Department of Pharmaceutics Krishna Foundations Jaywant Institute of Pharmacy, Wathar.
Cancer is known as the most dangerous disease in the world in terms of mortality and lack of effective treatment. Research on cancer treatment is still active and of great social importance. Since 1930, chemotherapeutics have been used to treat cancer. However, such conventional treatments are associated with pain, side effects, and a lack of targeting. Nano medicines are an emerging alternative due to their targeting, bioavailability, and low toxicity. Nano medicine in cancer therapy utilizes engineered nanoparticles (1-100nm) to improve drug delivery precision, reducing systemic toxicity while enhancing efficacy. These carriers, including liposomes, micelles, and gold nanoparticles, target tumours via passive (EPR effect) or active mechanisms, enabling better accumulation in cancer tissues. Magnetic nanoparticles (MNP) play a crucial role in the field of Nano medicine due to their magnetic properties making them valuable as drug delivery carriers, tracking agents capable of operating in different magnetic fields and as heat sources. The research that led to this invention proposes an innovative approach to promote the interaction between immune cells and nanoparticles, creating a system of immunorelease loaded with the maximum dose of magnetic materials and with the minimum cytotoxicity to immune cells, for the release and accumulation of MNPs and NK cells in the target tumour site so as to combine magnetic hyperthermia (MHT) with immunotherapy. Since FDA approval for Doxil®, several Nano-therapeutics have been developed, and a few have received approval for use in cancer treatment. Along with liposomes, solid lipid nanoparticles, polymeric nanoparticles, and Nano emulsions, even newer techniques involving extracellular vehicles (EVs) and thermal nanomaterial’s are now being researched and implemented in practice. This review highlights the evolution and current status of cancer therapy, with a focus on clinical/pre-clinical Nano medicine cancer studies. Insight is also provided into the prospects in this regard.
Cancer
Cancer is a group of over 200 disease characterized by uncontrolled growth and spread of abnormal cells caused by DNA mutation. Damaged cells divide uncontrollably often forming tumour that can invade nearby tissue or spread via the blood or lymphatic system.
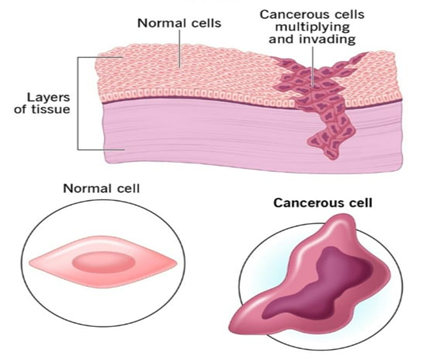
Fig.1-Development of Cancerous Cell
Cancer can start almost anywhere in the human body,which is made up of trillions of cells. Normally,human cells grow and multiply to form new cells as the body needs them. When cells grow old or become damaged,they die, and new cells take their place.
Cancer is a leading cause of death worldwide, posing a severe threat to human health. In 2022 alone, there were an estimated 20 million new cancer cases and nearly 10 million deaths globally.
Types of Cancer –
1. Carcinomas -The most common type, forming in the skin or tissue lining organs.
2. Sarcomas -Develop in bone, cartilage, fat, muscle or tendon.
3. Leukaemia -Cancer of the bone marrow that creates blood cells.
4. Lymphoma -Cancer that begins in the lymphatic system.
5. Myeloma -Develop from abnormal plasma cells in bone marrow.
Common Cancer Types by Sites –
1. Breast cancer - Affects breast tissue; symptoms include lumps and nipple changes
2. Lung cancer -Includes non-small cell [NSCLC] and small cell [SCLC]; linked to smoking
3. Colorectal cancer -Affects the colon and rectum; often arises from polyps
4. Prostate cancer -Affects the prostate gland, common in older men
5. Skin cancer -Main types include basal cell, squamous cell and melanoma
6. Blood cancer -Affects blood forming tissue and immune cells [Leukaemia / Lymphoma]
7. Gynaecological cancer -Cervical, ovarian, and uterine cancers
8. Other common types -Pancreatic, Bladder, Kidney, Thyroid, Head and Neck Cancer
Development of Cancer –
Cancer arise when DNA damage is not repaired, causing cells to ignore signals to stop dividing or die Apoptosis. These cells multiply ,forming tumour that can invade other tissue .While some risk are avoidable [Smoking ,Diet] ,others are not ,and cancer often result from a combination of factors over many years.
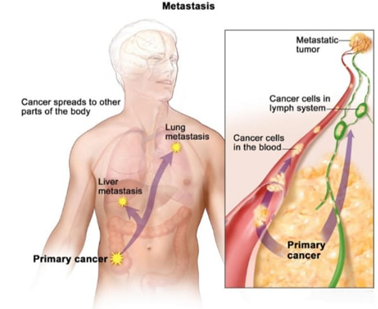
Fig.2 - Metastasis
1. Genetic Mutation -Cancer is a genetic disease caused by changes to genes that control cell function ,particularly division.
2. Uncontrolled Growth -While normal cells stop growing or die ,cancer cells continue to divide and accumulate.
3. Accumulation of Changes -It usually takes multiple ,specific mutation over time for a normal cell to bocome cancerous.
4. Tumor Development -These extra cells can form a mss clled a tumor.Note not all cancer form tumor.
5. Metastasis -Cancer cells can break away from the primary tumor and travel through the blood or lymph system to form new tumor elsewhere.
Causes of Cancer -
1. Lifestyle Habits – smoking is the leading preventable cause, contributing to lung and numerous other cancers. Other factor include high alcohol consumption, poor diet, lack of physical activity, and obesity.
2. Environmental Exposures – ultraviolet [UV] radiation from the sun or tanning beds cause skin cancer.
3. Infection and viruses – certain viruses and infection, such as human papillomavirus [HPV] and Hepatitis B and C causes liver cancer.
4. Genetic cancer – while most cancers are caused by acquired mutations by genes from parents.
5. Age – risk significantly increases with age because cells have more time to accumulate mutations.
Common signs of cancer –
1. Unexplained Weight Changes – losing 10 pounds or more without trying can be an early sign of cancer, such as stomach or lung cancer
2. Fatigue – extreme tiredness that does not improve with rest
3. Lumps or Thickening – new lumps under the skin, especially in the breast, neck, or groin.
4. Skin Changes – new moles, changes to existing moles, or jaundice.[yellowing of skin / eye]
5. Persistent Cough or Hoarseness – cough that does not go away or voice changes.
6. Pain – persistent, unexplained pain, particularly in the bones or back.
7. Bleeding or Bruising – unusual bleeding, such as coughing up blood, vomiting blood, unexplained bruising
Types of Cancer Treatments –
Cancer therapy aims to cure, control, or palliate cancer through methods like surgery (removing tumours), chemotherapy (drug-based cell killing), radiation (high-energy targeting), immunotherapy (boosting the immune system), targeted therapies (blocking specific genetic mutations), and hormone therapy. Treatments are tailored to the cancer type, stage, and patient health.
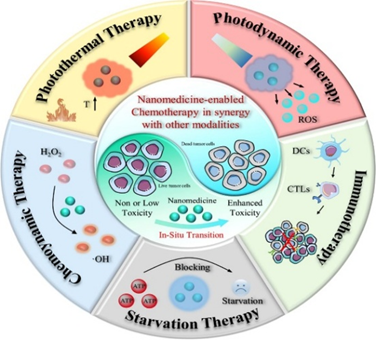
Fig. 3-Common Therapy Used In Cancer Treatment
Common Cancer Treatment Modalities –
1. Surgery – physical removal of the tumor, including robotic and organ preserving technique.
2. Radiation Therapy – high energy rays [X-ray, proton] used to destroy cancer cells, either externally or internally.
3. Chemo Therapy – drugs administered orally or intravenously to kill fast growing cells.it uses cytotoxic drugs.
4. Immuno Therapy – boosts the body natural immune system to recognise and attack cancer cells. [Examples. Include checkpoint inhibitors and CAR T-cell therapy].
5. Hormone Therapy – blocks the body`s natural hormones that feed certain cancers, such as breast or prostate.
6. Targeted Therapy – drugs that specifically target molecular changes in cancer cells that help them grow.
7. Stem Cell Transplant [Bone Marrow Transplant] – replace bone marrow destroyed by high dose chemotherapy or radiation.
8. Photo Thermal Therapy [PTT] -Is a invasive, high precision cancer treatment that uses light -absorbing agents [typically nanoparticle] to convert near -infrared light into localized heat ,causing tumour cell death through necrosis or apoptosis.
9. Photodynamic Therapy -It uses a light -sensitive medication [photosensitizer] and a specific light wavelength to destroy abnormal cells.
10. Starvation Therapy -It supress tumour growth by depriving cancer cells of essential nutrients ,oxygen ,and blood supply.it utilize strategies like ant angiogenesis ,vascular disruption ,and glucose oxidase -mediated metabolic disruption to trigger cancer cell.
11. Chemo dynamic Therapy [CDT] -relies on Fenton type reaction, often utilizing iron based nanomaterial to convert tumour localized into cytotoxic radicals that damage cancer cell DNA and proteins .Smart nanomedicines are designed to activate only upon encountering tumor conditions.
Table.1-Recent advancements in cancer Nano formulations.
|
Therapeutic modality |
Proprietary name (year) |
Composition |
Cancer indication |
|
Chemotherapy |
MagNeo (2024) |
Iron oxide NPs |
Breast cancer |
|
CNSI–Fe (II) (2023) |
Injectable ferrous sulfate with nanoparticle carbon |
Solid tumor |
|
|
Ursolic acid nano-liposomes (2023) |
Ursolic acid nano-liposomes for injection |
Hepatocellular carcinoma |
|
|
Nano-QUT (2022) |
Quercetin-encapsulated PLGA-PEG NPs |
Tongue squamous cell carcinoma |
|
|
D3S-001 (2022) |
D3S-001 monotherapy or combination therapy |
Solid tumor with KRAS P.G12C mutation |
|
|
Irinotecan hydrochloride (nano) micelles for injection (2021) |
Irinotecan hydrochloride (nano) micelles for injection |
Advanced colon cancer |
|
|
ABI-009 (2018) |
Albumin-bound rapamycin NPs |
Glioblastoma |
|
|
CPC634 (2018) |
Docetaxel micellar |
Ovarian cancer |
|
|
EndoTAG-1 (2016) |
Liposomal paclitaxel |
Breast cancer |
|
|
MM-302 (2014) |
Human epidermal growth factor receptor 2 (HER2)-targeted liposomal doxorubicin hydrochloride |
Breast cancer |
|
|
CRLX101 (2012) |
NPs consisting of camptothecin–cyclodextrin conjugate |
Stomach, gastroesophageal, esophageal cancer |
|
|
NK105 (2012) |
Paclitaxel micelle |
Breast cancer |
|
|
NKTR-102 (2011) |
Irinotecan PEG conjugate |
Breast cancer |
|
|
ThermoDox (2009) |
Thermally sensitive liposomal doxorubicin |
Breast cancer |
|
|
NC-6004 (2009) |
Cisplatin micellar |
Pancreatic cancer |
|
|
NKTR-102 (2008) |
Irinotecan PEG conjugate |
Breast cancer, glioma, ovarian cancer |
|
|
CT-2106 (2006) |
Camptothecin polymer conjugate |
Colorectal cancer, ovarian cancer |
|
|
CT-2103 (2005) |
Paclitaxel polymer conjugate |
Ovarian, peritoneal cancer |
|
|
Liposomal Annamycin (2005) |
Liposomal annamycin |
Leukemia |
|
|
SPI-077 (2004) |
Liposomal cisplatin |
Ovarian cancer |
|
|
Radiotherapy sensitizer |
Nano-SMART (2024) |
AGuIX gadolinium-chelated polysiloxane |
Non-small cell lung cancer, pancreatic cancer |
|
NBTXR3 (2015) |
Hafnium oxide NPs |
Sarcoma |
|
|
NVX-108 (2014) |
DDFP liquid emulsion combined with radiation therapy |
Glioblastoma multiforme |
|
|
Hyperthermia |
ANCHIALE (2024) |
Iron oxide NPs |
Glioblastoma multiforme |
|
Nano Therm (2021) |
Iron oxide NPs |
Prostate cancer |
|
|
Auro Lase (2009) |
Silica core with a gold nanoshell |
Primary and metastatic lung tumors |
|
|
Auro Lase (2009) |
Silica core with a gold nanoshell |
Head and neck tumor |
|
|
Immunotherapy |
JS014(2021) |
Recombinant interleukin-21 -human serum albumin nano antibody fusion protein |
Advanced stage tumor |
|
Personalized mRNA cancer vaccine (2018) |
Personalized mRNA cancer vaccine against neoantigens |
Melanoma, colon cancer, gastrointestinal cancer |
|
|
CV9202 (2017) |
mRNA cancer vaccine in combination with anti-PD-L1 |
Non-small cell lung cancer |
|
|
DPX-survivac (2014) |
Liposomal survivin-based synthetic peptide antigens |
Lymphoma |
|
|
PNT2258 (2012) |
Liposomal DNA interference oligonucleotides PNT100 |
Lymphoma |
|
|
Vaccination with mRNA-transfected DC (2011) |
Vaccination with mRNA transfected DC |
Prostate cancer |
|
|
Tecemotide (2011) |
Tecemotide (2011) |
Prostate cancer |
|
|
dHER2+AS15 (2009) |
Truncated HER2 protein combined with the immunological liposomal AS15 adjuvant |
Breast cancer |
|
|
MAGE A3+AS15 (2008) |
Melanoma-associated antigen A3 protein in combination with AS15 adjuvant |
Melanoma, non-small cell lung cancer |
|
|
Nucleic acid nanodrug |
SGT-53 (2015) |
Liposomal p53 plasmid |
Pancreatic cancer |
|
DCR-MYC (2014) |
Lipid NP containing MYC siRNA |
Hepatocellular carcinoma |
|
|
Atu027 (2013) |
Liposomal protein kinase N3 siRNA |
Pancreatic cancer |
|
|
Pbi-shRNA STMN1 LP (2012) |
shRNA against stathmin 1 using lipid NPs |
Advanced and/or metastatic cancer |
|
|
siRNA-EPHA2-DOPC (2012) |
siRNA against EPHA2 using liposomes |
Advanced neoplasm |
|
|
ALN-VSP02 (2010) |
siRNAs against KSP and VEGFA using lipid NPs |
Solid tumor |
|
|
TKM-PLK1 (2010) |
Lipid NP containing PLK1 siRNA |
Neuroendocrine tumors and adrenocortical carcinoma |
|
|
CALAA-01 (2008) |
siRNA targeting RRM2 using TfR-targeting polymeric NPs |
Cancer, solid tumor |
|
|
Allovectin-7 (2004) |
Liposomal VCL-1005 plasmid |
Melanoma |
Nanomedicines –
Nanomedicines is the medical application of nanotechnology ,utilizing engineered material and device at the Nano scales [typically 1-100 nanometres] to diagnose,monitor,treat and prevent disease.
Key Aspects of Nanomedicine –
1. Targeted drug delivery -Nano carriers [like liposomes and polymeric micelles] protect drugs from degradation, improve solubility, and deliver them directly to diseased cells [e.g. Tumour cells], sparing healthy tissue.
2. Medical imaging [Diagnostics] -Nanoparticles, such as super paramagnetic iron oxide nanoparticles [SPIONs], enhance contrast in MRI, CT, and PET scans to detect diseases earlier, including cancer and inflammation.
3. Improved Pharmacokinetics -These system increase a drug`s half-life and bioavailability, reducing the required dosage and associated side effects.
Physico-Chemical Properties –
The nanomaterial available for cancer research can be modified in size, shape and surface characteristics for customization to treat specific tumour .size is important for travel through the bloodstream and subsequent delivery of the Nano carriers to tumour tissue. While smaller nanoparticles can accumulate more easily in the leaky blood vessels of tumour than those that are larger, they can also extravagate into normal tissue .on the other hand, larger nanoparticles cannot extravagate as easily and thus their distribution in the blood stream is highly variable. Cancer is a leading cause of death worldwide, posing a severe threat to human health. In 2022 alone, there were an estimated 20 million new cancer cases and nearly 10 million deaths globally
Nanoparticles –
Nanoparticles (NPs) have revolutionized drug delivery with their small size, large surface area, and customizable surfaces and compared to traditional methods, they have improved the pharmacokinetics and distribution of therapeutic agents. The development of NPs for biomedical applications began in the 1960s with liposomes, which encapsulated hydrophilic and hydrophobic drugs. This advancement led to further innovations like polymeric NPs, dendrimers, and micelles, enhancing drug solubility, stability, and targeting9. Over the past few decades, research in cancer nanomedicine has achieved significant milestones. A variety of NPs, including lipid-based, polymeric, and inorganic NPs, have been developed for the targeted delivery of therapeutic nucleic acids, chemotherapeutic agents, and immunotherapeutic and have been evaluated in preclinical studies. Some of these nanomedicines have progressed to clinical trials.
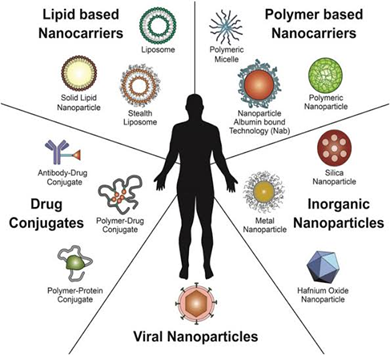
Fig.4 -Nanoparticles
Common visual representations of nanomedicine include:
1. Nanoparticles & Liposomes: 3D renderings of spherical vesicles or lipid bilayers used as drug-carrying vehicles.
2. Targeted Delivery: Illustrations showing nanoparticles releasing medication specifically to malignant cells while sparing healthy ones.
3. Nanorobots: Conceptual 3D models of microscopic robots treating blood clots or interacting with red blood cells.
4. Molecular Structures: High-resolution models of fullerenes, carbon nanotubes, and complex DNA statistics backgrounds.
5. Laboratory Research: Photos of scientists using microscopes and high-throughput screening tools to develop nano-therapeutics.
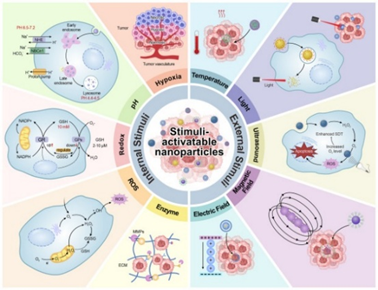
Fig.5 -Stimuli Activatable Nanoparticles
Recent advances have also integrated nanotechnology with immunotherapy to enhance antitumor immune responses. NPs have been engineered to deliver immune modulators, such as checkpoint inhibitors and cytokines, thereby stimulating the body's own immune system to recognize and destroy cancer cells. Moreover, nanomedicine-assisted imaging strategies are being employed to better statsify patients for specific treatments and monitor therapeutic responses, which significantly improves the precision and efficacy of cancer therapies. Recent cancer treatments leveraging nanotechnology have exhibited promising advancements. Such advancements incorporate stimuli-responsive, convertible, or biomimetic coatings for cell membranes; integrate prodrugs, co-assembled drugs, or cell–nanocarrier complexes with innovations like nanorobots and in vivo nano catalytic reactions; and use nano vaccines to augment immunotherapy. These advancements have collectively enhanced therapeutic outcomes for malignant tumors.
Process of nanomedicines from discovery to clinical adoption –
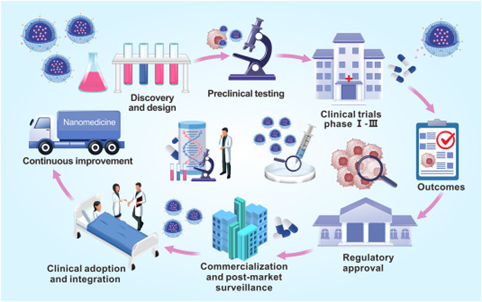
Fig.6- Process of Nano medicine from discovery to Clinical Adoption
The process of Nano medicine from discovery to clinical adoption is a multidisciplinary, multi-stage, and highly regulated journey, often described as a "bench-to-bedside" transition. It involves integrating nanotechnology with pharmacology to improve therapeutic outcomes by enhancing drug solubility, stability, and targeting efficiency. The process has moved from early liposomal research in the 1960s to over 50 approved products today, including advanced mRNA COVID-19 vaccines and cancer therapeutics.
Common Nanoparticles used in disease treatment and diagnostics –

Fig.7 -Nanoparticles in Disease Treatment and Diagnostics
Gold Nanoparticles (AuNPs): Used for imaging, drug delivery, and photothermal therapy due to unique optical properties.
Iron Oxide Nanoparticles (SPIONs): Widely used as MRI contrast agents for imaging and in targeted therapy.
Liposomes & Polymeric Nanoparticles: Popular for delivering drugs directly to disease sites, such as cancer cells, reducing side effects.
Quantum Dots (QDs): Semiconductor nanocrystals used for high-sensitivity imaging and tracking molecules.
Carbon Nanotubes (CNTs): Applied in drug delivery and biosensors for detecting diseases like diabetes.
Silica Nanoparticles: Utilized for controlled drug delivery and imaging due to their stable, tunable structure.
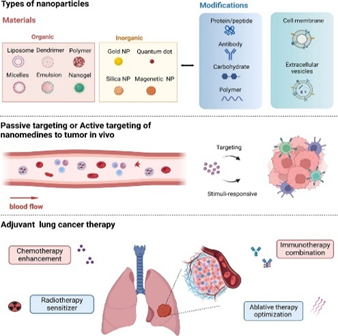
Fig.8 -Types of Nanoparticles Used In Various Therapy
1. Nanomedicine for Chemotherapy –
NP-based DDS have been a significant technological breakthrough in cancer treatment, offering fundamental improvements in therapeutic methods through the unique advantages of nanotechnology. These systems enable precise control over drug release and distribution, significantly enhancing treatment efficacy while minimizing damage to healthy cells, thereby effectively reducing patient side effects. Various types of NPs, including liposomes, polymeric NPs, and inorganic NPs, have been developed for cancer treatment.
1. Liposomes -
Liposome NPs, consisting of small vesicles made from natural or synthetic lipids, have been successfully applied in various drug delivery scenarios
Several liposomal formulation approved for clinical use -
Doxil®/Caelyx® (PEGylated Liposomal Doxorubicin): The first approved nano-drug (1995)
Myocet® (Non-pegylated Liposomal Doxorubicin): Used for metastatic breast cancer, offering reduced cardiotoxicity.
Onivyde® (Liposomal Irinotecan): Used for metastatic pancreatic cancer.
Marqibo® (Liposomal Vincristine): Approved for Acute Lymphoblastic Leukemia.
DaunoXome® (Liposomal Daunorubicin): Used for advanced HIV-associated Kaposi's sarcoma.
Vyxeos® (Liposomal Daunorubicin and Cytarabine): Used for acute myeloid leukemia.
2. Polymeric NPs –
Polymeric NPs, made from synthetic or natural polymers, can be optimized for drug delivery with immense flexibility and customization.
Several polymeric NP formulation approved for clinical use -
On Caspar® (1994): A PEG-polymer-enzyme conjugate used for treating acute lymphoblastic leukemia.
Eligard® (2002): A biodegradable PLGA-based system delivering leuprolide acetate for prostate cancer.
Genexol®-PM (2006): A PEG-PDLLA polymeric micelle containing paclitaxel, approved in Korea for breast, ovarian, and lung cancers.
Nanoxel® (2006): A polymeric micelle (PEG-PDLLA) containing docetaxel for treating breast and salivary gland cancers.
Apealea® (2018): A micellar formulation of paclitaxel approved by the EMA for ovarian, fallopian tube, and peritoneal cancers.
3. Inorganic NPs –
Inorganic NPs, such as those made from gold, silver, and silicon, leverage their unique optical and electrochemical properties to not only act as drug carriers but also enhance PTT and PDT effects.
Several inorganic NPs formulation -
Gold Nanoparticles (AuNPs)-
Formulation: AuNPs (including nanospheres, nanorods, and nanocages) are used as carriers for anticancer drugs like doxorubicin (DOX) and paclitaxel (PTX).
Mesoporous silica nanoparticles [MSNs]-
Formulation -Hollow mesoporous silica nanoparticles [HMSNs] often decorated with organic polymers e.g. PEG
Iron Oxide Nanoparticles [IONPs] –
Formulation -Silica -coated, polymer-coated [PEG, dextran], and shell-core structures.
2. Nano medicine for phototherapy and sonodynamic therapy-
Nanomedicines have led to significant technological advancements in cancer treatment, particularly in advanced therapeutic techniques such as PTT, PDT, and SDT. These methods have demonstrated the revolutionary potential of nanotechnology in medicine, providing cancer patients with more effective and precise treatment options.
Photodynamic Therapy (PDT): Involves photosensitizers that absorb light (often near-infrared) to produce cytotoxic ROS. Nanomaterials like porphyrin derivatives, Ce6, and indocyanine green (ICG) are commonly loaded into nanocarriers to improve their efficiency.
Photothermal Therapy (PTT): Utilizes materials to convert light energy into thermal energy, inducing hyperthermia to kill tumour cells. Examples include gold nanoparticles and Carbon-based materials (e.g., graphene).
Sonodynamic Therapy (SDT)- SDT uses low-intensity ultrasound to activate sonosensitizers. It offers deeper tissue penetration (>8 cm) than light-based therapies, making it suitable for deep-seated tumours.
Organic Sonosensitizers: Porphyrins, Chlorin e6 (Ce6), and Rose Bengal (RB) are commonly used, often modified to improve solubility and uptake.
Inorganic Sonosensitizers: Titanium dioxide is popular for its stability and high ROS generation. Other options include noble metal nanoparticles (Au, Ag) .
3. Nano medicine for immune therapy –
In cancer immunotherapy, nanomedicine has driven the development of tumour vaccines that precisely activate the immune system to target cancer cells while minimizing harm to healthy cells95. These tumour vaccines have been combined with other immunotherapy methods and have also been adapted for personalized medicine.
Nanomedicine has also driven the development of personalized cancer vaccines. These vaccines are tailored to each patient's unique tumor antigens, enhancing treatment specificity and providing bespoke plans for superior outcomes. Recent clinical trials have demonstrated promising results, showing that these vaccines can induce robust immune responses and improve clinical outcomes in various cancers. A melanoma trial combining a personalized mRNA vaccine with immunotherapy showed enhanced T-cell responses and significant tumor regression. Compared to patients receiving pembrolizumab alone, patients receiving mRNA and pembrolizumab had a 44%-reduced risk of recurrence or death. Nanomedicine's personalized approach offers new hope for cancer treatment by providing precise and effective tumor immunotherapy vaccines. This technology increases treatment success rates and improves patients' quality of life, showcasing nanotechnology's potential in advancing medical development
Challenges in the clinical translation of cancer nanomedicine -

Fig.9 -Translational Challenges in Cancer Nano medicine
Complexity & Manufacturing (CMC): Scaling up NP production from lab to industry while maintaining batch-to-batch consistency, stability, and sterility is challenging and costly.
Inadequate Preclinical Models: Standard animal models (CDX) do not accurately reflect the complex, heterogeneous tumor microenvironment (TME) of humans.
Low Targeting Efficiency: While designed for targeted delivery, many NPs suffer from low tumor accumulation and high off-target uptake in the liver and spleen (reticuloendothelial system).
Biological Barriers: The TME, including high interstitial fluid pressure and dense stroma, hinders deep tumor penetration.
Immune Response: Nanoparticles often trigger immune responses, such as anti-PEG IgG antibodies, leading to rapid clearance or hypersensitivity reactions.
Regulatory Uncertainty: Lack of standardized guidelines for evaluating safety, pharmacokinetics, and, particularly, "nano-specific" toxicities.
Future Opportunities in cancer nanomedicine development –
The future of cancer nanomedicine promises significant advancements in treatment. Key challenges include optimizing NP design, ensuring biocompatibility, and collaborating with regulators to streamline approvals. Advancements will involve modifying the TME to enhance immune response and reduce resistance, improving treatment outcomes. Integrating AI and big data will optimize NP design, predict patient responses, and personalize treatments. Addressing metastasis, recurrence, and side effects will expand nanomedicine's applications. A promising direction is the development of multifunctional NPs for imaging, theranostics, and combinational therapies, leading to more effective cancer treatments.
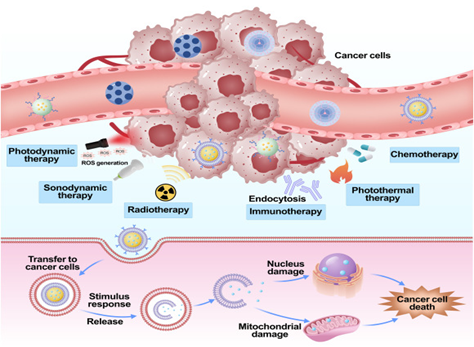
Fig.10 -Mechanism of Cancer Therapy
Integrating artificial intelligence [AI] and big data into cancer nanomedicine
AI-Guided Nanocarrier Design: AI predicts the optimal size, shape, surface charge, and ligand functionalization of nanoparticles to maximize targeting efficiency while minimizing toxicity.
Big Data Analysis for Personalization: AI processes multi-omics data (genomics, transcriptomics, and proteomics) and clinical data to create distinct molecular signatures for individual patients, enabling tailored therapy.
Advanced Diagnostics & Imaging: Nano sensors, combined with AI, detect biomarkers at extremely low concentrations (femtomolar) in liquid biopsies (blood, saliva, sweat). AI improves the accuracy of medical imaging and digital pathology (e.g., detecting metastatic breast cancer with ~99% accuracy).
Nanotheranostics: Integrating diagnostic (imaging agent) and therapeutic functions within a single nanoparticle, AI helps monitor treatment efficacy and drug release in real-time.
Overcoming Drug Resistance: AI helps identify novel biomarkers and therapeutic targets to combat multidrug-resistant (MDR) tumours, optimizing drug combinations to improve patient outcomes.
Nanotoxicity and biosafety concerns
Oxidative Stress & ROS Generation: Many nanoparticles (NPs), especially metal-based ones (e.g., Ag, ZnO, CuO), induce the overproduction of Reactive Oxygen Species (ROS). This leads to oxidative stress, which damages DNA, lipids, and proteins, causing cell apoptosis and necrosis.
Organ Accumulation & Long-Term Retention: Due to their small size, NPs can bypass natural defence mechanisms and accumulate in vital organs, particularly the liver, spleen, lungs, and kidneys. Their inability to be readily excreted raises risks of long-term chronic toxicity.
Inflammatory Responses: NPs can activate the innate immune system, leading to chronic inflammation, which is linked to diseases such as granulomas and fibrosis.
Genotoxicity: Some nanoparticles, such as carbon nanotubes (CNTs) and gold nanoparticles (AuNPs), can penetrate the cell nucleus, causing direct DNA strand breaks, mutations, and chromosomal abnormalities.
Impaired Mitochondrial Function: Internalized nanoparticles can depolarize the mitochondrial membrane and disrupt the electron transport chain, causing energy failure and cell death.
Application of Nano medicine in Cancer Therapy -
1. Targeted Drug Delivery: Nanocarriers (liposomes, micelles, nanoparticles) protect drugs from degradation, increase their circulation time, and improve solubility, delivering high concentrations of chemotherapeutics directly to tumour cells, reducing damage to healthy tissues.
2. Active vs. Passive Targeting: Passive targeting utilizes the Enhanced Permeability and Retention (EPR) effect in tumour tissues, while active targeting uses ligands to bind specific cancer cell receptors for improved uptake.
3. Stimuli-Responsive Release: Engineered nanoparticles can release drugs in response to internal stimuli (e.g., pH, redox) or external stimuli (e.g., magnetic fields, ultrasound, and temperature).
4. Enhanced Immunotherapy: Nanomedicines improve the delivery of checkpoint inhibitors and can reprogram the tumour immune microenvironment, increase T-cell infiltration and reducing regulatory T-cells.
5. Theranostics: Combining diagnostics and therapy, agents like gold or magnetic nanoparticles allow for simultaneous tumour imaging (e.g., MRI) and targeted treatment, such as hyperthermia or photothermal ablation.
6. Overcoming Resistance: Nanomedicine helps bypass biological barriers and efflux pumps that cause multidrug resistance in cancer cells.
Nanomedicine is the medical application of nanotechnology, utilizing engineered materials and devices at the Nano scale (typically 1–100 nanometres) to diagnose, monitor, treat, and prevent diseases.
REFERENCES




Sanika Shinde, Sana Shikalgar, Shravan Shinde, Suraj Jadhav, Bhagyesh Janugade, A Systemic Review on Nano Medicine in Cancer Therapy, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3500-3516. https://doi.org/10.5281/zenodo.19247709
 10.5281/zenodo.19247709
10.5281/zenodo.19247709
