Krishnarao Bhegde Institute of Pharmaceutical Education and Research, Talegaon Dabhade, Pune
The primary goal of any drug delivery system is to ensure that a therapeutic concentration of a drug is released at the desired site of action for a specific duration. Mucoadhesive drug delivery represents an advanced approach in novel drug delivery systems. These formulations are designed to enhance the residence time of the drug at the target site, enable rapid onset of action, improve bioavailability, bypass hepatic first-pass metabolism, and allow controlled and sustained drug release. Mucoadhesive systems can be administered through various routes, including buccal, oral, nasal, ocular, gastrointestinal, vaginal, and rectal routes. In this system, the drug interacts with the mucus layer and adheres to the epithelial surface of the mucous membrane. Mucoadhesion refers to the mechanism by which two materials typically a biological substrate and a polymer remain attached for a prolonged period through interfacial forces. It encompasses the attractive interactions between a biological surface and mucus or a mucosal membrane. This review provides an overview of mucoadhesion, its underlying theories and mechanisms, the factors influencing it, methods of evaluation, and the different types of mucoadhesive dosage forms.
A mucoadhesive drug delivery system is a specialized approach that employs polymers with bioadhesive properties materials that become adhesive upon hydration to deliver drugs to specific sites in the body for an extended duration. Mucoadhesion can be defined as the phenomenon in which two materials adhere to one another for a prolonged period through interfacial forces. When one of these materials is biological in nature, the process is termed bioadhesion. Specifically, mucoadhesion refers to the attachment of a material to the mucosal layer of the body.
Both natural and synthetic mucoadhesive polymers are utilized in controlled drug delivery systems to ensure close and prolonged contact between the drug formulation and the target tissue. These systems allow for sustained and site-specific drug release, thereby improving therapeutic efficiency. The concept of mucoadhesion was introduced into controlled-release drug delivery in the early 1980s. Controlled-release systems maintain a consistent release of the drug at a predetermined rate.
In recent years, there has been growing interest in the use of bioadhesive polymers and copolymers for controlled drug delivery due to their numerous advantages, including:
The biological surface involved in mucoadhesion may be an epithelial tissue or the mucus layer covering it. When adhesion occurs specifically with the mucus layer, it is termed mucoadhesion, whereas bioadhesion is a broader term referring to the attachment of polymers to any biological surface. Thus, mucoadhesion is considered a subset of bioadhesion.
Advantages of Mucoadhesive Drug Delivery System:
Limitations of Mucoadhesive Drug Delivery System:
Historical Development of Mucoadhesive Drug Delivery Systems:
Over the past four decades, the concept of mucoadhesion has been widely explored for its potential to extend the residence time of dosage forms and achieve controlled drug release through various mucosal routes. Mucoadhesive formulations have significantly enhanced the bioavailability of many drugs. The first reported application of a mucoadhesive drug delivery system dates back to 1947, when gum tragacanth was combined with dental adhesive powder to deliver penicillin to the oral mucosa.
Since then, numerous natural and synthetic polymers such as sodium alginate, carboxymethyl starch (CMS), guar gum, hydroxyethyl cellulose (HEC), and tragacanth have been identified for their mucoadhesive properties. During the 1980s, polymers like polyacrylic acid, hydroxypropyl cellulose (HPC), and sodium carboxymethyl cellulose (SCMC) gained prominence in the development of mucoadhesive formulations. Since that period, the application of acrylate-based polymers in mucoadhesive drug delivery systems has grown substantially, leading to significant advancements in controlled and targeted drug delivery technologies.
Anatomy and Physiology of the Oral Mucosa
The oral mucosa acts as an adhesive and lubricating surface, allowing cells to move smoothly against each other with minimal friction. It is divided into four main regions:

Fig no1:.basic anatomy and physiology of oral mucosa
Among these, the buccal cavity is the primary site used for drug administration. The buccal mucosa, located between the inner cheek and the gums, serves as the specific anatomical site for drug delivery.
Structurally, the oral cavity consists of three main layers:
The epithelial composition varies across different areas of the oral cavity. The epithelium in the soft palate, buccal, and sublingual regions is non-keratinized, meaning it lacks ceramides and acyl ceramides lipids responsible for forming a strong barrier. As a result, the buccal and sublingual mucosa contain only small amounts of ceramides and are therefore more permeable than other oral regions.
A mucus layer covers the outer surface of these cells, playing an essential role in cell adhesion, lubrication, and mucoadhesion, which supports the attachment of mucoadhesive drug delivery systems. The buccal mucosa has a smooth and relatively stable surface, making it ideal for placing drug absorption systems.
For buccal drug delivery, adherence to the mucosal surface ensures close contact, enhances drug absorption, and allows for a longer residence time at the site of application. These characteristics make the buccal mucosa particularly suitable for sustained systemic drug delivery.
Components / Structural Features of the Oral Cavity
The oral cavity is the part of the mouth enclosed by the lips, cheeks, hard palate, soft palate, and floor of the mouth. It is divided into two main regions:
Composition of the Mucus Layer
Mucus is a clear, sticky secretion that forms a thin, continuous gel layer over epithelial surfaces. In humans, its average thickness ranges from 50 to 450 µm, and it is secreted by goblet cells present in the epithelial lining. The general composition of mucus includes:
Functions of the Mucus Layer
Role of Saliva:
Saliva is composed of 99% water and is complex fluid containing organic and inorganic material. Secretion of saliva is highest during working hours.
Mechanisms of Mucoadhesion
The process of mucoadhesion generally occurs in two main stages:
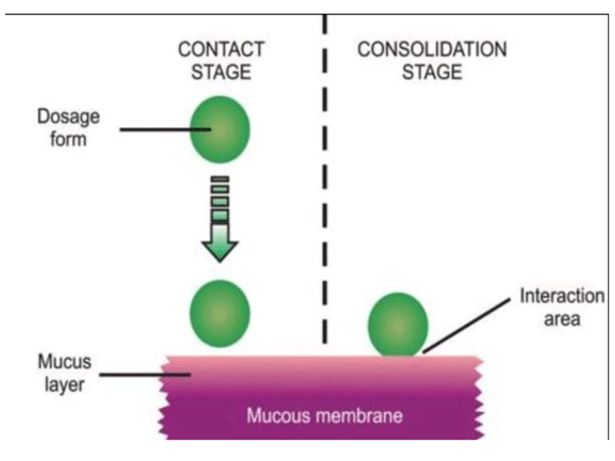
Fig no.2: Mechanism of Mucoadhesion
In the contact stage, the mucoadhesive formulation comes into initial contact with the mucous membrane, during which it begins to spread and swell, allowing for closer interaction with the mucus layer. In some delivery systems such as ocular or vaginal formulations the adhesive is mechanically applied to the mucosal surface. In other routes, like the nasal cavity, adhesion occurs naturally through aerodynamic deposition of the formulation onto the membrane.
During the consolidation stage, the mucoadhesive material becomes activated by moisture, which plasticizes the system. This allows the adhesive molecules to become more mobile and form weak interactions such as hydrogen bonds and van der Waals forces with the mucus.
There are two main theories that describe how this consolidation occurs:
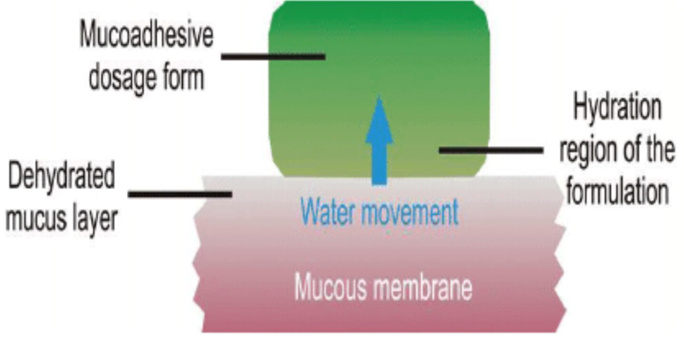
Fig no3: Dehydration theory
According to the diffusion theory, mucoadhesive molecules interact with the glycoproteins present in mucus through mutual interpenetration of their molecular chains, leading to the formation of secondary bonds between them. For this process to occur, the mucoadhesive system must possess properties that promote both chemical and mechanical interactions. According to the dehydration theory, materials capable of easily forming gels in an aqueous environment can dehydrate the mucus when they come into contact with it, as a result of the osmotic pressure difference.
Mucoadhesion theories
Mucoadhesion is a complex phenomenon explained through several proposed theories, including mechanical interlocking, electrostatic interaction, diffusion interpenetration, adsorption, and fracture processes.
Fig no 4: Various theories of mucosdhesion
Wetting theory
The wetting theory is mainly applicable to liquid systems that show an affinity for the surface, allowing them to spread effectively. This affinity can be determined by measuring the contact angle. Generally, a smaller contact angle indicates stronger affinity, and a contact angle close to zero ensures good spreadability. The spreadability coefficient, SAB, is determined by the difference between the surface energies γB and γA and the interfacial energy γAB, as shown in the related equation. This theory emphasizes the role of contact angle and the reduction of surface and interfacial energies in achieving effective mucoadhesion.
SAB = γB – γA – γAB

Fig no 5: Wetting theory
Diffusion theory
The diffusion theory explains mucoadhesion as the interpenetration of polymer and mucin chains to a sufficient depth, forming a semi-permanent adhesive bond. The strength of adhesion is thought to increase with the extent of polymer chain penetration. The rate of this penetration is influenced by factors such as the diffusion coefficient, flexibility and characteristics of the mucoadhesive chains, their mobility, and the duration of contact. According to studies, an interpenetration depth of 0.2–0.5 μm is required to achieve an effective bioadhesive bond. This depth can be calculated using a specific equation.
l = (tDb)½
In this context, t represents the contact time, and Db is the diffusion coefficient of the mucoadhesive material within the mucus. The polymer achieves maximum adhesion strength when its penetration depth is roughly equal to the length of its chains. For diffusion to take place effectively, the interacting components must exhibit good mutual solubility, meaning the bioadhesive and the mucus should have similar chemical structures. Higher structural similarity between them leads to a stronger mucoadhesive bond.
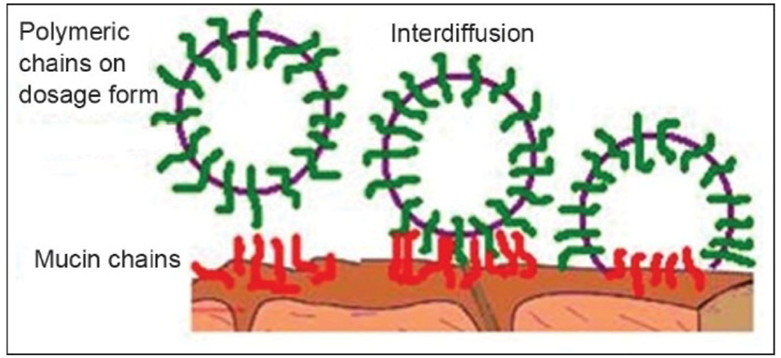
Fig no 6: Diffusion theory
Fracture theory
Fracture theory is widely applied in the mechanical assessment of mucoadhesion. It focuses on the force needed to separate two surfaces once adhesion has been formed. This force, denoted as sm, is often determined by dividing the maximum detachment force, Fm, by the total surface area, A0, that participates in the adhesive interaction. Fracture theory focuses solely on the force needed to separate adhered surfaces and does not consider the interpenetration or diffusion of polymer chains. Therefore, it is most suitable for evaluating rigid or semi-rigid bioadhesive materials, where the polymer chains do not infiltrate the mucus layer.
Sm =Fm/Ao

Fig no 7:fracture theory
Electronic theory
This theory explains adhesion as a result of electron transfer between the mucus and the mucoadhesive system, caused by differences in their electronic structures. The electron transfer leads to the formation of a double layer of electrical charges at the interface between the mucus and the mucoadhesive, generating attractive forces within this layer.

Fig no 8: Electronic theory
Adsorption theory
The adsorption theory, on the other hand, attributes adhesion to various surface interactions, including primary and secondary bonds, between the adhesive polymer and the mucus. Primary bonds, formed through chemisorption, involve ionic, covalent, or metallic interactions and are generally undesirable because of their permanent nature. Secondary bonds, which include van der Waals forces, hydrophobic interactions, and hydrogen bonding, require less energy to break and are the main type of interaction in mucoadhesion, providing semi-permanent bonding that is effective for adhesive purposes.
All these numerous theories should be considered as supplementary processes involved in the different stages of the mucus/substrate interaction, rather than individual and alternative theories. Each and every theory is equally important to describe the mucoadhesion process. There is a possibility that there will be initial wetting of the mucin, and then diffusion of the polymer into mucin layer, thus causing the fracture in the layers to affect the adhesion or electronic transfer or simple adsorption phenomenon that finally leads to the perfect mucoadhesion. The mechanism by which a mucoadhesive bond is formed will depend on the nature of the mucus membrane and mucoadhesive material, the type of formulation, the attachment process and the subsequent environment of the bond. It is apparent that a single mechanism for mucoadhesion proposed in many texts is unlikely for all the different occasions when adhesion occurs
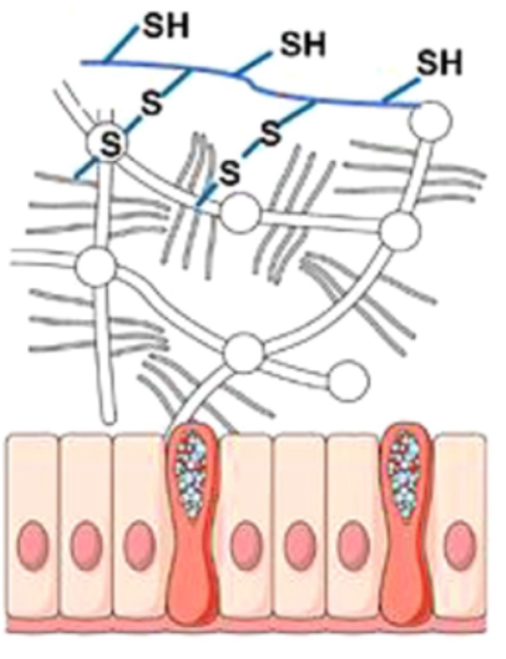
Fig no 9: Adsorption theory
Mechanical theory
Mechanical theory explains adhesion as the result of a mucoadhesive liquid filling the irregularities of a rough surface. This surface roughness also increases the available interfacial area, helping to dissipate energy, which is considered a key aspect of the process. However, mucoadhesion does not occur in the same way in all cases, so it cannot be fully explained by a single theory. Various theories are useful for identifying important factors involved in the process. The mechanisms of mucoadhesion are influenced both by the properties of the formulation and by the surrounding environment. Polymer-related factors include molecular weight, concentration, and chain flexibility. For linear polymers, higher molecular weight generally enhances mucoadhesion, whereas this relationship does not apply to non-linear polymers. More concentrated mucoadhesive formulations tend to remain on the mucous membrane for longer periods, as seen in systems that undergo in situ gelation. These formulations initially behave like liquids, allowing easy spreading, but then gel upon contact with the absorption site, which slows their removal. Chain flexibility is essential for effective interpenetration between the formulation and mucus. Environmental factors, such as pH, contact time, swelling, and physiological conditions, also affect mucoadhesion. The pH can alter ionizable groups in polymers and the charge on the mucus surface. The duration of contact between the mucoadhesive and mucus affects the degree of chain interpenetration. Excessive hydration can lead to mucilage buildup without actual adhesion. Mucus layer thickness varies widely, from 50 to 450 μm in the stomach to less than 1 μm in the oral cavity, and physiological conditions can change due to disease. No single theory or mechanism can fully account for mucoadhesion in all situations, but understanding these factors in each case can guide the development of new mucoadhesive products.
Factors Affecting Mucoadhesion
Molecular weight
The mucoadhesive strength of a polymer tends to increase when its molecular weight exceeds 100,000. For polyoxyethylene polymers, there is a direct relationship between molecular weight and mucoadhesive strength, particularly in the range of 200,000 to 7,000,000. Higher molecular weights provide longer polymer chains, which allow for greater entanglement with the mucus network, thereby enhancing adhesion.
Flexibility
Mucoadhesion begins with the diffusion of polymer chains into the interfacial region between the polymer and mucus. Therefore, the polymer chains must possess a substantial degree of flexibility to allow for sufficient interpenetration and entanglement with the mucin chains. Increased structural flexibility facilitates greater interpenetration, as observed when polymers are modified with polyethylene glycol, which enhances chain mobility. In general, the mobility and flexibility of polymers are closely related to their viscosity and diffusion coefficients, with more flexible polymers being able to diffuse more readily into the mucus layer.
Cross-linking density
Several interrelated structural parameters of a polymer network, such as the average pore size, the number and molecular weight of cross-linked polymers, and the density of cross-linking, play a critical role in mucoadhesion. An increase in cross-linking density reduces the rate at which water can diffuse into the polymer network, resulting in limited swelling of the polymer. This restricted swelling, in turn, decreases the extent of interpenetration between the polymer and mucin, thereby lowering mucoadhesive efficiency.
Hydrogen bonding capacity
The ability of a polymer to form hydrogen bonds is another key factor influencing mucoadhesion. Polymers intended for mucoadhesive applications should have functional groups capable of hydrogen bonding, and the flexibility of the polymer is important to maximize this bonding potential. Polymers such as poly(vinyl alcohol), hydroxylated methacrylates, poly(methacrylic acid), and their respective copolymers have significant hydrogen bonding capacity, which contributes to strong adhesion with the mucus.
Hydration
Hydration is essential for a mucoadhesive polymer to expand, form a macromolecular mesh of adequate size, and increase the mobility of its polymer chains. This allows better interpenetration between the polymer and mucin. Swelling of the polymer also exposes bioadhesive sites, promoting mechanical entanglement as well as hydrogen bonding and electrostatic interactions with the mucus network. However, there is a critical level of hydration at which optimal swelling occurs, providing the best conditions for mucoadhesion. Insufficient or excessive hydration can compromise the adhesive properties of the polymer.
Charge
The charge of a polymer significantly influences its mucoadhesive behavior. Generally, nonionic polymers exhibit lower adhesion compared to anionic polymers. A strong anionic charge is often required for effective mucoadhesion. Some cationic polymers can also demonstrate superior adhesive properties, particularly in neutral or slightly alkaline environments. High-molecular-weight cationic polymers, such as chitosan, are known for their good mucoadhesive performance. While there is limited information on the effect of membrane charge on mucoadhesion, the pH of the membrane can influence the ionization state of the polymer, which in turn affects adhesion.
Overall, the mucoadhesive performance of a polymer is determined by a combination of these factors, including molecular weight, flexibility, cross-linking density, hydrogen bonding capacity, hydration, and charge, all of which work together to enhance the interaction between the polymer and the mucus layer.
Methods of evaluation of mucoadhesion
No technology has been specifically developed to directly measure mucoadhesion. Most existing tests are adaptations of preexisting methods, yet they remain valuable for identifying potential mucoadhesive candidates and understanding their mechanisms of action.
In vitro and ex vivo tests
In vitro and ex vivo testing plays a crucial role in developing controlled-release bioadhesive systems. These tests help evaluate permeation, drug release, compatibility, mechanical and physical stability, interactions between the formulation and mucous membrane, and the strength of the bioadhesive bond. They can simulate various routes of administration, including oral, buccal, periodontal, nasal, gastrointestinal, vaginal, and rectal. Several widely used in vitro and ex vivo methods are discussed below.
Techniques using rat gut sacs
The everted gut sac method is an ex vivo technique that has been used since 1954 to study intestinal transport and has been adapted for mucoadhesion assays. It is simple, reproducible, and feasible in most laboratories. In this method, a segment of rat intestinal tissue is removed, everted, and one end is sutured and filled with saline. The sacs are then placed in tubes containing the formulation at known concentrations, stirred, incubated, and later removed. The adhesion percentage of the formulation is calculated by comparing the initial and residual mass.
Other variations involve using non-everted gut sacs filled with liposome suspensions. The sacs are sealed and incubated in saline, and after a defined period, the number of liposomes before (N?) and after (N?) incubation is measured using a Coulter counter. The percent mucoadhesion is calculated using the formula:
%adhesive={No-Ns/ No }* 100
Rheological Methods
Rheological methods are performed entirely in vitro and were initially introduced by Hassan and Gallo, who used viscosity measurements to study interactions between formulations and mucin on a macroscopic level. These tests allow the determination of mucoadhesive forces by observing changes in viscosity when the selected polymer is mixed with mucin. The energy from physical and chemical interactions between the polymer and mucin is converted into mechanical work, which rearranges macromolecules and results in a viscosity change.
The overall viscosity of a hydrophilic dispersion containing both mucin and a mucoadhesive polymer can be described by the contribution of each component as follows:
ηt = ηm + ηp + ηb
where is the total viscosity, is the viscosity of mucin, is the viscosity of the polymer, and represents the bioadhesion component. The bioadhesion contribution can be calculated using:
ηb = ηt – ηm – ηp
To ensure the validity of these equations, all components must be measured under identical conditions of concentration, temperature, time, and shear rate. The bioadhesion force () can then be determined from and the shear rate.
Falling Liquid Film Method
This method, adapted by Nielsen, Schubert, and Hansen from a procedure by Rango Rao and Buri, involves placing a selected mucous membrane in a longitudinally cut stainless steel cylindrical tube. The tube is inclined and positioned in a cylindrical cell maintained at 37?°C. An isotonic solution is passed over the mucous membrane and collected.
For particulate systems, the amount of material remaining on the membrane is quantified using a Coulter counter. For semi-solid systems, the non-adhered portion is measured using high-performance liquid chromatography. This method has been tested on porcine stomach, intestinal, and buccal mucus, as well as rabbit jejunum, and validation showed that the type of mucus does not significantly affect results.
The method also allows observation of liquid-crystalline mesophase formation on the mucous membrane after fluid flow, which can be analyzed using polarized light microscopy. The release systems studied included liquid crystal precursors made from monoglycerides.
Marketed products

CONCLUSION
Research on mucoadhesive systems has explored a wide range of topics and continues to be a rapidly growing field. The focus is on developing innovative devices, smarter polymers, and improved methods to better understand the mechanisms of mucoadhesion. With the continuous introduction of new drug molecules, mucoadhesive systems are likely to become increasingly important in pharmaceutical development.
REFERENCE


Sneha Bhalerao, Diya Gawade, G. K. Brahma, Aamena Simeem, Payal Shelkhe, An Overview on Mucosal Drug Delivery System, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 2866-2879. https://doi.org/10.5281/zenodo.17648960
 10.5281/zenodo.17648960
10.5281/zenodo.17648960
