Royal College of Pharmacy, Raipur, Chhattisgarh, India
"Diabetes mellitus is a chronic endocrine and metabolic disorder characterized by persistent hyperglycemia (elevated blood sugar levels) and often accompanied by multiple complications affecting various organ systems, including cardiovascular, renal, neurological, and ocular systems." Diabetes mellitus requires innovative pharmaceutical solutions to enhance treatment outcomes. This review highlights recent advancements in novel antidiabetic dosage forms, focusing on improved efficacy, safety, and patient compliance. provides an in-depth analysis of Novel formulations, mechanisms, and clinical implications.
Diabetes –
Diabetes is a frequent disease and its enormous complication is responsible. A complete lack of insulin leads to the release of carbohydrates, which is known as diabetes mellitus. Diabetes is a dangerous disease that causes billions of dollars' worth of annual difficulties in the global healthcare system. Diabetes is a collection of diseases characterized by elevated blood glucose levels and increased thirst, urination, and appetite. Diabetes affects people worldwide and has an economic impact on every country, but especially poorer nations.
At least 285 million people worldwide suffer with diabetes, according to the International Diabetes Federation. About 60% of people with diabetes worldwide live in Asia. By 2008, approximately 10% of Chinese adults suffered from an illness, up from less than 1% in 1980.[16] In France UK in the US in the 1990’s. a recent French carried out a survey during first quarter of 1999. They showed prevalence of type 2 diabetes had growing the 5.7% annually between 1994-1999. [1] The components that go into diet quality also have their own effects. The risk of diabetes is linked to higher dietary glycemic load and Tran's fat. Physical exercise is also raised and hence the lowered risk of diabetes.
Diabetes is the sixth most common cause of death worldwide. Around 171 million individuals globally, or 2.8% of the population in 2000, have diabetes, according to the World Health Organization. Diabetes is treated with insulin. The pancreas secretes the hormone insulin, which helps cells use glucose and regulate blood sugar. [17]
Insulin that acts quickly begins to function within minutes and continues for hours. Short-acting or regular insulin takes around 30 minutes to completely activate and lasts for three to six hours. 2-4 hours of intermediate acting insulin will persist up to the final 18 hours. All day long, long-acting insulin is effective. Worldwide, almost 100 million individuals require insulin. Everyone with type 1 diabetes and 10% to 25% of the population with type 2 diabetes.
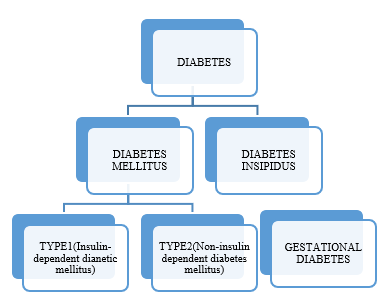
Fig 1.1: Types Of Diabetes
Insulin-
In 1921, Banting and Best made the discovery of insulin. They show how an extract of pancreas made after the exocrine portion degenerates as a result of pancreatic duct ligation has hypoglycemia effects.[23] It was originally discovered in pure crystalline form in 1926, and Sanger completely figured out its chemical composition in 1956. [23] A protein or peptide hormone is insulin. It is produced by the pancreatic beta cells. Blood sugar levels, or glucose concentration, have an impact on beta cells.[17] Insulin also prevents the liver from producing glucose. [17] Medical usage of insulin to treat specific types of diabetic mellitus. [23]
The molecular weight and amino acid composition of the human insulin protein is 51. Six Thousand. [23] The A-chain dimer contains 21 amino acids, while the B-chain contains 30.
Which are linked together by disulfide bonds. [23,17] The beta cell pancreatic islets generate insulin as the single chain peptide preproinsulin (110AA), from which proinsulin is initially made by removing 24 AAs.[23] Diabetes mellitus may develop if insulin level regulation is compromised. Protista and fungi are known to contain insulin-like proteins in addition to vertebrates.. [17] Type II diabetes mellitus may caused by Beta cell are destroyed by an autoimmune reaction insulin can no longer be synthesized or be secreted into blood. [17] The INS gene encodes the precursor of insulin known as preproinsulin. Insulin levels in the blood can be measured. International units can be used to measure blood insulin levels. [17]
Different Novel Dosage Form Of Insulin Delivery System
Oral drug delivery system of Insulin-
Insulin delivery through the digestive tract offers a convenient method. because it enables the direct distribution of insulin in the liver through the portal of entry. Protease from the gastrointestinal system quickly inactivates insulin administered orally. As an attempt to prevent insulin from degrading, liposomes are used to deliver insulin, yet even this method fails when insulin is delivered straight to the stomach. It absorbs poorly. [2, 3]
Buccal drug delivery system of insulin-
medication delivery to the systemic circulation through the buccal mucosa. The majority of buccal formulations are made to release the active component gradually. The primary site of administration for the bioadhesive system is the mucous membrane. The mucous membranes of humans are comparatively porous, facilitating the rapid absorption of drugs. A sustained release of medication over an extended period of time is achieved by mucosal buccal administration. The frequency of dosing is being reduced. [4, 3]
Rectal drug delivery system of insulin-
Insulin has been given via suppositories, which pass through the rectal mucosa. in suppositories that combine different absorption enhancers with insulin. The level of absorption of insulin is superior to the oral route. There are side effects from insulin suppositories, include soreness or urgency in the rectal area. [3, 5]
Dermal drug delivery system of insulin-
Very little insulin enters the systemic circulation through the epidermis. After applying an electrical potential, it increases the transfer of insulin via the skin (iontophoresis). Low bioavailability is the result. the insulin molecules into lipid particle vesicles. Liposomes enhanced the delivery of insulin transdermally. [6]
Nasal drug delivery system of Insulin-
Insulin is administered through the mucosa of the nose or oropharynx. Insulin is formulated in a liquid form employing mixed micelle microfine membranes and absorption enhancers to improve absorption. It was intended to be used as a buccal spray with a straightforward inhaler dosage. After 10 minutes of delivery, the spray releases a tiny particle aerosol, and insulin starts to circulate throughout the body. It was discovered that using this insulin method decreased plasma levels of c-peptide and blood glucose. At roughly 10%, bioavailability is low. Nasal insulin has a very quick start of action and rapid absorption. After 10 to 15 minutes after administration, it happens. [7]
Pulmonary drug delivery system of Insulin-
The alveolar capillary barrier facilitates the passage of inhaled insulin. After inhaling, insulin starts to circulate throughout the body 10 minutes later, reaching its maximal effect after 60 minutes. Since the effects of inhaled insulin wear off faster, there may be a lower chance of hypoglycemia during the two to four hours following meals or at night. Bioavailability of inhaled insulin was reported to be 10-20%. Patients with type 1 and type 2 diabetes have participated in clinical studies using inhaled insulin. [8, 9]
Vaginal or intrauterine drug delivery system of insulin-
Insulin distribution via the vaginal mucosa during rectal administration can help stop presystemic breakdown. Insulin is being tried intravaginally in sheep as a lyophilized powder with bioadhesive starch microsphere and as an aqueous solution with lysophosphatidylcholin. In rats, insulin is also injected intrauterine and is absorbed in a physiologically active form in the uterus. [14, 15]
Various insulin delivery devices-
Needle and Syringe-
A hypodermic needle and hypodermic syringe are used to inject liquids or gasses into bodily tissues or extract them from the body. The capacity of syringes in this range is 1 ml, 0.5 ml, and 0.3 ml. The needle is specially coated and has an extremely fine point for injection. Insulin syringes are made to fit the standard U-100. the process of diluting insulin so that one milliliter contains 100 standard insulin units. [16]
Insulin Pen-
It is injected with insulin to treat diabetics. It is used in conjunction with disposable pen needles for dose distribution and dosage measurement. Compared to the conventional vial and syringe, it is more portable and convenient. It consistently has a more precise dosage. It hurts less to inject.[17]
Insulin Pumps-
It is employed in the insulin administration process to treat type 1 diabetes mellitus. Its basal needs are met with fast-acting insulin thanks to the pattern of meals and activity. [17]
Insulin Jet Injectors-
As an alternative to T needles, the Insulin Jet Injector uses a pressurized jet of air to deliver a small spray of insulin into the skin. [20]
Insulin Patches-
Additionally, insulin patches are now being developed. However, insulin is not easily absorbed via the skin; instead, the patches release insulin gradually and constantly. Additional dose can be supplied by pulling out a tab on the patch. [20]
Insulin Inhaler-
are a novel approach to insulin delivery. Insulin inhalers function similarly to asthma inhalers, however they use the lungs to inhale dry powdered insulin into the circulation. Long-acting insulin can still be delivered because the technology can only be used to deliver fast acting insulin. [20]
Controlled Release System for insulin delivery
Controlled release system for subcutaneous delivery of insulin-
Subcutaneous injection is the classic approach of transport insulin into the body of someone with diabetes mellitus. The water soluble biodegradable triblock copolymer of poly-b-ethylene glycol-b-(D.L-Lactic acid co-Glycolic acid) (PLGA-PEG-PLGA) is an efficient injectable formulation for regulated release of insulin.Additionally, there was a steady rate of insulin release. in vivo after a single subcutaneous injection for two weeks. an insulin injection with controlled release utilizing microparticle technology.
This long-acting injectable insulin composition lowers blood glucose levels and treats diabetes by combining insulin with crystalline dextran microparticles. For the treatment of insulin-dependent or -independent patients, two patients are using a controlled release insulin formulation. Acid stabilized insulin zinc ions and zinc binding ligand are two examples of this.The rest included protamine, zinc ions, insulin, and a ligand that binds reversibly to a R state insulin hexamer's His B10 site. [10]
Controlled release system for oral delivery of insulin-
The most physiological way to administer insulin is orally, as this allows the hormone to be delivered straight from the intestine to the liver. An 80-hour research conducted in vivo on diabetic mice revealed a 20–40% drop in baseline glucose levels. An further method of delivering insulin orally involves the use of a thiolate polymer called chitosan-4-thiobutylamidine (chitosanTBA), along with insulin.
The permeation mediator lowered the glutathione. After the non-diabetic rat was given the manufactured chitosanTBA insulin tablet orally, the insulin was released in a regulated manner over a period of eight hours. [11]
Controlled release for pulmonary delivery of insulin-
Inhaled insulin proves they are clinically useful. a dry powder for insulin inhalation having a bulk median aerodynamic diameter of 1-4um. It was jointly spray dried from hyaluronic acid (HA) and recombinant human insulin. Microparticle with a biodegradable ether-anhydride copolymer that can be used as a dry powder for inhalation and controlled medication release.
[12, 13]
Advantages of controlled release drug delivery-
Current route for insulin delivery and their problems-
Present mode of administration of insulin is subcutaneous route by in which insulin is presented in body in a no physiological. Subcutaneous administration of insulin has many challenges. Insulin injected subcutaneously at least twice a day. There disadvantages local pain, inconvenience of injection. When the over dosing result itching allergy, hyperinsulinemia.
And insulin clinical trials have shown on injectable insulin treatment. then patient fail to attain lasting glycemic control due to noncompliance because of these problems, novel approach for insulin delivery are being explored include oral transdermal, nasal, rectal, pulmonary, uterine, ocular, subcutaneous implant. [20]
Problems-
Enzymatic degradation of problems-
Insulin is degraded by the git. This is due to the fact that digestive systems are made to break down peptides and proteins equally. enzymatic breakdown by pancreatic proteolytic enzymes like alpha chymotrypsin and trypsin, as well as pepsin. Insulin is broken down by luminal breakdown in the gut and acid-catalyzed degradation in the stomach.[20]
Intestinal transport of problems-
In the rat GIT, there was evidence of both active transport and biochemical evidence for insulin absorption. Researchers discovered that insulin is internalized by endocytosis after being absorbed to the apical plasma membrane. Through the endosomal route of tiny vesicles, it enters the basolateral plasma membrane and is secreted into the interstitial space. It is unknown if the surface of epithelial cells contains an insulin receptor. Erythrocytes have been shown to have insulin receptors on both their basolateral and apical surfaces. [20]
Stability problem-
The molecular structure in three dimensions is necessary for the activity protein. protein that can be broken down chemically and physically. Include structure up to a higher order structure in physical deterioration. in bond cleavage-based chemical degradation leading to the creation of new products. Proteins need to be described in terms of their size, shape, conformation, surface characteristics, and bioactivity. Spectrophotometric analysis, x-ray diffraction, differential scanning, colorimetry, and gel filtration were used to observe these alterations. A recent evaluation of research data examined the solid state stability of proteins in dose forms.[20]
Challenges to Oral Insulin Delivery-
Insulin is one example of a protein or peptide that cannot be taken orally because of fast enzymatic breakdown. Due to its large molecular weight and lack of lipophilicity, the intestinal epithelium in the stomach is able to inactivate and digest the substance using a proteolytic enzyme.
Less than 1% of proteins and peptides are bioavailable when taken orally. Improving the bioavailability to between 30 and 50 percent is the problem here. [18]
Approaches for oral insulin –
Following oral delivery, peptides are not bioavailable from the GIT. Overcoming the enzymatic and physical obstacles and taking precautions to preserve bioactivity throughout formulation processing are necessary for these effective oral insulin administrations. in creating highly bioavailable oral protein delivery methods.18]
Insulin administered via intramuscularly. It soon became clear that subcutaneous injection as a effective but considerably less traumatic.
Route of Administration
Drug delivery by membrane of the oral cavity can be classified as follows, by drug administration sites.
Subcutaneous Drug Delivery System –
Administering a drug subcutaneously involves injecting it into the adipose tissue directly beneath the skin. A bolus of subcutaneous injection is injected into the subcutis. the skin layer that lies just under the epidermis and dermis. referred known as the cutis together. Insulin can be administered very well by subcutaneous injection. When administered subcutaneously, it can result in swelling, redness, and burning sensations.[3]
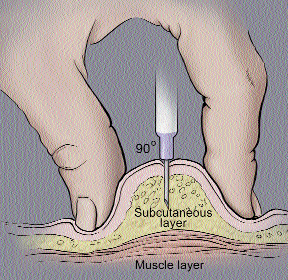
Fig. 1.2 Subcutaneous injection into the fatty layer of tissue under the skin
Intra muscular Drug Delivery System-
the injection, commonly into the thigh, gluteus, or dutoid muscles. When doctors cannot deliver an injection or no one with the necessary training is present, it might be challenging to administer an IV or even a SC injection. This method, however, is straightforward and easily accessible. When injected, intramuscular causes excruciating pain; tingling and numbers are also frequently experienced, and swelling and redness are unavoidably present.
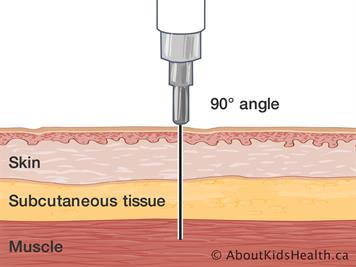
Fig. 1.3 Intra muscular injection under the skin
Buccal Drug Delivery System -
A buccal drug delivery system is a method of delivering medication through the oral cavity's buccal mucosa. The buccal mucosa, which lines the inside of the cheeks, aids in blood flow. In terms of biology, the product is used to treat a localized systemic ailment by placing it between the cheek and upper gingiva (gums). Mucoadhesive medication delivery systems are ineffective because they produce GI discomfort and decreased bioavailability. They made use of this particular polymer's distribution technique. They stick to hydration, therefore they can be used to apply a medication to a specific area of the body for a long time.
Buccal absorption:
Buccal absorption leads systemic or local action via buccal mucosa.
Mechanism of buccal absorption:
Drugs are absorbed through the buccal intercellular gaps of the epithelium by passive diffusion of the non-ionized species, which is mainly controlled by a concentration gradient. The main mode of transport is the passive movement of non-ionic species over the buccal cavity's lipid membrane. It has been suggested that the buccal mucosa acts as a lipoidal barrier to medication absorption., This is the case with many other mucosal membranes, and the medicine is absorbed more easily the more lipophillic it is.A first order rate process could properly capture the kinetics of medication absorption through the buccal mucosa. There are a number of possible obstacles to buccal medication absorption that have been found. Salivary secretion modifies the drug concentration in the mouth, which in turn affects the buccal absorption kinetics from drug solution, as noted by Dearden and Tomlison (1971).[35]
Factors affecting buccal absorption: Because there are numerous independent and interdependent variables that lower the absorbable concentration at the site of absorption, the oral cavity presents a complex environment for drug delivery.[34]
a. Saliva: Salivary pellicle or film is the term for the thin layer of saliva that covers the whole buccal mucosa. Salivary film has a thickness of 0.07 to 0.10 mm. The thickness, content and mobility of this coating determine the rate of buccal absorption.[34]
b. Salivary glands: The epithelium or deep epithelium of the buccal mucosa contains the small salivary glands. On the buccal mucosa's surface, they continuously release mucus. Mucus may act as a barrier to medication penetration even though it aids in the retention of mucoadhesive dose forms.[34]
c. Movement of buccal tissues: The mouth cavity's buccal portion moves less actively. It is necessary to use mucoadhesive polymers to maintain the dosage form in the buccal region for extended periods of time in order to withstand tissue motions during speaking, eating, and, if feasible, swallowing.[34]
Ideal Properties/Characteristics Of Buccal Drug Delivery System
Limitations of buccal drug delivery system
Advantages of buccal drug delivery System
Disadvantages of buccal drug delivery System
Method to increase drug delivery via buccal route –
High molecular weight substances, such peptides, which typically have poor buccal absorption rates, have been shown to be effectively delivered via absorption enhancers. These could work through a variety of processes, include making the cell membrane more fluid, drawing lipids from within and outside the cell, changing surface mucin, or changing cellular proteins. The most widely used substances to improve absorption are fatty acids, azone, bile salts, and surfactants like sodium dodecyl sulfate. In a tissue culture model of the buccal epithelium, mannitol and fluorescently tagged dextran were similarly found to be better absorbed by solutions or gels of chitosan, whereas glyceryl mono oleates were found to improve peptide absorption through a co-transport mechanism.
Permeation enhancers are substances that make the buccal mucosa easier to penetrate. The drug's physicochemical characteristics, the place of administration, the kind of vehicle, and additional excipients all influence the choice of enhancer and its effectiveness.
Mechanisms of action of permeation:
By reducing the viscosity of the mucus and saliva overcomes this barrier.
Disturb the intracellular lipid packing by interaction with either lipid packing by interaction with either lipid or protein components.
By inhibiting the various peptidases and proteases present within buccal mucosa, thereby overcoming the enzymatic barrier. In addition, changes in membrane fluidity also alter the enzymatic activity indirectly.
Some enhancers increase the solubility of drug there by alters the partition coefficient.
Table 1.1: Example of permeation enhancers with example
|
Category |
Examples |
Mechanism |
|
Surfactants and Bile Salts |
Surfactants and Bile Salts Sodium dodecyl sulphate Sodium lauryl sulphate Polysorbate 80 |
Acting on the components at tight junctions Increasing the fluidity of lipid bilayer membrane; |
|
Fatty Acids |
Oleic acid, Cod liver oil, Cupric acid, Lauric acid |
Increasing the fluidity of Lipid bilayer membrane. |
|
Polymers and Polymer Derivatives |
Chitosan Trimethyl chitosan Chitosan-4- thiobutylamide |
Increasing the fluidity of lipid bilayer membrane; Increased retention of drug at mucosal surface. |
|
Others |
Ethanol, Azone, Octisalate, Padimate, Menthol |
Acting on the components at tight junctions; Increasing the fluidity of lipid bilayer membrane |
BIOADHESION:[34]
‘Bioadhesive’ is defined as a substance that is capable of interacting with biological material and being retained on them or holding them together for extended period of time.
Bioadhesive are classified into three types.
1. Bioadhesion between biological layers without involvement of artificial materials. Cell diffusion and cell aggregation are good examples.
2. Bioadhesion can be represented by cell adhesion into culture dishes or adhesion to a variety of substances including metals, woods and other synthetic materials.
3. Adhesion of artificial substances to biological substrate such as adhesion of polymer to skin or other soft tissue.
Mechanism of Bioadhesion:
For bioadhesion to occur, three stages are involved:
1. a close bond between a bioadhesive and a membrane that results from the bioadhesive swelling or from a good wetting of the bioadhesive and membrane.
2. Penetration of the bio-adhesive into the tissue takes place.
3. Inter penetration of the chains of the bioadhesive with mucous takes place. Low chemical bonds can then settle.
4. Physical and chemical interactions, resulting from the expansion of the sticky material and chemical bonds caused by electrostatic interaction, hydrophobic interaction, hydrogen bonding, and dispersion forces, are the main ways that the mucus and biological substance bond.
Physiological factors affecting buccal bioavailability[36]
Insulin-
Chemical Name- 21A- Glycine-30Ba-1-arginine-30Bb-1-arginine insulin
Categories- antidiabetic
Molecular weight- 6062.955g/mole or 6063 Daltons
Molecular Formula- C267H404N72O78S6
Solubility – It is soluble in water, dilute acetic acid and dilute hydrochloric acid.
Dose - 0.5-0.8 unit/kg/day.
Pharmacokinetic -
Absorption – insulin administered via SC injection is absorbed directly into the bloodstream, with the lymphatic system playing minor role in transports.
Melting Point- 810 C.
Hydrophobicity- 0.098
Isoelectric point – 6.88.
tmax – 8 hrs.
Cmax – 13.6 mg/ml.
AUC – 329 uU/1/180min.
Distribution – circulating insulin is distributed in equilibrium between free insulin and insulin bound to IgG antibodies.
Volume of Distribution- 3.2 L/Kg.
Protein Binding- 80-90%

Fig.1.4 Structure of Insulin
Metabolism- Insulin glargine is largely metabolized in the sub-Q tissue depot to produce 2, which is metabolized with activity comparable to that of insulin.
Elimination- After seven days, 24% of the medication and its metabolites are retrieved in the urine and 69% are found in the feces.
Mechanism of Action- binding to a glycoprotein receptor on a surface cell to initiate an activity. The beta subunit of this receptor, which binds insulin-stimulated tyrosine-specific protein kinase, and the alpha subunit of this receptor bind the hormone. Insulin affects the metabolism of proteins, lipids, and glucose by activating this kinase and sending out a signal. In a diseased condition, different post-receptor phases in the action of insulin are triggered by receptor kinase activity.
Toxicity- Loss of vision and blindness, diabetic nephropathy, increased risk of heart attack, inflammatory disorder.
Administration- Administer by subcutaneous injection should not be intravenously.
Warning- Hypoglycemia is most common adverse effect of insulin, hypoglycemia reaction can cause consciousness, coma or death
Use in pregnancy and lactation- Teratogenic effects in children safe and effective over 6 yrs of age with type1 diabetes.
Drug interaction- Substances that may increase blood glucose lowering effects susceptibility to hypoglycemia for example oral antidiabetics, ACE inhibitors, disopyramide, fibrates, fluxetine, MOU inhibitors and sulphonamides.
Special Population:
Hepatic insufficiency: No studies were performed in patients with hepatic insufficiency. Increased circulating levels of insulin in liver failure. Pancreatic impairment.
Renal Insufficiency: Increased circulating level of insulin in renal failure and biliary impairment.
Obesity: Patients with increased body mass index.
Discussion of literature
Chein. et. al. 1987 When evaluating cutaneous drug delivery for insulin using the iontophoresis technique, it was discovered that systemic penetration was extremely low..[6]
K B Chaudhari. et.al. 1994 created liposomes containing insulin for oral administration and shown that the effects of oral administration equal those of subcutaneous administration of 1 U of insulin..[24]
Golomb. et.al. 1995 shown that the enzymatic breakdown is prevented by insulin administration via the vaginal mucosa. [14]
Bernkop – schnurch. et.al. 2000 conducted an in vivo investigation on the oral insulin control release system and found a reduction in the baseline glucose level..[11]
Heinmann.et. al 2001 .- found that insulin's new oral medication delivery system. They clarify that administering insulin orally involves contacting the gastrointestinal tract and distributing it to the liver if the insulin is encapsulated in the liver.[2]
Modi. et.al .2002 developed a liquid insulin formulation that uses an easy inhalation dosage, combined microfine membranes for improved absorption, and.[7]
Shenoy. et.al. 2003 discussed the use of microparticle technology to provide regulated release of insulin by injection. Regarding the long-acting injectable insulin composition for treating diabetes and blood glucose levels that contains crystallized dextran microparticles.[10]
Blair. et.al. 2003 revealed in a controlled-release insulin pulmonary administration tablet dry powder having a mass median aerodynamic diameter of 1-4 u for insulin inhalation. [12]
Hanes. et.al. 2003 produced as microparticles, they clarify that they can be used to administer controlled medication release and can be inhaled as a dry powder utilizing a copolymer of biodegradable ether and anhydride.13]
Kim .et.al. 2003 formulated a successful injectable. A water soluble, biodegradable triblock copolymer of poly-b-ethylene glycol-b-(D.L. Lactic acid co-glycolic acid) (PLGA-PEG-PLGA) is used to release insulin under regulated conditions.and the insulin release demonstrated a steady rate of insulin release.[26]
Hermansen .et.al. 2004 described as the discovered gene SHIP2, which controls insulin. These genes can be used to treat type 2 diabetes because they enhance insulin regulation.[19]
Kinesh. et. al 2010 discussed the general difficulties with the oral drug delivery strategy for insulin and came to the conclusion that the stomach's quick enzymatic breakdown makes oral insulin administration impossible.[18]
Vershney. et. al examined the clinical trials involving injectable insulin therapy and found that patients were unable to maintain a stable blood sugar level due to a variety of issues with enzymatic degradation, intestinal transit, and stability.[20]
R. Shaikh et. al 2011 The review included a number of topics, including mucoadhesive materials, factors that influence mucoadhesion, methods of evaluation, and ultimately, mucoadhesive drug delivery systems, including buccal, nasal, ophthalmic, gastro, vaginal, and rectal.[28]
Al- Tabakha et al.2008 They proposed that pharmaceutical corporations are using non-invansive insulin delivery to lessen injection-related pain and hypoglycemia incidents in an effort to increase patient compliance.[27]
J. Belmin et al. 2003 A recent study that did not involve older participants stressed the significance of maintaining strict glycaemic control to avoid problems. Eighty years after its development, subcutaneous insulin remains a primary treatment for diabetes. When oral antihyperglycemic medications, diet, and exercise don't produce the desired metabolic control in type 2 diabetes, it's utilized as a first-line treatment. Other insulin delivery methods, such as oral, cutaneous, and rectal, have been investigated as alternatives to injections, but they were not proven to be suitable for clinical usage. The fascinating properties of combining nasal or buccal insulin with absorption enhancers have been demonstrated.[3]
Tuesca A et.al. 2006 found that insulin underwent destruction due of the environment of the GIT's enzymatic barrier. This is because the digestive system is meant to break down proteins and peptides without distinction.[18]
Agarwal V et al. 2001 They clarified that pepsin and pancreatic proteolytic enzymes like trypsin and ?-chymotrypsin degrade insulin enzymatically.[18]
Patki VP et al. 1996 outlined how insulin is degraded by acid in the stomach, luminal degradation in the colon, and intracellular degradation; it is not susceptible to proteolytic breakdown by brush border enzyme.[18]
Lee VH et al. 1991 They came to the conclusion that less than 1% of most peptides and proteins were bioavailable orally. The task at hand is enhancing the bioavailability to a range of 30 to 50 percent.[18]
N. G. Raghsvendra et. al. 2013 demonstrated that the study of mucoadhesive polymers offers a useful perspective on mucoadhesion and a few variables that can influence a polymer's mucoadhesive characteristics. Mucoadhesive buccal patches are prepared using both natural and synthetic polymers. Furthermore, research has been done on the creation of controlled or slow release delivery systems for both local and systemic treatment of disorders affecting the oral cavity.[31]
M. Patel et.al. 2011 They looked over the systemic formulation and the buccal medication delivery method. By avoiding first pass metabolism contact with the mucosal surface, it improves bioavailability and results in a longer and better resident period. Additionally, it was determined that the majority of medications can be administered via buccal drug delivery, for all substances..[30]
Hussain et.al.2013 They conducted research on the oral mucosa, medication penetration barriers, various dose forms, evaluation techniques, and the challenges related to formulation design..[32]
CONCLUSION
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
REFERENCES

Neha Giri, Advances In Diabetes Management: A Comprehensive Review of Novel Formulations for Optimized Insulin Delivery, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 884-897. https://doi.org/10.5281/zenodo.14323213
 10.5281/zenodo.14323213
10.5281/zenodo.14323213
