducted by David John et al. and Ashitkumarpaul, Dilip Kumar das et al.
Males were predominantly in the moderate risk (18) and high risk (25) categories which is similar to the study conducted by Santi Susanti et.al who found that men had a higher risk of CVD compared to women. Similarly, Midhun Sasikumar et.al also found that males had a higher risk of CVD.
Out of 133 patients, >50years patients had high level of risk, similarly Santi Susanti et.al who observed that age is significantly contributed to higher FRS scores particularly in individuals age above 50. CVD risk factor knowledge level scale (CARRF-KL), is used to assess the knowledge about cardiovascular diseases.
In our study out of 133 patients, 71 males and 62 females were included. Males (18%) are having high knowledge when compared to females (15%) which is similar to the study conducted by Joseph Thomas et.al, which shows out of 693 participants 49.4% were males.
High risk FRS patients tended to have moderate (70) and high (44) knowledge levels suggesting that patients with perceived higher risk are informed but may lack actionable interventions which is similar to the study conducted by Nafiz et.al reported a correlation between higher CARRF-KL and higher FRS, similar to the study finding that high risk patients had better awareness but may not translate knowledge into action.
CONCULSION
This prospective observational study we demonstrated that age, gender, social history, past medical history are the major risk factors for CVDs. Participants aged above 50 years old are having high risk similarly male (53%). According to Framingham risk score low risk individuals are high (57.1%). we also found that participants with high moderate and low knowledge is having risk of cardiovascular diseases.
Our study concluded that the 133 patients revealed a significant distribution of CVD risk among patients, with a larger proportion of males in the higher risk category according to the Framingham risk score. A knowledge level scale about CV risk factors was prevalent among patients, with males showing slightly higher knowledge than females. The study also demonstrated that patients with high CVD risk were generally not co-related with level of knowledge about risk factors, which could reflect their pro-active attitude towards managing health.
The study emphasizes the importance of increasing awareness among the population. A clinical pharmacist plays a vital role in assessing individual risk, and focus on improving knowledge about lifestyle modifications and reducing liability of CVD by patient counselling.
REFERENCES



Raju Korra, Srinidhi Bongani, Gayathri Kamarapu, Anitha Enukonda, Rama Narsimha Reddy Anreddy, Association Between Health Knowledge and Framingham Score for CVD, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 2046-2056. https://doi.org/10.5281/zenodo.18318167
 10.5281/zenodo.18318167
10.5281/zenodo.18318167
