1,3,4,6 Appasaheb Birnale College of Pharmacy, Sangli, Maharashtra-416416.
2 Gyanpeeth Rahul Dharkar College of Pharmacy & Research Institute, Karjat, Maharashtra- 410201
5 Women’s College of Pharmacy, Peth-vadgaon
Platelet aggregation plays a critical role in hemostasis but also contributes to thrombotic disorders, driving the need for effective and safe antiplatelet therapies. While conventional agents like aspirin and P2Y12 inhibitors are widely used, their long-term application is limited by adverse effects such as bleeding, gastrointestinal toxicity, and thrombocytopenia. This review explores the antiplatelet potential of four traditional medicinal herbs: ginger (Zingiber officinale), garlic (Allium sativum), turmeric (Curcuma longa), and onion (Allium cepa), focusing on their bioactive constituents, mechanisms of action, and comparative advantages over synthetic drugs. Ginger’s gingerol selectively inhibits arachidonic acid (AA)-induced aggregation by suppressing thromboxane A? (TXA?) synthesis. Garlic’s organosulphur compounds (e.g., allicin) modulate platelet membrane properties and calcium Signalling, while turmeric’s curcuminoids and turmerones target COX-1, 12-LOX, and shear-induced aggregation. Onion’s quercetin and thiosulfinates inhibit collagen-induced activation via cAMP and TXA? pathways. These herbs exhibit multitarget mechanisms, reducing thrombotic risk without significantly impairing hemostasis. Key findings highlight their synergistic effects, dose-dependent efficacy, and bioavailability challenges, particularly with curcumin. Clinical implications suggest their utility as adjuncts or alternatives to conventional therapy, though standardization and rigorous trials are needed. By integrating ethnopharmacological evidence with modern mechanistic studies, this review underscores the potential of these herbs in developing safer, natural antiplatelet strategies for cardiovascular disease prevention.
Platelets, also known as thrombocytes, are blood components primarily responsible for preventing bleeding by aggregating at sites of blood vessel injury to initiate clot formation. These are a nucleated cell fragments that originate from the cytoplasm of megakaryocytes in the bone marrow or lungs before entering the bloodstream. In healthy individuals, the platelet count typically ranges from 150,000 to 450,000 per microliter (μl) of blood.1 Under normal physiological conditions, platelets have a lifespan of approximately 8 to 10 days. Beyond their role in coagulation, platelets also participate in several other biological processes including inflammation, tumour progression, infection response, vascular repair, and maintenance of tissue homeostasis.2
Curcumin, chemically known as diferuloylmethane, is a naturally occurring polyphenol derived from the rhizomes of Curcuma longa (turmeric). It is widely used as a culinary spice, natural colouring agent, flavour enhancer, and a therapeutic agent in traditional Indian medicine. Curcumin has demonstrated significant medicinal potential, especially its anticoagulant properties, which have been confirmed in multiple studies. Research indicates that curcumin can inhibit platelet aggregation triggered by ADP, arachidonic acid (AA), and collagen.2
The rhizome of ginger has long been utilized in various traditional medicinal systems. Research highlights that its active ingredients—gingerol and shogaol—offer numerous therapeutic benefits, such as anti-inflammatory, antioxidant, and lipid-lowering effects. Experimental data show that ginger can suppress platelet aggregation initiated by arachidonic acid, epinephrine, ADP, and collagen, with the strongest inhibitory effect noted against AA-induced aggregation.3
Garlic (Allium sativum), widely used since ancient times in traditional medicine across different cultures, is recognized for its antioxidant activity and cardiovascular benefits, including the prevention of atherosclerosis and the reduction of blood pressure and plasma cholesterol levels. Both raw garlic and its various preparations—such as aqueous extracts, garlic oil, aged garlic extract, and garlic powder—have been shown to modulate platelet aggregation in both in vitro and in vivo settings. The bioactive effects of garlic are mainly attributed to its volatile Sulphur -containing compounds, especially thiosulfates, which also give garlic its distinct smell.4
Onion (Allium cepa), a member of the Amaryllidaceae family, is reported to provide several health advantages, including anticancer, antiplatelet, and antithrombotic effects. Onion extracts have been observed to inhibit platelet aggregation induced by several agonists, such as ADP, AA, and collagen. Specifically, onion.5
3. PLATELET ACTIVATION AND AGGREGATION:
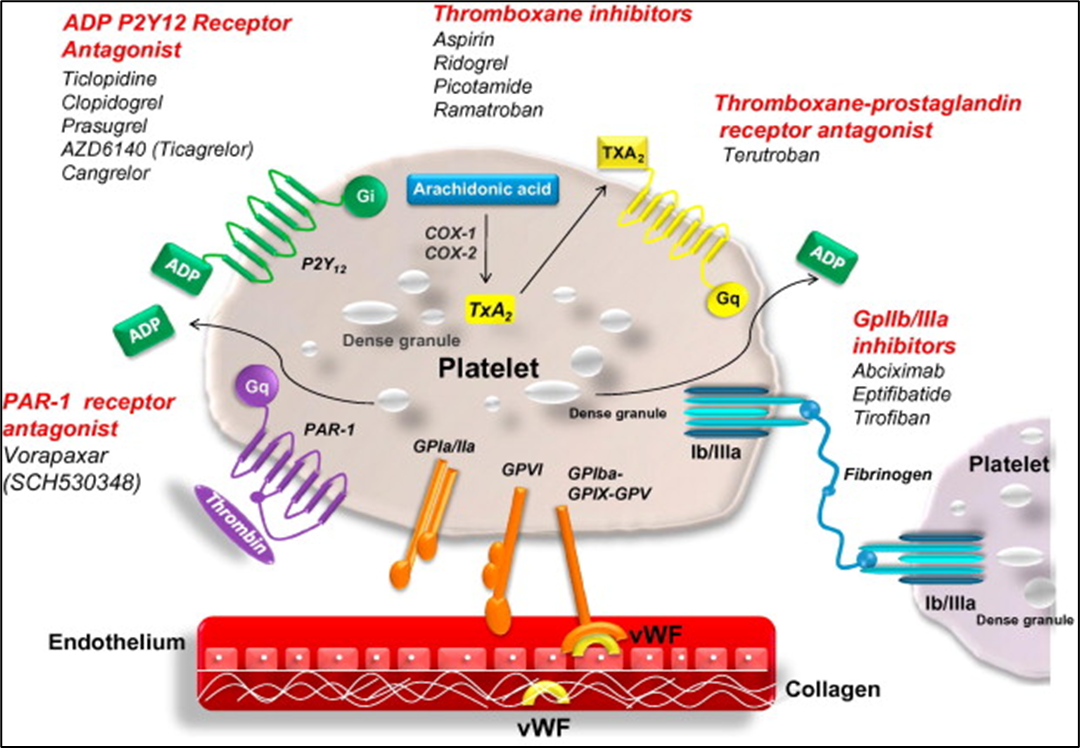
Fig.1: Platelet activation – an overview
Platelets play a fundamental role in initiating the coagulation cascade, primarily through their activation and aggregation. The process of primary haemostasis begins when platelets adhere to the exposed extracellular matrix at the site of vascular injury. Under high shear stress conditions, von Willebrand factor (vWF) facilitates platelet adhesion by acting as a bridge between exposed collagen and the platelet glycoprotein (GP) Ib-IX-V receptor complex. Additionally, collagen directly interacts with platelet GP Ia/IIa and GP VI receptors. As platelets become activated, they undergo shape changes and release the contents of their granules. A key step in aggregation involves the activation of the GP IIb/IIIa receptor, which binds fibrinogen or vWF, thereby linking adjacent platelets and stabilizing the forming thrombus. Platelet activation is further driven by secreted platelet factors and local prothrombotic agents, including tissue factors, through various Signalling pathways. Soluble agonists such as ADP, thromboxane A2 (TxA2), and thrombin released from activated cells, stimulate platelets mainly via G-protein-coupled receptors (GPCRs). TxA2, a lipid mediator within the eicosanoid family, is synthesized from arachidonic acid through the enzymatic actions of phospholipase A2, COX-1/COX-2, and thromboxane synthase (TXAS). ADP released from damaged endothelial cells and activated platelets binds to the P2Y1 and P2Y12 GPCRs on platelets, amplifying activation and triggering additional ADP release. The P2Y12 receptor is especially critical for maintaining platelet activation in response to ADP. Similarly, TxA2 produced by activated platelets further enhances platelet activation via GPCRs, contributing to the formation of the platelet plug. Thrombin, the most powerful platelet activator, also plays a central role in converting fibrinogen into fibrin, reinforcing the platelet plug. It activates platelets through protease-activated receptors (PARs), which are also GPCRs found on the platelet surface. All these Signalling mechanisms ultimately lead to the activation of integrin adhesion receptors, particularly GP IIb/IIIa. This integrin's activation allows the binding of fibrinogen or vWF between platelets, driving aggregation and the recruitment of more platelets to the injury site, culminating in thrombus formation.6
4. CURRENTLY AVAILABLE ANTIPLATELET AGENTS AND THEIR DRAWBACKS:
Patients with diverse atherosclerotic illnesses can be treated with aspirin, a currently available antiplatelet drug. It works by preventing the COX-1 enzyme from being activated, which prevents the formation of TxA2 from arachidonic acid. Aspirin has greater effectiveness in venous thrombosis than in the prevention of arterial thrombosis.7
Ticlopidine and clopidogrel are prodrugs. These irreversibly bind and inhibit the P2Y12 receptor for the lifespan of the platelet7
The FDA first licensed a GP IIb/IIIa antagonist, abciximab, in 1994 for the treatment of ischemic problems following angioplasty.
The majority of administered abciximab forms a strong but not permanent bond with GP IIb/IIIa on platelets, inhibiting platelet aggregation.7
5. TRADITIONAL MEDICINAL HERBS AS A REMEDY FOR PREVENTING PLATELET AGGREGATION:
Zingiber officinale (ginger), a herbaceous perennial belonging to the family Zingiberaceae, has been traditionally used for culinary and medicinal purposes across various cultures, particularly in Southeast Asia. The pungent rhizome of ginger contains a rich array of bioactive constituents, including gingerol, shogaol, and zingiberene, which have been shown to possess anti-inflammatory, antioxidant, and cardiovascular protective effects.13
Among its active constituents, gingerol has been widely studied for its role in inhibiting platelet aggregation. In in vitro experiments, gingerol demonstrated a concentration-dependent inhibition (0–20 μM) of platelet aggregation induced by arachidonic acid (AA) and collagen. Notably, it did not affect aggregation pathways activated by platelet-activating factor (PAF), thrombin, or the thromboxane receptor agonist U46619. These findings indicate a selective mechanism of action, likely mediated through the AA metabolic cascade. Gingerol significantly suppressed the synthesis of thromboxane B? (TXB?) and prostaglandins (PGs) such as PGE?, PGD?, and PGF?α. It also completely inhibited AA-induced phosphoinositide breakdown, a critical Signalling step in platelet activation. However, this inhibitory effect was not observed with collagen-, PAF-, or thrombin-induced phosphoinositide responses, even at concentrations as high as 300 μM.14
In studies utilizing human platelet-rich plasma, gingerol and the cyclooxygenase inhibitor indomethacin both inhibited secondary aggregation and ATP release in response to adenosine diphosphate (ADP) and adrenaline. Importantly, neither compound affected the primary aggregation response, suggesting that the mechanism involves modulation of feedback amplification rather than initial platelet activation. The maximal antiplatelet effect occurred after a 30-minute incubation period and was fully reversible upon removal of gingerol.15, 16
Phytochemical analysis of ginger rhizomes has led to the isolation of twenty-nine distinct compounds, many of which exhibit antiplatelet and vasodilatory properties. Thin-layer chromatography (TLC)-separated bands from ginger extract were shown to inhibit thromboxane formation while increasing lipoxygenase products, supporting a redirection of AA metabolism. The combined action of gingerol, zingiberene, and related constituents is believed to underlie ginger’s pharmacological effects, indicating a synergistic mechanism rather than the activity of a single agent. 17
The consistent correlation between the inhibition of platelet aggregation and suppression of thromboxane synthesis underscores ginger's therapeutic potential in cardiovascular protection, particularly as an antithrombotic agent. However, the optimal dose, formulation, and standardization of ginger preparations remain to be fully established. Variability in extraction methods and bioavailability may influence efficacy and safety, highlighting the need for further clinical trials and pharmacokinetic studies. Ginger, particularly through its active compound gingerol, exhibits potent and selective antiplatelet effects primarily via inhibition of thromboxane synthesis and modulation of arachidonic acid metabolism. These properties, coupled with its traditional use and low toxicity profile, position ginger as a promising candidate for adjunctive therapy in the prevention of thrombotic disorders. Future research should aim to standardize preparations and validate efficacy in clinical settings.
Garlic (Allium sativum L.), a member of the onion family Alliaceae, has been traditionally used for its medicinal properties, particularly in cardiovascular health. Recent studies have focused on its antiplatelet effects, positioning garlic as a potential complementary therapy in managing cardiovascular diseases (CVDs).18, 19
A synergistic inhibitory effect has also been noted when garlic is used in combination with multiple platelet agonists. Although promising, the precise biochemical mechanisms underlying these synergistic effects remain to be elucidated.21
ii. Comparative Effects of Garlic Preparations: Studies comparing Allium sativum and Allium ursinum reveal similar antiplatelet effects, particularly against ADP-induced aggregation. Garlic oil has shown a dose-dependent inhibition of platelet aggregation induced by AA, adrenaline, collagen, and calcium ionophores. The pharmacokinetics and efficacy of garlic preparations can vary significantly depending on the formulation and concentration of organosulphur compounds.22
iii. Clinical Observations and Herb-Drug Interactions: A substantial number of cardiovascular Patients report using garlic supplements alongside conventional medications, often noting subjective improvement in symptoms. However, clinical data indicate a potential for adverse effects, particularly when garlic is combined with antiplatelet drugs such as aspirin and clopidogrel. These interactions have been associated with:
These findings underscore the importance of cautious integration of garlic supplements into therapeutic regimens and the need for healthcare providers to counsel patients on potential risks.19 Garlic presents a promising adjunct in the management of platelet aggregation and cardiovascular health. However, its concurrent use with antiplatelet medications requires careful consideration due to the risk of adverse hematological effects. Further research is necessary to understand the long-term safety, efficacy, and mechanisms of herb-drug interactions involving garlic. Clinical practitioners should ensure thorough patient education and regular monitoring when incorporating herbal therapies into cardiovascular treatment plans.
Curcuma longa (turmeric), a perennial herb of the Zingiberaceae family, has long been used in traditional medicine for its antioxidant, anti-inflammatory, and antimicrobial properties. Its pharmacologically active constituents—curcumin, turmerone, and ar-turmerone—have demonstrated significant potential in the inhibition of platelet aggregation and thrombosis.
Multiple in vitro studies have shown that ar-turmerone, turmerone, and curcumin inhibit platelet aggregation induced by ADP, arachidonic acid (AA), collagen, and platelet-activating factor (PAF), with ar-turmerone exhibiting the strongest effect. The hexane extract of C. longa rhizomes, enriched in ar-turmerone, potently inhibited collagen-induced aggregation (IC??: 1.2 µM), surpassing even aspirin in efficacy. Its mechanism likely involves interference with the cyclooxygenase (COX) pathway, though further mechanistic studies are warranted.23,24
Due to their poor solubility and stability, curcuminoids (curcumin, demethoxycurcumin [DMC], and bisdemethoxycurcumin [BDMC]) have limited bioavailability. A water-dispersible formulation (curcumin:DMC:BDMC = 2:1:3) improved solubility and doubled the potency in inhibiting platelet aggregation (IC??: 10–25 µg/mL). These curcuminoids modulated multiple pathways:
Cyclocurcumin, a minor compound in C. longa, selectively inhibited shear-induced platelet aggregation (SIPA), a key event in pathological thrombosis (e.g., atherosclerosis). Unlike traditional antiplatelet agents, cyclocurcumin:
This selectivity suggests cyclocurcumin could be a safer therapeutic option for thrombotic conditions with reduced bleeding risk.26
Although C.oil did not protect against myocardial ischemia-reperfusion (MI/RP) injury, it exhibited potent antiplatelet effects:
Its major constituents ar-turmerone, α, β-turmerone, and curlone displayed favourable pharmacokinetics, including good oral absorption and sustained plasma levels. Notably, the antithrombotic effect appears platelet-specific, with no changes in coagulation parameters (TT, PT, aPTT).27
Onion (Allium cepa), a biennial herbaceous plant from the Amaryllidaceae family, is widely recognized for its therapeutic properties, particularly its antiplatelet activity (AA). The key bioactive constituents responsible for this activity include organoSulphur compounds (e.g., allyl propyl disulfide and thiosulfinates) and flavonoids such as quercetin and its glucosides.
Multiple mechanisms underlie the antiplatelet effects of onion:
The antiplatelet efficacy of onions is influenced by varietal differences and cooking methods:
The physical form (whole, quartered, or crushed) and cooking technique (convection oven vs. microwave) critically impact AA:
Notably, prolonged heating can not only reduce AA but may also induce pro-aggregatory effects, possibly due to the persistence of heat-tolerant platelet-stimulant compounds like prostaglandins, especially when AA compounds are degraded.28 Onions exhibit strong antiplatelet and antioxidant activities, driven by both organosulphur compounds and flavonoids. However, heat processing significantly diminishes these effects, especially under high or uniform heating conditions. For maximum cardiovascular benefits, onions should be crushed and consumed raw or stir-fried briefly without water to preserve bioactivity. These findings underline the critical role of food preparation in maintaining the therapeutic potential of Allium vegetables and support their use as functional foods for cardiovascular health.
Table No.1: Active constituents of TMHs.
|
Sr. no |
Kingdom
|
Order |
Family |
Scientific name |
Active compound |
Result |
Ref. |
|
1.
|
Plantae |
Zingiberales |
Zingiberaceae |
Zingiber officinale |
Gingerol |
Inhibition of AA-induced platelet aggregation. |
14, 17 |
|
Zingiberene |
|||||||
|
2. |
Plantae |
Asparagales |
Amaryllidaceae |
Allium sativum |
Diallyl thiosulfinate (Allicin), |
Inhibited platelet aggregation induced by AA, collagen, adrenaline & Ca++ ionophore. |
18,19, 20,21, 22 |
|
Diallyl disulfide (DADS) & |
|||||||
|
Diallyl trisulfide |
|||||||
|
3. |
Plantae |
Zingiberales |
Zingiberaceae |
Curcuma longa |
Turmerone |
Inhibition of platelet aggregation induced by collagen & AA. |
23,24 |
|
Curcumin |
Inhibition of platelet aggregation induced by PAF, AA & Calcium. |
||||||
|
4. |
Plantae |
Asparagales |
Amaryllidaceae |
Allium cepa |
Allyl propyl disulfide |
Inhibited platelet aggregation induced by Collagen & ADP |
26, 27 |
|
Quercetin |
Inhibited platelet aggregation induced by Collagen |
29 |
DISCUSSION:
The increasing prevalence of cardiovascular diseases (CVDs) and thrombotic disorders has necessitated the exploration of alternative and complementary therapeutic strategies. Conventional antiplatelet agents, such as aspirin, P2Y12 inhibitors, and GPIIb/IIIa antagonists, remain the cornerstone of thrombosis prevention. However, their long-term use is often associated with significant adverse effects, including gastrointestinal bleeding, thrombocytopenia, and immune suppression. This review highlights the potential of four traditional medicinal herbs—ginger, garlic, turmeric, and onion—as natural antiplatelet agents with promising efficacy and a favorable safety profile.
Mechanistic Insights into Herbal Antiplatelet Activity:
The antiplatelet mechanisms of these herbs are diverse and involve multiple pathways:
Ginger (Zingiber officinale) primarily exerts its effects through gingerol, which selectively inhibits arachidonic acid (AA)-induced platelet aggregation by suppressing thromboxane A2 (TXA2) synthesis and phosphoinositide breakdown. Its reversible action and synergistic interactions with other bioactive compounds enhance its therapeutic potential without significant toxicity.
Garlic (Allium sativum) contains organosulphur compounds, such as allicin and thiosulfinates, which modify platelet membrane properties, inhibit AA metabolism, and interfere with calcium Signalling. However, its concurrent use with conventional antiplatelet drugs may increase bleeding risk, necessitating cautious clinical integration.
Turmeric (Curcuma longa) demonstrates potent antiplatelet activity through curcuminoids (curcumin, demethoxycurcumin, bisdemethoxycurcumin) and turmerones, which suppress COX-1, 12-LOX, and TXB2 production. Cyclocurcumin, a lesser-known constituent, shows selective inhibition of shear-induced platelet aggregation, offering a novel approach to targeting pathological thrombosis without impairing normal hemostasis.
Onion (Allium cepa) contains quercetin and organosulphur compounds that inhibit collagen-induced aggregation by modulating intracellular calcium, cAMP, and TXA2 synthesis. However, its antiplatelet activity is highly dependent on processing methods, with raw or minimally processed forms (e.g., stir-fried) retaining maximal bioactivity.
Comparative Advantages Over Conventional Antiplatelet Drugs:
Unlike synthetic antiplatelet agents, these herbal alternatives exhibit:
CONCLUSION:
Traditional medicinal herbs ginger, garlic, turmeric, and onion offer a promising, naturally derived approach to antiplatelet therapy. Their multi-mechanistic actions, favorable safety profiles, and additional cardiovascular benefits position them as potential adjuncts or alternatives to conventional antiplatelet drugs. However, their clinical translation requires rigorous standardization, bioavailability enhancement, and further human trials to validate efficacy and safety. Integrating these herbs into evidence-based cardiovascular care could pave the way for more holistic and personalized thrombosis prevention strategies, minimizing the limitations of current pharmacotherapies. Future research should focus on optimizing formulations, elucidating molecular mechanisms, and assessing long-term outcomes in at-risk populations.
REFERENCES




Vaishnavi Kumbhar, Shweta Dangat, Dr. P. L. Ladda, Dr. N. S. Naikwade, Shruti Dilpak, Prathamesh Kurane, Antiplatelet Activity of Traditional Medicinal Herbs: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 4226-4237. https://doi.org/10.5281/zenodo.15736294
 10.5281/zenodo.15736294
10.5281/zenodo.15736294
