Department of Pharmacy, Ranchi College of Pharmacy, Ranchi, Jharkhand -8340010.
Antibiotics have been a cornerstone of modern medicine since their discovery, transforming the treatment of bacterial infections and significantly reducing mortality and morbidity worldwide. However, the effectiveness of these life-saving drugs is increasingly threatened by the growing problem of antibiotic resistance. Antibiotic resistance occurs when bacteria evolve mechanisms to withstand the drugs that are designed to kill them. This phenomenon is accelerated by the misuse and overuse of antibiotics in human medicine, veterinary practice, and agriculture. Antibiotic stewardship refers to a coordinated set of strategies aimed at improving and measuring the appropriate use of antibiotics. The goal is to optimize clinical outcomes while minimizing unintended consequences, such as the development of resistance, adverse drug reactions, and increased healthcare costs. Effective stewardship ensures that patients receive the right antibiotic, at the right dose, for the right duration, and only when necessary. With the discovery of penicillin, antibiotics are a critical part of global health, including cancer chemotherapy and advanced surgical procedures. Antimicrobial agents are not like other drugs. They are unique in that both the individual patient and the broader society bear the consequences of their use with each prescription. The antimicrobial effect that saves lives also exerts.
Antibiotic Resistance
Antibiotic resistance is a complex biological and ecological phenomenon where bacteria develop the ability to survive exposure to antibiotics that would normally kill them or inhibit their growth. This resistance can be intrinsic (naturally occurring in certain bacterial species) or acquired (through mutation or horizontal gene transfer from other bacteria).
Mechanisms of resistance include:
Resistance can develop rapidly and spread within and between bacterial species. One of the most alarming aspects is the horizontal transfer of resistance genes via plasmids, transposons, and integrons, enabling bacteria to share genetic material and create multidrug-resistant organisms.
Factors contributing to the acceleration of antibiotic resistance include:
Antibiotic resistance has profound implications for public health:
The World Health Organization (WHO) has declared antimicrobial resistance (AMR) as one of the top ten global public health threats. Without urgent and sustained action, we risk entering a "post-antibiotic era" where even minor infections could become deadly.

Key Principles of Antibiotic Stewardship
Effective antibiotic stewardship is based on several core principles. First and foremost is the principle of appropriate antibiotic use, which entails prescribing antibiotics only when there is clear evidence of a bacterial infection. Viral infections, such as the common cold or influenza, do not respond to antibiotics and should not be treated with them. Another critical principle is the selection of the right antibiotic. This involves choosing an agent that is effective against the suspected or confirmed pathogen, has the narrowest possible spectrum of activity, and is associated with the least risk of adverse effects. Dosing and duration of therapy should be optimized based on the patient's clinical status, site of infection, and pharmacokinetic/pharmacodynamic considerations. Monitoring and reviewing antibiotic use is also essential. This includes tracking resistance patterns, auditing prescribing practices, and providing feedback to prescribers. Education and training for healthcare providers, patients, and the public are fundamental components of stewardship, fostering awareness and promoting responsible behavior.
Function / Role of Antibiotic Stewardship
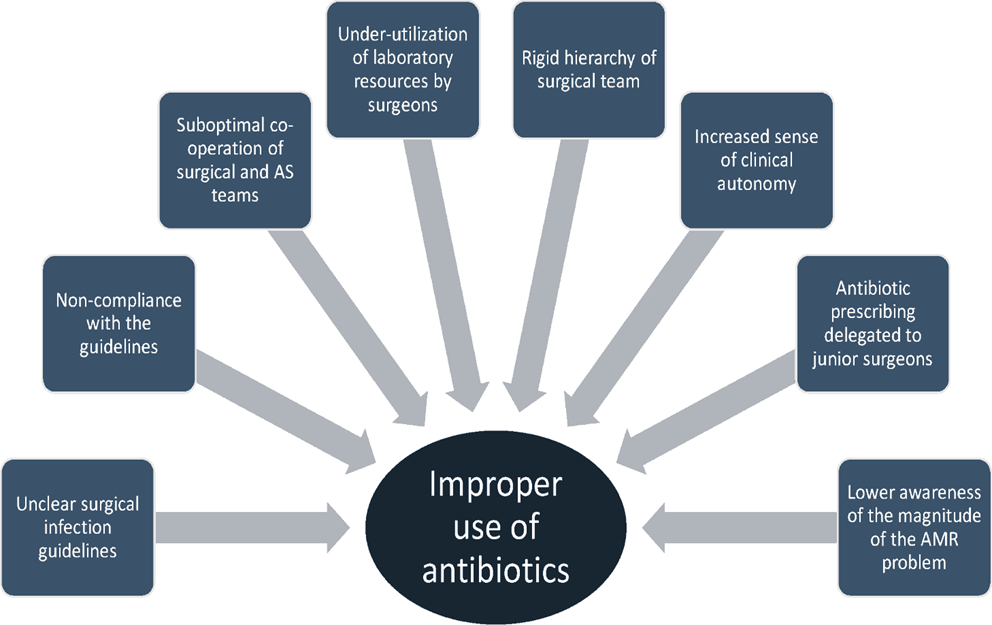
According to the Center for Disease Control (CDC), 20 to 50% of all antibiotics prescriptions in the acute care hospital setting in the USA are either unnecessary or inappropriate. CDC also stated that most antibiotics prescriptions include nursing homes and long-term care facilities (LTCF). Like the hospital setting, 40% to 75% of antibiotics prescribed in nursing homes and LTCF may be unnecessary or inappropriate. The current scientific literature emphasizes on reduction of inappropriate use of antimicrobials in all healthcare settings. Along with the Centers for Medicare and Medicaid Services (CMS), CDC, and Society for Healthcare Epidemiology of America(SHEA), the Joint Commission developed the AMS standard for hospitals, critical access hospitals, and nursing care centers. The standard for ambulatory settings and office-based surgery practices is still under development. The CMS also finalized a new regulation in 2019 requiring all US hospitals to develop Antimicrobial Stewardship programs by March 2020.
The AMS programs have the following goals:
With the above goals in target, the AMS programs include the following core elements:

Leadership Commitment
Leadership support is crucial for the success of antimicrobial stewardship programs. They can be in different forms, including:
Accountability and Drug Expertise
To identify a single leader as a stewardship program leader who will be responsible for the program outcome. Literature has shown that physician leaders have highly successful programs. Physicians with formal training in infectious disease and AMS benefit stewardship program. Similarly, appointing a single pharmacist leader as co-leader has shown improved outcome.
Action
Action includes implementing policies supporting optimal antibiotic use, utilizing specific interventions to improve antibiotic use, and prioritizing intervention based on the needs of the care setting. Examples for policies supporting optimal antimicrobial prescription include specifying dose, duration, and indication on documentation. The implementation of policies helps to ensure modification or prompt discontinuation of antimicrobials. Similarly, developing and implementing facility-specific treatments based on local susceptibilities using antibiogram and national guidelines help optimize antibiotic selection and duration.
Interventions directed towards stewardship can be categorized into
The pharmacy interventions also alert the prescriber in cases of the unnecessary overlapping spectrum of antimicrobial coverage, help in detecting and preventing drug interactions related to antibiotics.
Interventions for UTI focus on avoiding unnecessary management of asymptomatic cases and ensuring that patients receive the right therapy based on local susceptibilities and for a suitable duration. Similarly, there are interventions for community-acquired pneumonia, skin and soft tissue infections, Methicillin- Resistant Staphylococcus Aureus (MRSA), Clostridoides difficile infection (CDI), and treatment of culture-proven invasive infections.
Tracking and Reporting of Antimicrobial use and Outcomes
Keeping track of the evaluation of both policies and outcomes is critical to identify areas of improvement and assess the impacts of improvement efforts. For example, determining if the prescriber has applied the diagnostic criteria accurately; prescribed the antimicrobial agent for a particular indication with documentation of duration and relevant tests before treatment. CDC has developed an Antibiotic Use (AU) option as a part of the National Healthcare Safety Network (NHSN). AU automatically collects data and monthly reports for the duration of therapy data and is later analyzed in aggregate by specific agents and patient care locations. The AU module is available to facilities with the capability to submit electronic medication administration records. Likewise, tracking outcomes that measure the impact of interventions help optimize antimicrobial use.
Education
Regular updates to prescribers on antibiotic prescribing, antibiotic resistance, and infectious disease management motivate optimization in antimicrobial prescription. However, didactic presentations, electronic messages to staff groups are few options to provide education. Education has been most effective when paired with corresponding interventions and outcome measurements.
The spectrum of infectious diseases is rapidly evolving. Emerging infectious agents present with a constellation of challenges. The highly virulent pathogens with increased resistance result in increased morbidity, mortality, and healthcare costs. It has been estimated that ten million people will die every year due to AMR by 2050. CDC has published antibiotic-resistant threat reports in 2013 and 2019. According to the 2019 report, in the US, more than 2.8million antibiotic-resistant infections occur each year, and more than 35000 people die. In addition to this, it also mentioned that 223,900 cases of Clostridoides difficile occurred in 2017, of which 12800 people died. The report did not include viruses or parasites.
The report categorized the threats into four tiers based on level of concern to human health;
World Health Organisation created a priority list of pathogens in 2017 and 2020 based on their substantial threat to morbidity and mortality.
The priority list is categorized into three tiers:
3. High Priority
o Vancomycin-Resistant Enterococcus faecium
Clinical Significance
Antibiotics have transformed the healthcare system, making once lethal infection readily treatable. It has also helped to make other medical advances like cancer chemotherapy and organ transplants possible. Prompt initiation of antimicrobials has reduced morbidity and mortality, for example, in cases of sepsis. However, 30% of all antibiotics prescribed in hospitals are unnecessary or suboptimal. Health care is in dire need of responsible and optimized use of antimicrobial agents for the safety of our current and future patients. It is important to enlighten the point that antibiotics differ from other drugs. With emerging resistance, the antibiotics that were being used are no longer as effective as they are. Compared to other specialties, their drugs are continuously improved in addition to the old ones. Like all medications, antibiotics have serious adverse effects. Around 20% of hospitalized patients on antibiotics experience side effects. C. difficile has widely illustrated the adverse impact on patients' health even to those not directly exposed to antibiotics. Around 140,000 visits to the emergency department occur annually for antibiotics. In hospitalized patients, severe reactions, including renal and bone marrow toxicity, can be seen. A retrospective study from 2006-2010 by Baggs et al. revealed 0.6% increased sepsis risk within 90 days of discharge following sepsis admission. The study included 473 US hospitals and revealed broad-spectrum antibiotics were associated with a 50% increased risk of readmission within 90 days. Another study by Roberts et al. also estimated that the cost of treatment for antimicrobial-resistant infection is around 18- 29,000 USD per patient, with an increase in hospital stay by 6.4 to 12.7 days and attributable mortality of 6.5%. The goal of antimicrobial stewardship is better patient care, reduced antibiotic use, and cost-effective health care are favorable side effects. Antimicrobial stewardship programs have shown promising results in numerous health care settings. Reported benefits include reducing the incidence of C. difficile infection, reducing AMR, improved dosing in renally-impaired patients, improved infection cure rates, decreased mortality rates, and hospital cost savings. The meta-analysis by Davey et al. has shown that interventions for a reduction in excessive antibiotic prescription in inpatient patients can reduce AMR or nosocomial infections. Likewise, interventions to increase effective prescribing following the national and local guidelines can improve the clinical outcome. The CDC's 2019 Antibiotic resistance Threat report has shown an 18% overall decline in deaths from AMR compared to the 2013 report and a decline in deaths by AMR by 28% in-hospital patients. Similarly, the report has shown a 41% decline in VRE, 33% in Carbapenem-resistant Acinetobacter, 29% in multidrug- resistant Pseudomonas aeruginosa, 25% in Candida, and 21% in MRSA. Although the results for high-priority pathogens are promising, the report also highlighted a 315% increase in erythromycin- resistant invasive group A Streptococcus, 124% in drug-resistant gonorrhea, and 50% in ESBL Enterobacteriaceae. The CDC's annual outpatient antibiotics prescription report for 2018 has shown that 249.8 million antibiotics prescriptions have been dispersed throughout the US. This antibiotic dispense is equivalent to 763 prescriptions per 1000 people. When comparing with the highest prescription according to provider specialty, their data reveals the highest prescription by dermatologist-525 antibiotic prescription per 1000 person followed by physician assistants and nurse practitioners with 423 prescriptions per 1000 person and Emergency Medicine 392 per 1000 person. With the overuse or abuse of antimicrobials, up-trending antimicrobial resistance, and limited antimicrobial resources, it is high time we take action.
Other Issues
Antibiotic resistance is a global crisis. Not only a human population but also food and food animals are equally contributing to antibiotic resistance. Animals also carry bacteria in their gut which might also include antibiotic-resistant bacteria. People can get infections from handling or eating meat or food contaminated with resistant bacteria, from contact with animal waste, from touching animals without proper handwashing. Antibiotics are actively used in livestock farming for treatment purposes and used in subtherapeutic levels for growth promotion and increase productivity.
As per WHO, antimicrobial use in livestock can be classified into:
The study by Boeckel et al. noted that the total consumption of antibiotics in livestock in 2010 was 63,151 tons. They also projected that consumption of antimicrobials will increase by 67% by 2030. It is estimated that 65% of medically important antibiotics in the US are used for food animals, compared to 35% in humans. The antibiotics also used in humans are referred to as medically important antibiotics. This might lead to antibiotic pollution resulting in antibiotic residues in animal-derived products. These products like meat, milk, eggs, when consumed by humans, can cause the emergence of resistant bacterial strains, therapeutic failure in some cases. Widespread use of antimicrobials drives the emergence of antibiotic-resistant organisms in the food industry that can cause diseases in humans like E. Coli, Campylobacter, enterococci, Salmonella. Antibiotic-resistant organism in food is a global health concern. 600 million cases and 420,000 deaths occur per year from food-borne diseases. The Food and Drug administration report in 2019 revealed that more than 6.1 kilograms of medically important antibiotics are sold and distributed to US farmers. The most antibiotic use was in cattle (41%), swine (42%), turkeys(10%), and chickens (3%). The most commonly used antibiotics for livestock were tetracyclines(67%), penicillin (12%), macrolides(8%). The data also revealed that sales increased by 4% compared to the year 2018. Considering the emergent circumstance, CDC founded One health in 2009 to achieve optimum health outcomes via a multisectoral, transdisciplinary approach that recognizes the interconnection between people, animals, and the environment. The plan recommends the complete restriction of medically important antibiotics in livestock for disease prevention and growth promotion.
There are opportunities for antimicrobial stewardship on farms.
Some of them are listed below:
Enhancing Healthcare Team Outcomes
The Agency for Healthcare Research and Quality is an excellent resource for antimicrobial stewardship, including best practices in all healthcare settings, methods for developing and improving antimicrobial stewardship, and developing a culture for safety during prescribing. One tool for use by prescribers of antibiotics is their 'Four Moments of Antibiotic Decision Making.'
Moment 1 is considering the question if the patient has an infection and does it require antibiotics. Prescribers tend to order antibiotics to the hospitalized patient in response to abnormal clinical signs or lab results (for example- isolated fever or leukocytosis). This moment asks prescribers to pause, rethink and analyze all relevant information to determine the likelihood of any infectious process. At present, COVID 19 pandemic sets as a perfect example of antibiotics prescribed without any bacterial infection.
Moment 2 is to think about what cultures should be obtained and the best empiric treatment. This moment focuses on the need for culture data when appropriate before administering the antibiotics. When no specific data is available, there is a tendency for prolonged broad-spectrum antibiotic therapy. The second part of Moment 2 ensures timely administration of empirical therapy based on severity and likely source of infection. For example, patients are at low risk of MRSA for urinary tract infections. Therefore they would not benefit from IV vancomycin. Local antibiotics guidelines should be developed for common inpatient infections- this aids in enacting Moment 2.
Moment 3 is the question of, after a day or so of antibiotics being used, should the regimen be stopped, narrowed, or changed from IV to oral treatment. This process should be ongoing. For instance, most patients with community-acquired pneumonia become stable with normal vital signs by day three and are at an excellent time to switch to oral medications. Antibiotics time-outs should be used to address Moment 3. Nurses and pharmacists are excellent resources to prompt clinicians regarding further plans about antibiotics. At the same time, clinicians should also document their decision regarding the choice of antimicrobial therapy, indication, duration, and dosing. IT department can also help by regularly updating the electronic health records system with prompts to review orders, set up antimicrobial time-outs, etc. This way, clinicians are prompted with indication, duration, dosing, route of therapy.
Moment 4 considers how long the antibiotic should be continued for the treatment of the patient's infection. There has been an increasing number of studies that support a shorter duration of therapy than previously prescribed. Local and national antibiotics guidelines help to uniform the duration of antimicrobial therapy prescription. Antimicrobial stewardship is a coordinated effort between inter-professional teams, including clinicians/prescribers, nursing staff, pharmacists, microbiologists, infection prevention teams, and patient safety teams. Targeted goals and multidisciplinary approach interventions result in excellent clinical, economic outcomes.
Nursing, Allied Health, and Inter- professional Team Interventions
The success of antimicrobial stewardship programs is deeply connected with the core elements mentioned above as guided by the CDC. The antimicrobial stewardship programs are greatly enhanced by interdepartmental communication and coordination.
The significant support from below mentioned groups can play a vital role;
Clinicians: All clinicians at any point during patient care have prescribed antibiotics to the patients.
Therefore it is crucial that all clinicians fully engage and support antibiotics optimization. Hospitalists and primary care physicians are particularly essential as they comprise a majority of the prescribers. Prescribers can act as good stewards by following the 5 "D"s of antimicrobial stewardship; right Drug, correct Dose, right Drug-route, suitable Duration, timely De-escalation to pathogen-directed therapy. Example actions include making accurate diagnoses, following local antimicrobial guidelines, and timely reviewing the need for therapy.
For instance, integrating stewardship into order sets. They can also help educate patients regarding medications and be a very useful resource to physicians when prescribing antibiotics.
Examples include triaging patients for isolation, a timely collection of culture samples before antimicrobial use, educating patients on how to take antimicrobials at discharge from the hospital.
Microbiology lab staff can assist as a part of diagnostic stewardship by guiding proper use of the test.
They also help in creating local anti-microbiogram, which help optimize antimicrobial prescriptions.
Examples include developing prompts to review antimicrobials and their indication, incorporating order sets in electronic medical records;
Nursing, Allied Health, and Interprofessional Team Monitoring
In the United States, around fifteen percent of inpatient patients report penicillin allergy, of which approximately one percent have a severe penicillin allergy. An important step is to not merely accept what is in the electronic medical record (EMR). It is important to reassess the documentation with the patient about the actual event regarding the antibiotic allergic event. Too often, it is labeled in the EMR as an allergy when it was a side effect of the drug or that the actual allergic effect was not clarified. Some data show that 50% of allergies documented are non-immunologic and mostly adverse effects. Having to substitute another class of drugs rather than beta- lactams can cause a tendency to use broad classes of antimicrobials to be used to treat the patient's infection. The consequences of using inappropriate allergy labels include increase broad-spectrum antibiotics use, limited therapeutic options, increased toxicity, and increased hospital costs. Charneski et al.'s study on 11,872 inpatients revealed that 11.2% of inpatients had allergy labeled with antimicrobial and had increased hospital length of stay, greater antimicrobial use, higher intensive care admission rate, higher readmission rate, and higher mortality. Adequate history and physical exam, skin testing, and challenge dosing are few ways to assess the allergy. Nurses can be vital in assessing drug allergies. Pharmacists can also play a pivotal role while updating EMR about patient's medication lists and drug interactions.
Promotion Of Antibiotic Stewardship
For Healthcare Professionals
Healthcare providers should follow best practices, such as choosing the right antibiotic based on culture results and using diagnostic testing to confirm bacterial infections. It is essential to emphasize to patients the value of finishing specified schedules and avoiding from using antibiotics unnecessarily. Hospitals and other healthcare institutions may optimize antibiotic use, lower antibiotic resistance, and enhance patient outcomes by implementing antibiotic stewardship programs that offer recommendations, education, and monitoring. These initiatives support appropriate prescription practices and ongoing quality enhancement to guarantee successful care while lowering the possibility of resistance developing.
For Patients
To guarantee effective treatment and prevent antibiotic resistance, patients should only take antibiotics recommended by medical specialists and take them for the entire prescribed duration as instructed. Antibiotic overuse can result in improper administration, treatment failure, and the emergence of resistant microorganisms. Patients can obtain trustworthy resources to learn more about antibiotic stewardship from pharmacies or healthcare facilities, credible websites such as the Centers for Disease Control and Prevention (CDC), and advice from healthcare providers. It is critical to comprehend and abide by these guidelines to maintain the efficacy of antibiotics and protect both public and individual health.
For Policy Makers
Policymakers play an essential role in selling the right use of antibiotics across the economic system by following legal guidelines and policies. Among those attempts are tips for healthcare vendors, bans on antibiotic utilization in agriculture, and steps to halt the selling of medicines without a prescription. Financing the creation of recent medicines and alternative therapies is likewise important to addressing the rapidly increasing problem of antibiotic resistance. Investing in innovation can serve to be useful for the improvement of diagnostic tools, preventative measures, and novel remedies for infections with resistance. Both monetary support and legislative tasks are important for a comprehensive strategy to cope with antibiotic resistance and to make certain that antibiotics continue to be powerful for upcoming generations.
CONCLUSION
Even though antimicrobial stewardship was introduced in 1996, antimicrobial resistance still remains a global crisis. However, during the COVID-19 pandemic, antibiotic stewardship program efforts slowed tremendously due to the changes in patient care, testing, treatment, and staff availability. As a result, there was an increase in combined antimicrobial resistance by 20%.23 Antimicrobial stewardship is necessary for better patient outcomes and reduced healthcare costs. So, actions mentioned in the guidance documents for antimicrobial stewardship need to be made a habitual practice in every healthcare setting so that even if there are pandemic situations in the future there is no rise in antimicrobial resistance. The emergence of newer technologies enabling rapid accurate diagnosis, and the increased incorporation of big data, artificial intelligence (AI), and internet of things (IoT). In healthcare is making personalized medicine possible. Personalized medicine will make antimicrobial stewardship programs a success. Antibiotic stewardship is critical to retaining the effectiveness of antibiotics in the future and addressing the rising trouble of antibiotic resistance. Essential teachings embody the necessity of educating sufferers, finishing unique remedies, and using antibiotics sensibly. Recognizing that sufferers, lawmakers, healthcare carriers, and the general public all have a very important role in the fight against antibiotic resistance. When those parties collaborate, successful stewardship policies and projects might be positioned in place. To fight antibiotic resistance, collaboration among all parties is vital. By operating together, we can prevent the misuse and overuse of antibiotics. We can halt the growth of antibiotic-resistant microorganism, and preserve the efficacy of those existence-saving drugs. Let’s get started right now by assisting legislation that encourages stewardship, elevating awareness of the importance of the usage of antibiotics well. Together, we can ensure that antibiotics continue to be a cornerstone of advanced medication by safeguarding those valuable sources for upcoming and future generations.
REFERENCES




Badal Kr. Singh*, Ritik Kumar, Khushi Singh, Ritika, Antibiotic stewardship & Its Importance, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 467-482. https://doi.org/10.5281/zenodo.16745995
 10.5281/zenodo.16745995
10.5281/zenodo.16745995
