Swami Vivekanand College of Pharmacy, Udgir.
Brain tumors are a serious health problem around the world, and their number is increasing every year. India, being a large country, has many patients suffering from brain tumors. The rate of brain tumors in India is different in different regions and among different groups of people. Age, gender, income level, and where a person lives can affect how common brain tumors are in the country. Research and treatment for brain tumors in India are improving. Doctors and scientists are working on new methods like personalized medicine, targeted treatment, immunotherapy, and precision oncology to help patients more effectively. In summary, brain tumors are a big healthcare challenge in India. To deal with them, we need to understand how they occur, how to diagnose them, and how to treat them properly. Working together and using modern techniques can help improve patient care and quality of life.
Recent health data suggests that the number of brain tumor cases in India is increasing. This rise is adding to the country’s overall burden of brain tumor patients. Several reasons may explain this growth, such as changes in lifestyle, better medical facilities and diagnostic tools, longer life expectancy, and an expanding population. Together, these factors are leading to more people being diagnosed with brain tumors in India.
Today, many advanced imaging methods are available to help doctors identify and treat brain tumors. Modern MRI scans use special contrast agents, and PET scans use amino-acid-based tracers. Together, these techniques give radiologists clearer and more detailed pictures of tumors, helping them locate and measure tumors.
Brain tumors are the second most common type of cancer in children and young adults. Every year, about 215,000 children aged 0–14 years and around 85,000 teenagers aged 15–19 years are diagnosed with cancer worldwide. According to the International Agency for Research on Cancer, the number of brain tumor cases differs from country to country, ranging from 1.15 to 5.14 cases per 100,000 children. The rates also change depending on the ethnicity of the population.
Childhood brain tumors include different types of solid growths in the brain and are the leading cause of cancer-related deaths in children under 20 years. They make up nearly 25% of all childhood cancers. Worldwide data shows that both the number of cases and deaths from childhood brain tumors are higher in wealthier countries compared to developing countries
These tumors not only affect physical health but also emotional and mental wellbeing, which can lead to a poor quality of life.(1,6,7,8)
3. LITREATURE REVIEW
4. NEED OF THE STUDY
Brain tumors in children and young adults cause disproportionate long-term disability and mortality compared with many other illnesses of youth. Yet risk factors, early markers and vulnerable windows of exposure remain poorly consolidated across ages, tumor types and populations. A focused review that synthesizes what is known about environmental, genetic, perinatal and lifestyle risk factors—and highlights gaps and methodological challenges—will help clinicians, researchers and policymakers prioritize prevention, screening and research that targets the young.
5. AIM
To evaluate and summarize the potential risk factors, genetic predispositions, and environmental influences contributing to the development of brain tumors among the young population, and to identify preventive and early detection strategies.
OBJECTIVES
6. TYPES OF TUMORS
Brain tumors are growths that develop inside the brain due to cells growing in an abnormal and uncontrolled way. They are a mixed group of tumors, and each type grows and behaves differently. They also have different chances of survival and different treatment options. However, their symptoms, basic tests for diagnosis, and first steps of treatment are mostly similar for all types. Brain tumors can be classified in different ways, such as by the type of cell they come from, where they are located, how they behave, and their grade (how fast they grow). These classifications help doctors understand the type of tumor and how to treat it. Some important types of brain tumors include:
1. Gliomas
These tumors start from glial cells, which support and protect nerve cells in the brain. One very serious and fast-growing type of glioma is called Glioblastoma Multiforme (GBM). Gliomas can range from low-grade (slow-growing, less harmful) to high-grade (fast-growing, more dangerous) tumors.
2. Oligodendrogliomas
These tumors grow from oligodendrocytes, a type of glial cell. Another related tumor, called olingoastrocytoma develops from ependymal cells found in the brain’s ventricles or the spinal cord canal.
3. Meningiomas
These tumors form from the membranes (meninges) that cover and protect the brain and spinal cord. Most meningioma’s are non-cancerous (benign), but depending on their size and location, they can still cause symptoms by pressing on the brain.
4. Pituitary Tumors
These tumors form in the pituitary gland, the part of the brain that controls hormone production. Many pituitary tumors (pituitary adenomas) are benign, but they may affect hormone levels in the body. (the part of the brain that controls balance and coordination). They commonly occur in children. A similar type — previously called Primitive Neuroectodermal Tumor (PNET) — affects developing nerve cells / PNET Medulloblastomas are fast-growing tumors usually found in the cerebellum (the part of the brain that controls balance and coordination). They commonly occur in children. A similar type — previously called Primitive Neuroectodermal Tumor (PNET) — affects developing nerve cells(1,3,20)
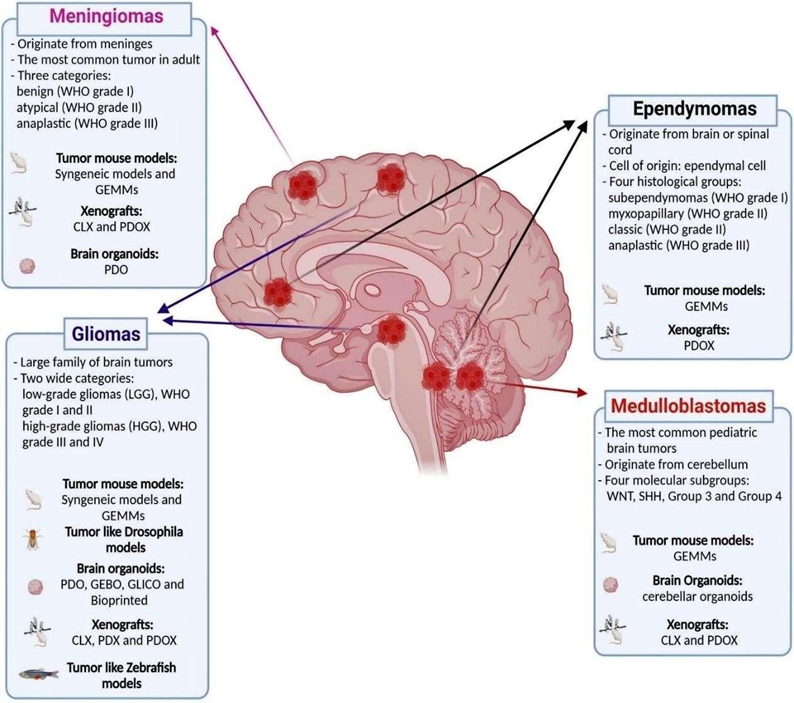
Fig 1: Brain Tumor Types
Location Of Tumor
The largest part of the brain; controls thinking, memory, speech, and movement. Tumors here may cause: Weakness on one side of the body, Speech or language problems, Seizures, Personality or behavior changes, Memory loss.
Located at the back of the brain; controls balance and coordination. Tumors here may cause: Difficulty walking or balancing, Dizziness, Poor coordination, Headache and vomiting
Connects the brain to the spinal cord; controls breathing, heart rate, vision, swallowing. Tumors here may cause: Difficulty speaking or swallowing, Double vision, Weakness or paralysis, Breathing or heart rate problems.
Tumors here may cause: Hormonal imbalance, Vision problems (especially peripheral vision loss),Growth abnormalities.
Deep in the brain; controls sleep cycle Tumors here may cause: Sleep disturbances, Problems with eye movement, Headache.
Tissue covering the brain (meningiomas). Symptoms include: Headache, Seizures, Vision changes
Especially near the ear or face (e.g., acoustic neuroma). May cause: Hearing loss, Ringing in ears, Facial numbness or weakness(12)
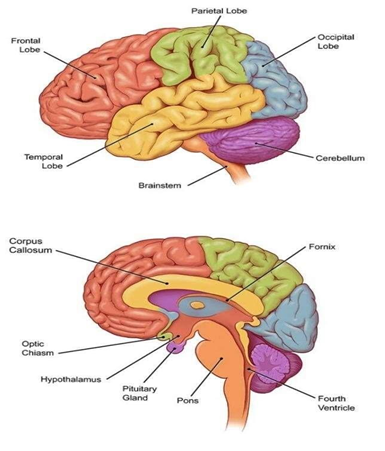
Fig 2: locations of tumor.
7. MECHANISM OF BRAIN TUMOR FORMATION
Normal brain cells acquire DNA mutations (due to heredity or external factors).These mutations affect key genes:Oncogenes get activated (promote cell growth) Tumor suppressor genes get inactivated (e.g., p53, PTEN) Result: uncontrolled cell division.
Growth signaling pathways (EGFR, PDGF, PI3K/AKT, RAS/MAPK) become overactive. Cells keep receiving ?grow and divide? signals even when unnecessary.
Checkpoints that control cell division fail. Tumor cells bypass apoptosis (programmed cell death).They accumulate instead of dying.
Tumor cells release VEGF and other factors. New blood vessels grow to supply oxygen and nutrients. Tumor grows rapidly due to enhanced blood supply.
Tumor cells secrete enzymes (MMPs) that break down surrounding tissue. They invade nearby brain structures. This makes surgical removal challenging.
Tumor cells suppress immune cells and produce inhibitory molecules. They avoid being recognized and destroyed by the immune system.
8. CAUSES OF BRAIN TUMOR
I. Genetic (Hereditary) Factors
Some people inherit abnormal genes from their parents that increase the risk of brain tumors. Example: Neurofibromatosis, Li-Fraumeni syndrome, Tuberous sclerosis
II. Radiation Exposure
Previous exposure to high-dose radiation, especially to the head, increases the risk. Example: Radiation treatment for childhood cancers
III. Age Factor
Brain tumors can occur at any age but are more common in children and older adults.
IV. Environmental Factors (less proven but suspected)
Some studies suggest certain environmental exposures may increase risk. Possible factors include: Exposure to harmful chemicals (e.g., pesticides, industrial chemicals), Air pollution, Ionizing radiation in the environment
V. Weakened Immune System
People with weak immune systems (e.g., HIV patients or those taking immunosuppressant’s) are at higher risk.
VI. Family History
If close family members have brain tumors, your risk may be slightly higher.(8,12)
Symptoms of Brain Tumor
Brain tumor symptoms can vary widely because they depend on the tumor’s size, type, growth rate, and location in the brain. As the tumor grows, it may press on nearby nerves, brain tissue, or block the flow of cerebrospinal fluid, leading to increased pressure inside the skull. This results in various physical, mental, and neurological changes.
General Symptoms These symptoms can occur regardless of the tumor’s location:
9. DIAGNOSIS OF BRAIN TUMOR
The diagnosis of brain and spinal cord tumors in adults involves several medical examinations and imaging techniques.
Vision and hearing, Walking patterns (gait), Muscle strength and reflexes
10. PATHOLOGY OF BRAIN TUMOR
Normal Brain Cells
↓
(Cells start changing due to DNA damage)
↓
Abnormal Cell Growth Begins
↓
Cells divide too fast & don’t die
↓
Formation of Tumor (Mass of abnormal cells)
↓
Tumor grows & presses on brain tissue
↓
↓ ↓ ↓ Effects ↓ ↓ ↓
Headache
Seizures
Weakness
Vision / speech problems
Memory issues
↓
Tumor spreads to nearby brain areas
( Some tumors can be spread through the cerebrospinal fluid)(1)
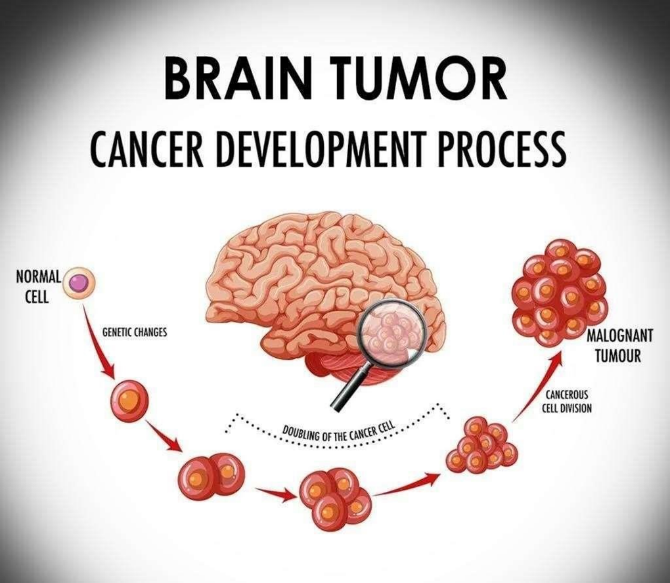
Fig3: Development of Brain Tumor
Pathogenesis Of Brain Tumor
a) IDH Mutation
Mutations in the isocitrate dehydrogenase (IDH1/2) genes are common in secondary glioblastomas. These mutations cause abnormal production of 2hydroxyglutarate (2-HG), an oncometabolite that drives tumor formation. Targeted drugs such as AG-120, AG-221, AG881, FT-2102, and IDH305 inhibit mutant IDH enzymes and are under clinical trials.
b) Notch Pathway
The Notch signaling pathway regulates cell differentiation and survival. Overactivation contributes to glioblastoma progression and resistance to therapy. Inhibitors of Notch signaling (like γ-secretase inhibitors and CB-103) show promise in reducing tumor growth and improving treatment response.
The enzyme acid ceramidase (ASAH1) converts pro-apoptotic ceramide into sphingosine-1-phosphate (S1P), which promotes cell survival. Overexpression of ASAH1 in glioblastoma reduces apoptosis and enhances tumor spread. ASAH1 inhibitors (like carmofur) can restore apoptosis and are potential therapeutic agents.
Vascular endothelial growth factor (VEGF) drives angiogenesis (formation of new blood vessels) to supply tumors with oxygen and nutrients. Blocking VEGF or its receptors (using agents like bevacizumab, sunitinib, or tivozanib) can restrict tumor blood supply.
Combination therapies are being tested to overcome resistance.
Platelet-derived growth factor (PDGF) promotes glioblastoma cell growth and survival via its receptor (PDGFR). Tumor cells often activate PDGF signaling through autocrine loops, leading to uncontrolled proliferation. Targeting this pathway can inhibit tumor growth.
EGFR is a receptor on cell surfaces that normally helps cells grow when growth factors bind to it. In glioblastoma, this receptor often becomes overactive due to gene amplification or mutations (like EGFRvIII). This makes tumor cells grow, divide, and spread uncontrollably.
PTEN is a tumor-suppressor gene that keeps cell growth under control. When PTEN is mutated or lost in glioblastoma, tumor cells grow faster and resist treatment. Research is trying to correct PTEN mutations and restore its function to slow tumor growth.
The SHH pathway controls cell growth and stem cell behavior. In glioblastoma, mutations keep this pathway permanently ?on,? leading to constant tumor cell growth and survival. Drugs that block this pathway—especially SMO inhibitors like vismodegib—are being tested in clinical trials.(15)
11. TREATMENT OF BRAIN TUMOR
For primary brain tumors, the most reliable treatment strategy usually begins with surgical removal of the tumor, followed by chemotherapy and radiotherapy. Surgery offers several benefits, such as maximum tumor excision, reduction of mass effect, decreased tumor load, improved diagnosis, and a better chance of long-term survival. However, brain tumor surgery can lead to a few complications. The most urgent concern after surgery is brain swelling (edema), while issues like infection, bleeding, and anesthesia-related reactions are less common.
To manage tumor-related edema, corticosteroids such as dexamethasone or prednisone are administered before and after surgery. Patients with larger tumors often present with elevated intracranial pressure and neurological deficits. Neurosurgical patients are also vulnerable to systemic problems such as hemodynamic instability, coagulation abnormalities, and metabolic disturbances. Mortality has been observed to be higher in children younger than 18 years of age.
1. Radiation Therapy (Re-written Version)
Advanced radiation techniques such as 3D-Conformal Radiation Therapy (3D-CRT), Intensity-Modulated Radiation Therapy (IMRT), and Proton Beam Therapy (PBT) help deliver radiation precisely to the tumor while protecting surrounding brain tissue.
3D-CRT uses MRI, CT, or PET imaging along with sophisticated computer technology to tailor radiation beams to the tumor’s exact shape. IMRT offers even greater precision by modulating radiation beam intensity with computercontrolled linear accelerators. Compared to these methods, Proton Beam Therapy is more accurate because protons can be focused precisely at the tumor site, sparing nearby healthy tissue; pencil-beam scanning further improves precision.
Common radiation-related side effects usually appear within 2–3 weeks and may include hair loss, skin irritation, headache, nausea, vomiting, hearing loss, loss of appetite, and cognitive difficulties. PBT patients may additionally experience fatigue, mood changes, depression, insomnia, and nausea.
2. Targeted Biological Therapy (Precision Medicine)
Certain targeted therapies work by blocking specific molecules involved in tumor growth. Two commonly used drugs in brain tumors are Bevacizumab (Avastin) and Everolimus (Afinitor). Bevacizumab is a monoclonal antibody that blocks VEGF-A, a key factor in tumor blood-vessel formation. It restricts VEGF binding to endothelial cell receptors, slowing tumor vascular growth. It is frequently used in glioblastoma Multiforme (GBM), especially after radiotherapy and Temozolomide. Avastin can be combined with drugs like irinotecan, carboplatin, and etoposide, though combination therapy does not show much added benefit. Side effects may include proteinuria, hypertension, fatigue, bleeding, headaches, diarrhea, and mouth sores.(1,3,5,8,10,12,17)
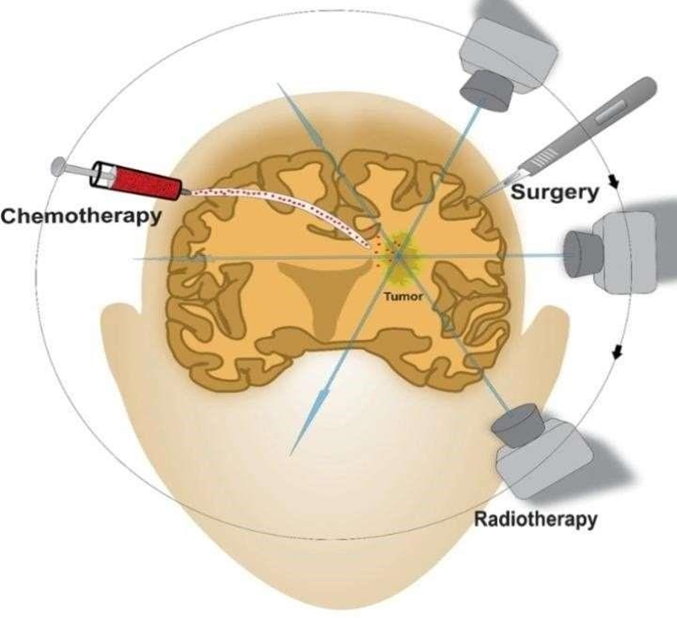
Fig4: treatment of tumor
12.FUTURE PROSPECTS
Despite major progress in understanding and managing brain tumors, several challenges remain in early detection, precise diagnosis, and effective treatment. Future research and clinical practice are expected to move toward a more personalized, targeted, and technologydriven approach.
Advances in genomics and proteomics will enable identification of novel molecular markers that can predict tumor behavior, treatment response, and prognosis. Integrating molecular profiling into routine diagnostics will help design personalized therapies.
AI-based imaging tools and predictive models are expected to revolutionize tumor detection, segmentation, and classification. Automated radiomics and machine learning algorithms can enhance diagnostic accuracy and treatment planning.
The future of brain tumor therapy lies in targeted molecular agents and immunebased treatments such as checkpoint inhibitors, CAR-T cell therapy, and oncolytic viruses. These approaches hold promise for improving survival with fewer side effects.
Overcoming the blood–brain barrier remains a key challenge. Nanoparticle-based drug delivery systems and novel carrier molecules may enhance the delivery of chemotherapeutic and gene-editing agents directly to tumor sites.
Gene-editing tools like CRISPR and the use of neural stem cells for regenerative therapy are emerging areas. These can potentially repair damaged neural tissues and selectively target tumor cells.
The combination of MRI, PET, and molecular imaging can provide real-time insights into tumor metabolism and microenvironment, enabling better surgical guidance and radiotherapy planning.
In developing countries like India, improved awareness, screening programs, and epidemiological surveillance are essential to detect brain tumors early and reduce mortality.
Global research collaborations and open-access clinical databases will help integrate large datasets, accelerating discoveries and standardizing treatment protocols. (18)
OBSERVATION
The review of existing literature indicates a rising concern regarding the incidence of brain tumors among the young population, including children, adolescents, and young adults. Studies consistently highlight that although brain tumors are relatively rare, they remain one of the leading causes of cancer-related morbidity and mortality in younger age groups
Environmental exposures such as ionizing radiation remain the most strongly supported risk factor across studies. However, increasing attention is directed toward potential associations with non-ionizing radiation (e.g., mobile phone use), although findings remain inconclusive. Genetic predisposition and hereditary syndromes are also observed to play a significant role in a subset of patients.
Another key observation from the literature is the variability in reported incidence rates across regions, likely influenced by differences in diagnostic capabilities, healthcare access, environmental conditions, and population genetics. Improvements in neuroimaging technologies over recent decades may also contribute to the apparent rise in detected cases. Despite extensive research, significant knowledge gaps persist regarding modifiable risk factors, lifestyle influences, and long-term environmental exposures.
Overall, the reviewed data suggest that while brain tumor risk in the young pulation remains relatively low, the potential influence of environmental, genetic, and technological factors warrants continued surveillance, targeted research, and improved public health strategies.
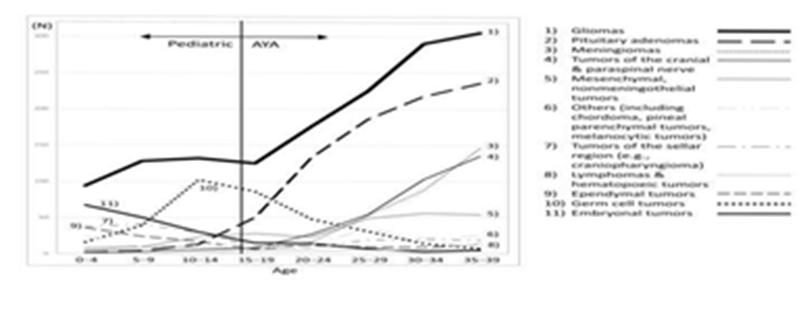
Fig 5: Age specific no. Of patiensts for each brain tumor at the brain tumor registry 2005-08 Japan
CONCLUSION
In India and across the world, brain tumors are becoming a major health issue because their cases are increasing over time. This growing problem is affected by factors such as a rising population, more elderly people, lifestyle changes, and differences in access to healthcare. A brain tumor is an abnormal growth in the brain that harms normal brain functions. In medical image processing, the goal is to find accurate and useful information with very few errors using computer algorithms. For detecting and classifying brain tumors in MRI scans, four main steps are used: preprocessing the images, segmenting the tumor area, extracting important features, and classifying the tumor type.In the future, tumor imaging will focus on better ways to combine and analyze images from different scans, along with new PET tracers. These improvements will be useful in advanced treatments like intensity-modulated radiotherapy and will help doctors plan radiotherapy more accurately for patients with brain tumors. In recent years, major advances in understanding the molecular features of pediatric brain tumors have improved how we diagnose and treat them. These developments support precision medicine, helping create more targeted therapies. As research grows, future WHO classifications will rely more on molecular markers than traditional histology. Next-generation sequencing continues to provide valuable insights into tumor types, patient characteristics, and treatment outcomes.
REFERENCES






Nikita Achintalwar, Dr. Ganesh Tolsarwad, Maheshwar S Mukta, Shaikh Sharmin, Vishwajeet Belkone, Supriya Bansode, Sheyash Bawage, Assessing the Risk of Brain Tumor in Young Population, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3906-3919. https://doi.org/10.5281/zenodo.18761408
 10.5281/zenodo.18761408
10.5281/zenodo.18761408
