Department of Pharmacology, RBVRR Women's College of Pharmacy, Affiliated to Osmania University, Hyderabad-500027, Telangana State, India.
Angiogenesis, the formation of new blood vessels from pre-existing vasculature, is a fundamental biological process occurring throughout life, from embryonic development to tissue maintenance and repair in adulthood. No metabolically active tissue lies more than a few hundred micrometers from a blood capillary, emphasizing the critical role of angiogenesis in sustaining cellular viability. Over the past four decades, the recognition of angiogenesis as a pivotal player in both physiological and pathological processes has garnered considerable therapeutic interest. Under physiological conditions, angiogenesis facilitates growth, wound healing, and tissue regeneration. Conversely, its dysregulation is implicated in numerous pathological states, including cancer, cardiovascular diseases, diabetic retinopathy, and rheumatoid arthritis. The dual nature of angiogenesis, as both a restorative and a pathological mechanism, has made it a compelling target for therapeutic intervention. While inhibition of angiogenesis, particularly via vascular endothelial growth factor (VEGF) antagonists, has yielded promising outcomes in slowing tumor progression, limitations such as therapeutic resistance and limited survival benefits persist. Future directions are increasingly focused on combinatorial approaches that integrate anti-angiogenic agents with immunotherapies to enhance clinical efficacy. Conversely, therapeutic stimulation of angiogenesis offers hope in regenerative medicine, particularly for treating ischemic conditions and enhancing tissue repair. Emerging technologies such as nanomedicine and novel targeting of alternative angiogenic pathways are opening new frontiers for precise and individualized therapies. This review aims to comprehensively explore the dual role of angiogenesis in health and disease, highlighting its therapeutic potential in both regenerative medicine and oncology. It discusses current anti- and pro-angiogenic strategies, key molecular targets, limitations of existing therapies, and innovative future approaches, including combination regimens and nanotechnology-driven interventions.
Angiogenesis, the process of forming new blood vessels from pre-existing vasculature, is a finely tuned and essential biological phenomenon. This process involves the activation, proliferation, migration, and differentiation of endothelial cells, which line the inner walls of blood vessels. Angiogenesis is predominantly regulated by a coordinated interplay of chemical signals growth factors, cytokines, and extracellular matrix components that orchestrate vascular remodelling in response to developmental, physiological, or pathological stimuli. Throughout the human lifespan, from embryogenesis to aging, angiogenesis plays a pivotal role in maintaining tissue homeostasis. Under physiological conditions, it is indispensable for organogenesis, wound healing, tissue regeneration, and the cyclic processes of the female reproductive system, such as ovulation and menstruation. Notably, no metabolically active tissue lies more than a few hundred micrometres from a capillary, emphasizing the crucial dependence of cellular viability on proper vascularization. The formation of capillaries through angiogenesis ensures adequate delivery of oxygen, nutrients, and removal of metabolic waste. [1,2,3] The historical evolution of angiogenesis research spans over two millennia, with early anatomical observations giving way to modern molecular insights. A landmark in angiogenesis research came in the 1970s when Judah Folkman introduced the revolutionary hypothesis that tumor growth is angiogenesis-dependent, leading to the birth of the field of tumor angiogenesis. This paradigm shift catalyzed the discovery of specific angiogenic regulators such as vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF). Over the subsequent decades, our understanding of angiogenesis has been significantly enriched by interdisciplinary contributions from oncology, cardiovascular science, immunology, and regenerative medicine.[4] In normal physiology, angiogenesis ensures tissue repair and regeneration following injury, ischemia, or inflammation. In embryonic development, it works in concert with vasculogenesis to establish and expand the vascular network. In adults, angiogenesis is usually quiescent but can be rapidly reactivated by hypoxic or inflammatory cues. For example, in ischemic myocardial tissue or gastrointestinal ulcers, angiogenic signaling restores perfusion and accelerates healing. VEGF and FGF remain central to these processes, regulating endothelial proliferation, vascular permeability, and new capillary sprouting. Conversely, dysregulated or excessive angiogenesis underlies numerous pathological conditions. In cancer, pathological angiogenesis facilitates tumor growth, immune evasion, and metastasis. Tumor cells often exploit angiogenic factors like VEGF to stimulate neovascularization, ensuring their sustained growth and dissemination. Similar mechanisms are observed in diabetic retinopathy, rheumatoid arthritis, psoriasis, and systemic lupus erythematosus, where abnormal neovascularization contributes to tissue destruction and chronic inflammation. In cardiovascular diseases, angiogenesis assumes a dual role. On one hand, therapeutic angiogenesis is a promising approach in ischemic heart and peripheral artery disease, aiming to restore blood flow through neovascularization. Clinical interventions have explored the use of angiogenic growth factors and gene therapy for this purpose. On the other hand, intraplaque angiogenesis in atherosclerosis may lead to plaque instability, hemorrhage, and increased risk of thrombosis. The expression of VEGF within atherosclerotic lesions has been linked to smooth muscle proliferation, macrophage recruitment, and enhanced inflammation.[5,6,7,8] Moreover, angiogenesis is modulated by a complex interplay of hypoxia-inducible factors (HIFs), nitric oxide, cytokines, and metabolic regulators. Hypoxia is a potent inducer of angiogenesis via HIF-mediated upregulation of VEGF in ischemic tissues. Interestingly, both hyperglycemia and hypoglycemia can modulate VEGF expression, establishing a mechanistic link between metabolic dysfunction and vascular complications, especially in diabetes mellitus. [9,10] This review aims to provide a comprehensive and critical analysis of the dual role of angiogenesis in health and disease, with emphasis on its molecular regulation, diagnostic approaches, and therapeutic implications.
Molecular Mechanisms of Angiogenesis [11-15]
Angiogenesis is a tightly regulated, multi-step biological process that leads to the formation of new blood vessels from pre-existing vasculature. This phenomenon is crucial for physiological processes such as embryonic development, wound healing, and tissue regeneration, but it also plays a pivotal role in pathological conditions like tumor growth, diabetic retinopathy, and rheumatoid arthritis.[11-15] The principal stages of angiogenesis include:
a) Endothelial Cell Activation
Angiogenesis is typically initiated in response to hypoxia or tissue injury, which stimulates the release of pro-angiogenic factors such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and angiopoietins. These factors activate endothelial cells (ECs) that line the interior surface of existing blood vessels, initiating the angiogenic cascade.
b) Degradation of the Basement Membrane
Upon activation, endothelial cells secrete proteolytic enzymes, primarily matrix metalloproteinases (MMPs), which degrade components of the basement membrane and extracellular matrix (ECM). This degradation facilitates the detachment and migration of ECs by creating physical space and altering the extracellular environment.
c) Endothelial Cell Migration
Guided by chemotactic gradients of angiogenic stimuli, endothelial cells migrate toward the hypoxic or injured tissue. This directed migration is a critical step in establishing the nascent vascular sprout.
d) Endothelial Cell Proliferation
Concurrently with migration, ECs undergo proliferation to ensure an adequate cellular supply for the elongation and expansion of the newly forming vessel. This step is regulated by mitogenic signals, predominantly mediated by VEGF and FGF pathways.
e) Tube Formation
Migrating and proliferating ECs begin to align and form intercellular junctions, organizing into three-dimensional tubular structures. This process results in the formation of capillary-like lumens capable of supporting eventual blood flow.
f) Maturation and Stabilization
To ensure structural and functional integrity, the immature endothelial tubes recruit mural cells, such as pericytes and vascular smooth muscle cells. These supporting cells envelop the endothelial tubes, promote basement membrane reformation, and contribute to vessel stabilization and reduced permeability.
g) Vascular Remodeling and Integration
The final phase involves the pruning, remodeling, and integration of the neovasculature into the pre-existing vascular network. Blood flow is established, and the vessel architecture is refined in accordance with the metabolic and oxygen demands of the surrounding tissue.[11-15]
Major Signalling Pathways In Angiogenesis[16-20]
Angiogenesis is orchestrated by a tightly controlled network of signaling pathways that regulate endothelial cell (EC) behavior and coordinate interactions with surrounding stromal and perivascular cells. These pathways are activated by extracellular signals primarily growth factors, that bind to specific receptors on the cell surface, initiating intracellular cascades that govern cell proliferation, migration, survival, and new vessel formation. A thorough understanding of these molecular mechanisms is critical for the development of therapeutic strategies aimed at either promoting angiogenesis (e.g., in ischemic diseases) or inhibiting it (e.g., in cancer and retinopathies).[16-20]
VEGF is a central mediator of angiogenesis, with VEGF-A being the most extensively studied isoform. It primarily exerts its angiogenic effects through VEGF receptor-2 (VEGFR-2), a tyrosine kinase receptor expressed on endothelial cells. Activation of VEGFR-2 leads to the stimulation of downstream signaling pathways such as PI3K/AKT (promoting cell survival and nitric oxide production) and MAPK/ERK (regulating proliferation and migration).
VEGF expression is tightly regulated by hypoxia and is crucial for endothelial sprouting, increased vascular permeability, and neovascular network formation.
Among the FGF family, FGF-2 (basic FGF) is a potent pro-angiogenic factor. It binds to FGF receptors (FGFRs), which are also tyrosine kinase receptors, triggering multiple intracellular signaling cascades, including:
FGFs not only stimulate endothelial cell proliferation and chemotaxis but also contribute to extracellular matrix (ECM) degradation and remodeling, facilitating angiogenic sprouting.
The angiopoietin–Tie signaling axis plays a pivotal role in the maturation, stabilization, and remodeling of blood vessels:
This balance between Ang-1 and Ang-2 is essential for the fine-tuning of vessel stability versus plasticity during angiogenic processes.
The Notch signaling pathway is critical for determining endothelial cell fate and maintaining vascular patterning during sprouting angiogenesis. Activation occurs through ligand–receptor interactions, primarily between Delta-like ligand 4 (Dll4) and Notch1–4 receptors on adjacent cells.
This pathway ensures that newly formed vessels are structured, functional, and efficiently perfused.
Hypoxia is a major physiological and pathological trigger for angiogenesis. Rapidly growing tumors and ischemic tissues often outpace their vascular supply, resulting in low oxygen tension. In such environments, HIF-1α escapes degradation and accumulates in the nucleus, where it dimerizes with HIF-1β to form an active transcription factor complex.
Types Of Angiogenesis
Angiogenesis occurs through two principal mechanisms:
(a) Sprouting Angiogenesis
(b) Intussusceptive Angiogenesis
(a) Sprouting Angiogenesis
Sprouting angiogenesis is the predominant and most extensively characterized form of neovascularization. It involves the formation of new capillary branches from pre-existing blood vessels in response to pro-angiogenic stimuli, particularly under conditions of tissue hypoxia, inflammation, or growth factor signaling (notably VEGF-A).The process initiates when pro-angiogenic signals, such as VEGF, FGF, and angiopoietins activate quiescent endothelial cells (ECs) in the parent vessel. These activated ECs secrete matrix metalloproteinases (MMPs), including collagenase, which degrade the basement membrane and surrounding extracellular matrix (ECM), thereby allowing endothelial cell migration (Figure 1).
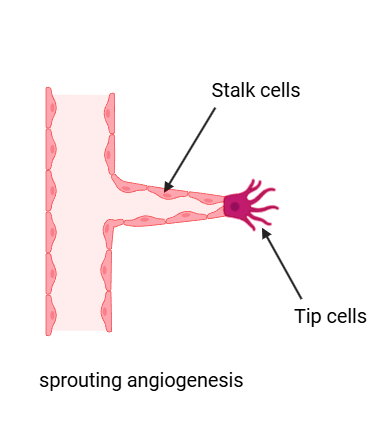
Figure 1: Sprouting angiogenesis
Key Steps in Sprouting Angiogenesis:
1.Tip Cell Selection and Guidance
A subset of ECs adopts the “tip cell” phenotype, characterized by high expression of VEGFR-2 and Dll4 (Delta-like ligand 4). Tip cells extend filopodia to sense and navigate toward angiogenic signals, guiding the direction of sprout formation.
2. Stalk Cell Proliferation
The ECs behind the tip cell become “stalk cells”, which proliferate and elongate the developing sprout. These cells are driven by VEGF-induced activation of Notch signaling, which suppresses the tip cell phenotype and maintains vessel integrity.
3. Lumen Formation and Anastomosis
As the stalk elongates, lumen formation occurs through vacuole coalescence or cord hollowing, enabling the eventual passage of blood. The nascent sprout connects (anastomoses) with adjacent vessels or other sprouts, forming a continuous vascular loop.
4. Maturation and Stabilization
Pericytes and smooth muscle cells are recruited through PDGF-B and Ang-1/Tie2 signaling to stabilize the new vessel. A new basement membrane is deposited, and the vessel transitions to a quiescent state unless further stimuli are present. Sprouting angiogenesis plays a critical role in embryonic vascular development, wound healing, organ regeneration, and tissue perfusion in ischemic conditions. It is particularly prominent in avascular tissues such as the brain and retina, where the vascular network must continuously expand and remodel to meet metabolic demands.Dysregulated sprouting angiogenesis contributes to various pathological conditions, including tumor growth, diabetic retinopathy, psoriasis, and chronic inflammatory diseases, making it a key target for both pro-angiogenic and anti-angiogenic therapies.[21,22,23]
(b) Intussusceptive Angiogenesis
Intussusceptive angiogenesis, also known as intussusceptive microvascular growth (IMG), is a non-sprouting mechanism of blood vessel formation in which pre-existing vessels split longitudinally to form new vascular structures. Unlike sprouting angiogenesis, which requires endothelial cell (EC) proliferation, migration, and extensive extracellular matrix remodeling, intussusceptive angiogenesis occurs with minimal cellular proliferation and preserves the integrity of existing perfused vessels, making it a rapid and energy-efficient process (Figure 2).
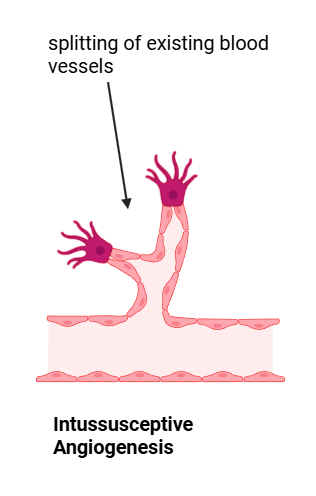
Figure 2: Intussusceptive Angiogenesis
Mechanism of Intussusceptive Angiogenesis:
The hallmark feature of intussusceptive angiogenesis is the formation of intraluminal tissue pillars that progressively expand to divide a single blood vessel into two distinct lumens. The process proceeds through the following sequential steps:
1. Pillar Initiation:
Small transluminal pillars, composed initially of opposing endothelial cells from the vessel wall, begin to form by extending into the lumen. These protrusions are typically 2–5 µm in diameter and are stabilized by extracellular matrix components such as collagen fibers and, occasionally, pericyte extensions.
2. Pillar Expansion and Maturation:
The endothelial bilayer surrounding the pillar forms transcellular perforations or gaps, allowing interstitial cells, including pericytes and fibroblasts, to invade the core. The intraluminal pillar enlarges as the basement membrane is remodeled, eventually leading to a complete partitioning of the vessel lumen into two functional and independent capillaries.
3.Vascular Reorganization:
As intussusception continues, the newly formed vessels can further remodel, adapt, or integrate into the existing vascular network. This mechanism enables dynamic adjustment of capillary density and geometry, facilitating efficient microcirculatory regulation.[24,25,26]
Vasculogenesis Vs. Angiogenesis
Vasculogenesis is the process of de novo blood vessel formation, predominantly occurring during embryogenesis. It initiates with the differentiation of mesodermal progenitor cells into hemangioblasts, which further differentiate into endothelial precursor cells (angioblasts) and hematopoietic cells. These endothelial precursors coalesce to form primitive blood islands, which subsequently fuse to establish the primary vascular plexus, giving rise to major embryonic vessels such as the dorsal aortae and the heart. In contrast, angiogenesis refers to the formation of new blood vessels from pre-existing vasculature. This process is critical for vascular growth, remodeling, and repair throughout postnatal life, including physiological events such as tissue growth and wound healing, as well as pathological conditions like tumor progression and chronic inflammation. Angiogenesis proceeds via two principal mechanisms: sprouting angiogenesis, characterized by endothelial cell proliferation and migration to form new capillary branches, and intussusceptive angiogenesis, where existing vessels split and expand through intraluminal pillar formation.In summary, vasculogenesis establishes the primary vascular network during early development, while angiogenesis drives the subsequent expansion, remodeling, and functional adaptation of the vascular system in both physiological and pathological contexts.[27,28,29]
ANGIOGENESIS IN PHYSIOLOGICAL VS. PATHOLOGICAL CONDITIONS
Angiogenesis refers to the formation of new blood vessels from pre-existing vasculature. Under physiological conditions, angiogenesis is a finely regulated process essential for normal biological functions such as wound healing, embryonic development, endometrial regeneration, and tissue growth. It is tightly orchestrated by a dynamic balance between pro-angiogenic and anti-angiogenic factors, ensuring transient, localized vessel formation necessary for tissue repair and regeneration. In contrast, pathological angiogenesis is characterised by a dysregulation of this balance, leading to excessive or abnormal vessel growth. This uncontrolled angiogenesis contributes to the progression of various diseases, including cancer, diabetic retinopathy, rheumatoid arthritis, and psoriasis. In these conditions, sustained expression of pro-angiogenic signals, particularly vascular endothelial growth factor (VEGF),supports aberrant neovascularization, chronic inflammation, and tissue destruction.[30,31,32] Table 1 summarizes the key distinctions between physiological and pathological angiogenesis:
Table 1: Comparison of Physiological and Pathological Angiogenesis
|
Feature |
Physiological Angiogenesis |
Pathological Angiogenesis |
|
Context |
Occurs during normal processes such as wound healing, embryogenesis, and menstruation |
Occurs in disease states including cancer, diabetic retinopathy, rheumatoid arthritis, and psoriasis |
|
Regulation |
Tightly controlled by a balance between pro- and anti-angiogenic factors |
Dysregulated; dominated by excessive pro-angiogenic signals (e.g., VEGF overexpression) |
|
Purpose |
Restores perfusion to ischemic or injured tissues |
Supports tumor growth, metastasis, and pathological tissue remodeling |
|
Example |
Promotes endometrial regeneration during the menstrual cycle |
Drives neovascularization in diabetic retina, contributing to vision impairment |
|
Outcome |
Facilitates proper wound repair and tissue regeneration |
Leads to chronic inflammation, edema, and joint/tissue damage |
|
Growth Factor Activity |
Transient and spatially restricted activity of VEGF, FGF, and other mediators |
Persistent, unregulated VEGF/PDGF signaling promoting pathological neovascularization |
Biomarkers And Diagnostic Tools In Angiogenesis [33,34,35,36]
Angiogenesis is essential in both normal and disease conditions. Its evaluation is important in diseases such as cancer, diabetic retinopathy, and arthritis. Diagnostic tools, including biomarkers and imaging techniques, help monitor disease progression and therapeutic outcomes.
A. Circulating Endothelial and Progenitor Cells (CEC and CEP)
B. Angiogenic Factors in Blood (Serum and Plasma)
C. Imaging Techniques
a. Dynamic Contrast-Enhanced MRI (DCE-MRI)
b. Doppler Ultrasound
c. Positron Emission Tomography (PET)
d. Computed Tomography (CT) and CT Angiography
e. Optical Imaging
f. Micro-CT and Micro-MRI
ELISA and Other Assays: Used to quantify circulating angiogenic factors in blood samples.
Immunohistochemistry: Used to assess MVD (micro vessel density) and other markers in tissue samples.
Genomic and Proteomic Approaches: Identify genes and proteins involved in angiogenesis.
Monitoring angiogenesis using both biomarkers (CEC, CEP, VEGF, etc.) and imaging techniques (MRI, PET, Doppler) allows for better diagnosis, treatment selection, and evaluation of therapy response. Combining these tools gives a comprehensive understanding of vascular changes in health and disease. [33,34,35,36]
Therapeutic Modulation of Angiogenesis
Angiogenesis is a critical physiological process involving the formation of new blood vessels from existing vasculature. In healthy individuals, it plays a fundamental role in wound healing, reproductive function, and tissue regeneration. However, dysregulated angiogenesis can lead to pathological consequences, either inadequate vascularization, as seen in ischemic disorders, or excessive neovascularization, typical of cancer and inflammatory diseases.To therapeutically modulate this process, two opposing strategies have been developed: pro-angiogenic therapies, aimed at enhancing blood vessel formation in ischemic conditions, and anti-angiogenic therapies, designed to inhibit abnormal vascular growth in malignancies and other pathological states.[37,38,39,40]
A. Pro-Angiogenic Therapies
Pro-angiogenic interventions aim to restore or enhance tissue perfusion in conditions where blood supply is compromised. These approaches are particularly valuable in treating ischemic cardiovascular and peripheral vascular diseases, chronic wounds, and neurovascular injuries.
Diseases Targeted by Pro-Angiogenic Therapies
Therapeutic Strategies and Representative Examples
a. Growth Factor Therapy
This approach utilizes exogenous delivery of angiogenic proteins to stimulate endothelial cell proliferation, migration, and capillary formation.
b. Gene Therapy
Gene-based therapies involve the introduction of genes encoding angiogenic factors into target tissues using plasmid DNA or viral vectors.
c. Cell-Based Therapy
This strategy involves the transplantation of autologous or allogeneic cells capable of promoting angiogenesis through paracrine signaling or direct incorporation into nascent vasculature.
d. Tissue Engineering and Biomaterials
Engineered scaffolds and hydrogels loaded with angiogenic factors or cells can provide structural support and localized delivery, creating a pro-angiogenic microenvironment.
B. Anti-Angiogenic Therapies
Anti-angiogenic therapies are designed to inhibit or normalize aberrant blood vessel formation. These approaches are crucial in diseases where excessive, disorganized, or persistent angiogenesis drives disease progression, particularly in cancer, chronic inflammation, and ocular neovascular disorders. By targeting the angiogenic cascade, these therapies aim to starve pathological tissues of oxygen and nutrients, restore vascular homeostasis, and mitigate tissue damage.[40,41,42,43]
Diseases Commonly Treated with Anti-Angiogenic Therapies
Therapeutic Strategies and Representative Examples
a. VEGF Inhibition
Vascular Endothelial Growth Factor (VEGF) is a key mediator of pathological angiogenesis in tumors and retinal diseases. Therapeutic inhibition of VEGF signaling constitutes a central approach in anti-angiogenic therapy.
Therapeutic Impact: These agents inhibit neovascularization, reduce vascular leakage and edema, improve visual acuity, and slow disease progression.
b. Tyrosine Kinase Inhibitors (TKIs)
TKIs are small-molecule inhibitors that block intracellular signaling cascades downstream of VEGF receptors and other angiogenic receptors.
Clinical Role: TKIs offer broader target inhibition and are often employed when resistance to monoclonal antibodies emerges.
c. Vascular Disrupting Agents (VDAs)
VDAs target existing tumor vasculature rather than preventing new vessel growth, leading to rapid vascular collapse and tumor necrosis.
d. Endogenous Inhibitors and Anti-Angiogenic Peptides
Naturally occurring inhibitors of angiogenesis derived from extracellular matrix components or circulating proteins are under investigation for therapeutic use.
e. Combination Therapies
Combining anti-angiogenic agents with chemotherapy, immunotherapy, or radiotherapy has shown synergistic effects, improved clinical outcomes, and reduced drug resistance.
Natural Compounds and Angiogenesis
Natural compounds derived from plants have emerged as a valuable source of anti-angiogenic agents, offering a complementary or alternative strategy to synthetic drugs. These phytochemicals exhibit the ability to modulate key pathways involved in angiogenesis, including the inhibition of VEGF signaling, endothelial cell proliferation, migration, and tube formation. Due to their multi-targeted mechanisms, lower toxicity, and structural diversity, plant-derived compounds are being extensively investigated for their potential in treating angiogenesis-dependent diseases such as cancer, diabetic retinopathy, and rheumatoid arthritis.
Table 2: Plant-Derived Anti-Angiogenic Agents [43,44,45,46,47,48,49]
|
Compound/Food |
Source Plant/Food |
Activity (Angiogenic / Anti-Angiogenic) |
Molecular Target / Mechanism |
|
Resveratrol |
Grapes, Berries, Red Wine |
Anti-Angiogenic |
Inhibits VEGF and VEGFR-2, MAPK, HIF-1α |
|
EGCG (Epigallocatechin gallate) |
Green Tea |
Anti-Angiogenic |
Inhibits VEGF, PI3K/Akt, NF-κB |
|
Curcumin |
Turmeric |
Anti-Angiogenic |
Inhibits VEGF secretion, NF-κB/VEGF, MMP-2/9 |
|
Apigenin |
Parsley, Onion, Grapes |
Anti-Angiogenic |
Reduces VEGF, COX-2, NF-κB |
|
Quercetin |
Onion, Apple, Tea |
Anti-Angiogenic |
Inhibits VEGF, COX-2, PI3K/Akt |
|
Nobiletin |
Citrus Fruits |
Anti-Angiogenic |
Inhibits NF-κB, HIF-1α, MMP-2 |
|
Myricetin |
Fruits, Berries, Tea |
Anti-Angiogenic |
Suppresses PI3K/Akt/mTOR |
|
Hydroxytyrosol |
Olives, Olive Oil |
Anti-Angiogenic |
Inhibits VEGFR-2, Akt, MMP-2 |
|
Gallic Acid |
Tea, Berries, Walnuts |
Anti-Angiogenic |
Suppresses VEGF, HIF-1α |
|
Lycopene |
Tomato |
Anti-Angiogenic |
Downregulates VEGFR-2, increases IL-12, IFN-γ |
|
Fucoxanthin |
Brown Algae |
Anti-Angiogenic |
Suppresses MMP-9, FGF-2, PI3K/Akt |
|
Astaxanthin |
Microalgae, Seafood |
Anti-Angiogenic |
Inhibits ERK/MAPK, PI3K/Akt |
|
Piperine |
Black Pepper |
Anti-Angiogenic |
Inhibits ERK1/2, Akt, MMP-2/9 |
|
Ursolic Acid |
Apple, Rosemary |
Anti-Angiogenic |
Inhibits VEGF-A, FGF-2, HIF-1α |
|
Triphala |
Amla, Haritaki, Bibhitaki |
Anti-Angiogenic |
Inhibits VEGFR-2 phosphorylation |
|
Ginsenosides |
Ginseng |
Anti-Angiogenic |
Inhibits neovascularization |
|
Taxol |
Pacific Yew Tree |
Anti-Angiogenic |
Inhibits HIF-1α, VEGF |
|
Silymarin |
Milk Thistle |
Anti-Angiogenic |
Downregulates VEGF, MMP-2 |
|
Ginsenoside Rg1 |
Ginseng (Panax ginseng) |
Angiogenic |
Stimulates endothelial cell proliferation via VEGF signaling |
|
Arjunolic Acid |
Terminalia arjuna |
Angiogenic |
Enhances nitric oxide production and VEGF expression |
|
Astragaloside IV |
Astragalus membranaceus |
Angiogenic |
Promotes VEGF and bFGF secretion in endothelial cells |
|
Ursolic Acid (at low dose) |
Apple, Basil, Rosemary |
Angiogenic |
Activates VEGF-A and FGF-2 pathways |
|
Ferulic Acid |
Wheat bran, Rice bran |
Angiogenic |
Enhances VEGF-mediated angiogenic signaling |
|
Shikonin |
Lithospermum erythrorhizon |
Angiogenic |
Induces angiogenesis through HIF-1α and VEGF |
|
Procyanidin B2 |
Grape seeds, Apples |
Angiogenic |
Stimulates angiogenesis via VEGF and FGF-2 |
|
Baicalein |
Scutellaria baicalensis |
Angiogenic |
Increases VEGF expression and tube formation |
|
Emodin |
Rheum palmatum (Chinese rhubarb) |
Angiogenic |
Promotes endothelial cell growth and angiogenic factors |
Nutraceuticals And Functional Foods In Angiogenesis Regulation [50,51,52]
Angiogenesis, the formation of new blood vessels from pre-existing vasculature, plays a dual role in human health. While essential in wound healing and tissue regeneration, uncontrolled angiogenesis is a hallmark of diseases such as cancer, diabetic retinopathy, and chronic inflammation. Both nutraceuticals and functional foods have shown potential in modulating angiogenesis—either promoting it when needed (pro-angiogenic) or inhibiting it in pathological conditions (anti-angiogenic).
Nutraceuticals as Modulators of Angiogenesis
Several nutraceutical compounds derived from natural sources exhibit significant activity in influencing blood vessel formation.
Conversely, some vitamins exhibit angiogenic potential.
Functional Foods Influencing Angiogenesis
Functional foods, which provide health benefits beyond basic nutrition, also play a pivotal role in angiogenesis regulation.
Some functional foods support angiogenesis in beneficial ways, particularly in healing and vascular repair.
Emerging Trends and Future Directions in Angiogenesis Therapy [53,54]
A. Nanotechnology in Angiogenesis Therapy
Nanotechnology is revolutionizing cancer treatment by enabling more precise targeting of tumor blood vessels. Tiny particles (nanocarriers) can be designed to:
Future direction: Smart nanoparticles that can respond to the tumor’s environment (e.g., acidic pH or hypoxia) to release drugs only when and where needed are under development.
B. 3D Bioprinting and Tissue Engineering
3D bioprinting is being used to recreate realistic models of tumor vasculature, allowing researchers to:
Future direction: Bioprinted vascularized tumors will help test multi-drug therapies and understand resistance to anti-angiogenic agents.
C. Artificial Intelligence (AI) & Systems Biology
AI and systems biology tools are helping scientists:
Future direction: Integrating AI with genomics and imaging may lead to earlier detection of angiogenic “switches” and more precise treatment planning.
D. Personalized Medicine Approaches
Not all tumors respond the same way to anti-angiogenic drugs. Personalized medicine is about:
Future direction: Blood-based biomarkers and tumor sequencing will allow real-time monitoring of angiogenesis and rapid therapy adjustment.
E. Combination Therapies
Anti-angiogenic drugs are increasingly being combined with:
Future direction: Custom-designed combinations based on tumor type, mutation profile, and immune response are being tested in clinical trials.
F. Overcoming Resistance Mechanisms
Tumors often bypass anti-angiogenic drugs through:
Future direction: Targeting the tumor microenvironment, metabolic pathways, and using multi-target drugs can help overcome resistance.
Challenges And Limitations [55,56,57]
A. Resistance to Anti-Angiogenic Therapy
One of the biggest problems with anti-angiogenic treatments is that tumors often become resistant over time. There are several reasons for this:
B. Off-Target Effects and Toxicity
Targeting blood vessels affects both tumors and normal tissues, causing side effects such as:
These effects occur because VEGF and similar molecules are also essential for maintaining normal blood vessels in healthy tissues, not just tumors.
C. Tumor Adaptability and Complexity
Tumors are biologically complex. Even if one mechanism of angiogenesis is blocked:
D. Short-lived Benefits
While anti-angiogenic drugs can temporarily shrink tumors or slow their growth:
E. Difficulty in Clinical Translation
Many experimental therapies that show success in lab models do not work as well in humans due to:
Additionally, clinical trials for these therapies are expensive, long, and often inconclusive. Some therapies that worked in preclinical models failed to show benefit in phase II or III trials.
F. Lack of Reliable Biomarkers
CONCLUSION
Angiogenesis plays a pivotal role in both physiological homeostasis and pathological progression. This review underscores the dual nature of angiogenesis: it is essential for processes such as embryonic development, wound healing, and tissue regeneration, yet it also drives disease states like cancer, chronic inflammation, and vision-threatening disorders when dysregulated. Central molecular mediators—including vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and hypoxia-inducible factor-1α (HIF-1α)-coordinate angiogenic signaling, making them prime therapeutic targets. Current therapeutic approaches aim to either enhance or inhibit angiogenesis based on disease context. Pro-angiogenic strategies, including growth factor therapy, gene delivery, cell-based therapies, and tissue-engineered constructs, have shown promise in addressing ischemic pathologies and impaired tissue repair. Conversely, anti-angiogenic agents—particularly VEGF inhibitors and tyrosine kinase blockers—have demonstrated efficacy in managing cancers and neovascular ocular diseases. Nonetheless, clinical challenges persist, including therapy resistance, off-target toxicity, tumor microenvironment adaptability, and variability in patient response. Maintaining a physiological angiogenic balance is critical; insufficient neovascularization can lead to ischemia and delayed healing, whereas excessive or aberrant angiogenesis promotes disease progression. Hence, precise regulation of angiogenic signaling remains a fundamental therapeutic objective. Looking forward, innovations such as nanotechnology-based delivery systems, 3D bioprinting of vascularized tissues, artificial intelligence-driven therapeutic design, and personalized medicine hold great potential to revolutionize angiogenesis-targeted treatments. Future research must prioritize overcoming resistance mechanisms, optimizing targeted delivery, validating robust biomarkers, and ensuring effective clinical translation. In summary, angiogenesis represents a highly modifiable biological process with vast therapeutic implications. A deeper mechanistic understanding combined with integrative, patient-specific strategies will be essential to maximize therapeutic benefit while minimizing risk, ultimately advancing care in oncology, cardiovascular disease, and regenerative medicine.
REFERENCES


Balerao Sowmya, Zeenath Banu*, Angiogenesis: Molecular Pathways, Clinical Challenges, and Emerging Therapies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2772-2793. https://doi.org/10.5281/zenodo.15703199
 10.5281/zenodo.15703199
10.5281/zenodo.15703199
