We use cookies to make sure that our website works properly, as well as some ‘optional’ cookies to personalise content and advertising, provide social media features and analyse how people use our site. Further information can be found in our Cookies policy
Mucoadhesive drug delivery systems (MDDS) represent a novel approach to improve therapeutic effectiveness by utilizing the adhesive interaction between polymers and the mucosal surface. These systems enhance drug residence time, increase absorption, and bypass hepatic first-pass metabolism, thereby improving the bioavailability of drugs with poor oral absorption. MDDS have been developed for multiple routes, including oral, buccal, nasal, vaginal, rectal, ocular, and gastrointestinal delivery, using dosage forms such as tablets, films, gels, microspheres, nanoparticles, and sprays. The mechanism of mucoadhesion is explained through various theories electronic, adsorption, wetting, diffusion, and fracture and is influenced by polymer type, hydration, pH, and mucosal physiology. Both natural and synthetic polymers, including chitosan, Carbopol, and cellulose derivatives, are widely used to achieve desirable adhesion and controlled release. Evaluation parameters involve mechanical strength, bioadhesive force, swelling studies, in vitro dissolution, permeability, and in vivo pharmacokinetic assessments. Despite certain limitations, such as dose restrictions and mucosal variability, continuous advances in polymer science, nanotechnology, and smart delivery carriers are expanding the clinical potential of MDDS. With increasing patient compliance and several marketed formulations, mucoadhesive systems continue to be a promising and rapidly growing area in pharmaceutical research.
Mucoadhesion refers to the interaction occurring between the mucus layer and the bioadhesive polymer that coats the mucosal layer, involving processes such as wetting, absorption, and the interpenetration of the biopolymer chains involved [1]. These drug delivery systems are based on the concept of bioadhesion or mucoadhesion. In this, the polymer is attached to the biological surface or mucus membrane [2].
Based on the site of drug action, mucoadhesive drug delivery is classified into six types [3]:
Buccal Drug Delivery System (BDDS): Delivery of drugs through the buccal mucosa (cheek lining).
Nasal Drug Delivery System (NDDS): Drugs delivered via the nasal mucosa into systemic circulation or the CNS.
Vaginal Drug Delivery System (VDDS): Delivery of drugs through the vaginal mucosa for local or systemic effect.
Rectal Drug Delivery System (RDDS): Administration of drugs via rectal mucosa.
Oral Drug Delivery System (ODDS): Oral DDS delivers drugs through the mouth, mainly for systemic absorption via the GIT.
Gastrointestinal Drug Delivery System (GIDDS): Delivery of drugs along the stomach and intestinal mucosa.
Mucoadhesive dosage forms meet the requirements for controlled release systems [4]:
Some medications have issues with bioavailability, so they localize the medication in a specific area to increase and improve its bioavailability.
The polymers' strong interaction with the mucosal lining of tissues enhances contact time and localization of drugs, which is crucial for delivering peptides, proteins, and ionized species that require tissue permeability modification.
To stop the metabolizing enzymes in a specific location.
To locally administer the agents in order to modify antigenicity.
Advantages And Disadvantages of Mucoadhesive Drug Delivery System:
Advantages of Mucoadhesive Drug Delivery [5, 6]:
It is easy to administer.
Termination (withdrawal of dosage form) of therapy is easy in emergency conditions.
It enhanced the bioavailability by avoiding first-pass metabolism.
Longer residence time of the drug at the site of administration.
High absorption rate due to a large mucosal surface and high blood flow.
Therapeutic concentration of the drug in plasma is achieved rapidly.
It can be applied when a patient is unconscious.
High patient acceptability and better patient compliance.
To significantly reduce the dose of the drug and its adverse effects.
The absorption process takes place by passive diffusion, requiring no energy.
Disadvantages of Mucoadhesive Drug Delivery [7]:
Only a small dose of the drug is administered.
Only those drugs can be used that follow the passive diffusion mechanism of absorption.
Limitations of eating and drinking.
Sometimes, patients unwillingly swallow the dosage form.
Mucosal Membrane Anatomy and Physiology:
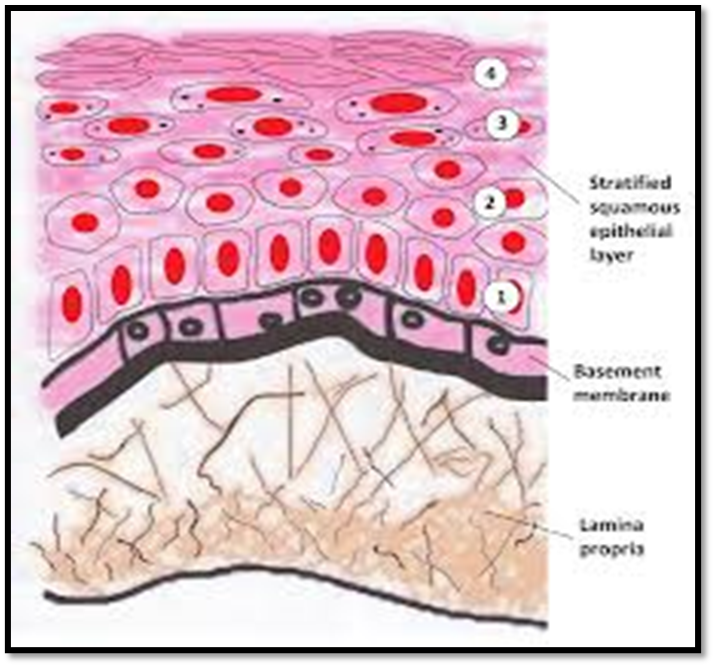
Mucosal membrane lining is present in the stomach, intestine, ureters, and bladder, also in the mouth, nose, eyelids, trachea, and lungs. The structure consists of three main layers: the epithelial layer, the basement membrane, and the connective tissue layer (lamina propria) [Fig. 01]. The epithelium layer may be either multilayered/stratified squamous epithelium or simple columnar epithelium. It contains goblet cells, which secrete mucus at the surface of the epithelial membrane. Mucus contains mucin, water, lipids, and inorganic salts, which are major components of the mucosal membrane. The important function of mucus is protection and lubrication, which provides a barrier against microorganisms [8].
Figure 1: Anatomy of mucus membrane
Mechanism Of Mucoadhesion:
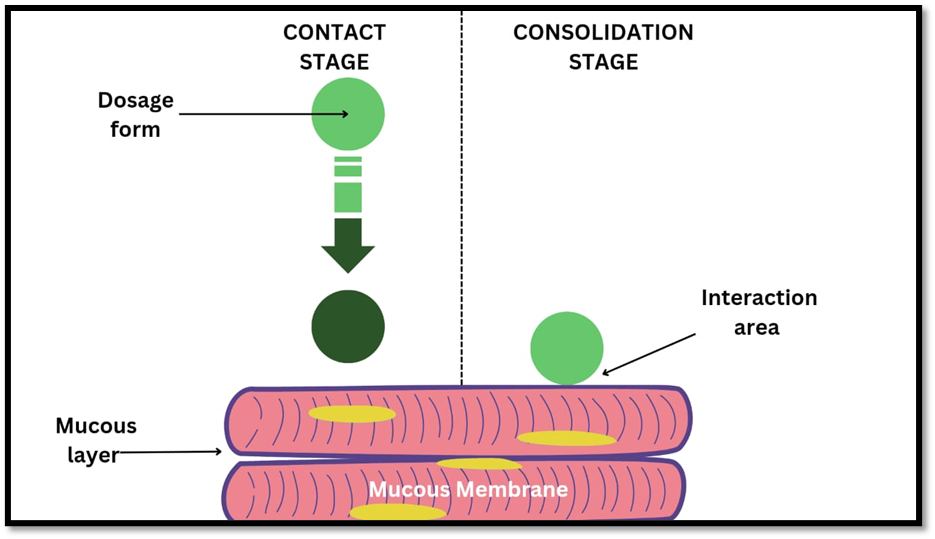
An interfacial phenomenon known as mucoadhesion occurs when two materials, one of which may be artificial, like a mucoadhesive polymer, and the other may be the mucin layer of the mucosal tissue, are held together by interfacial forces of attraction. An artificial material that can interact with mucous membranes and stay on them or hold them together for a long time is called a mucoadhesive [9]. It is divided into stages: the contact stage and the consolidation stage. (fig.02)
Contact stage: Mucoadhesive material and mucus layer interact, causing the formulation to swell and spread across the mucous membrane [10].
Consolidation stage: Moisture activates the mucoadhesive material, further plasticizing the system and enabling the molecules of mucoadhesive material to separate and connect through weak hydrogen bonds and van der Waals forces [11].
Researchers have discovered theoretical models of mucoadhesion, which are mostly based on how polymers interact with each other and with mucosal tissues. However, the mechanisms of mucoadhesion are not fully understood [12].
Chemical bond theory
Mechanical bond theory
Electronic theory
Adsorption theory
Wetting theory
Diffusion theory
Fracture theory
Chemical bond theory:
This theory states that adhesion occurs due to some type of chemical bond. Primary chemical bonds, such as covalent bonds, and secondary chemical bonds involve van der Waals forces, hydrogen bonds, and ionic bonds.
Mechanical bond theory:
This type of bonding can happen when two surfaces connect physically, similar to the way interlocking systems work. Five main theories explain the phenomenon of mucoadhesion based on the features and strengths of these interactions [13].
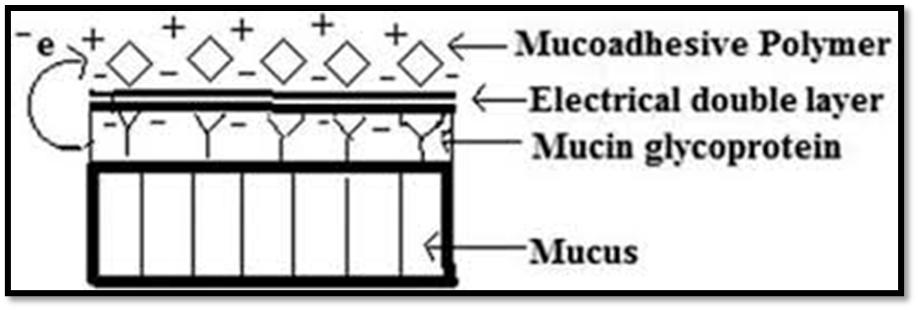
Electronic theory:
This theory states that there is a difference between the electronic structures of the mucin layer and mucoadhesive materials that results in attaining an electronic gradient. That results in electron transfer happening between them. As a result of electronic transfer, there is formation of an electronic double layer forms at the interface of the mucus and the polymer. The overall result of this process is the formation of a force of attraction between two surfaces. That's responsible for mucoadhesion between them [14].
According to adsorption theory, there is a presence of surface energy on both the surface of the biological tissue and the mucoadhesive drug delivery system. Whenever both surfaces of mucus tissue and a mucoadhesive polymer come in contact, the adhesion phenomenon can be seen due to surface energy and result in the development of chemical bonds. [15]. Absorption theory explains the involvement of both types of chemical bonds, that is, primary and secondary bonds, in the mucoadhesion mechanism. Primary chemical bonds involve covalent bonds, which are strong in nature, thus the formation of a permanent bond linkage between mucus tissue and mucoadhesive polymers. Secondary chemical bonds involve van der Waals forces, hydrophobic interaction, and hydrogen bonding, which are weak in nature; thus, the formation of semi-permanent bond linkage between mucus tissue and mucoadhesive polymers [16].
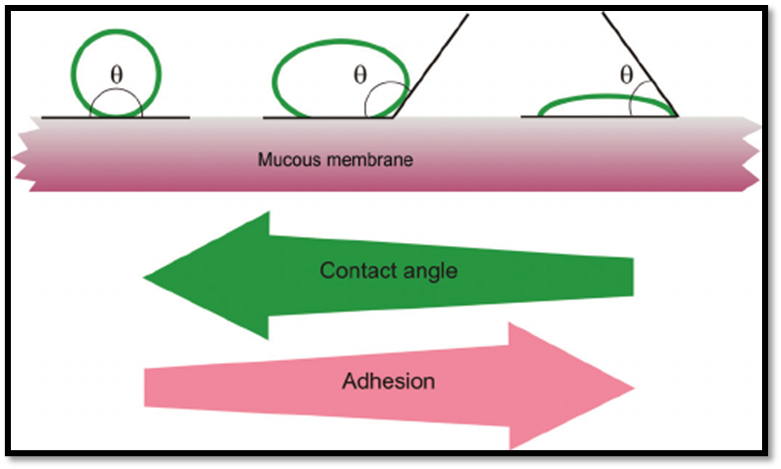
Wetting theory:
This is a theory based upon the spreadability of bioadhesive polymers and biological surfaces. These are applicable to low-viscosity liquids. According to this theory, the polymer developed contact with a biological surface. The contact angle between them should be equal or nearly close to zero to provide proper spreading. As a result, the affinity increases with decreasing contact angle [17].
The difference between surface energies can be used to calculate the spreadability coefficient, SAB.
γB & γA and the interfacial energy γAB.
The spreading coefficient formula is SAB= γB- γA -γAB
typically attributed to Thomas Young and Pierre-Simon Laplace.
The work of adhesion (Wa) given by the Dupres equation:
Wa= γB+γA -γAB.
Where A is a biological membrane and B is a bioadhesive formulation.
Figure 4: Wetting Theory
Diffusion theory:
This theory explains the interpenetration of the bioadhesive polymer chain and the mucin chain. The adhesive force increases with the increasing degree of penetration. The rate of penetration depends on the diffusion coefficient, flexibility, mobility, contact time, and nature of the mucoadhesive chain. Any crosslinking of either component tends to hinder interpenetration. It has not been specified exactly how much interpenetration is required to produce an effective adhesive bond, but it lies in the range of 0.2-0.5μm.
To calculate the interpenetration depth by the equation:
I= (tDb) ½
Where Db is the mucus and bioadhesive material's diffusion coefficient, and t is the contact time.
In order for diffusion to occur, it is important that they have a comparable chemical structure.
The greater the structural similarity results in better the mucoadhesive bond [18].
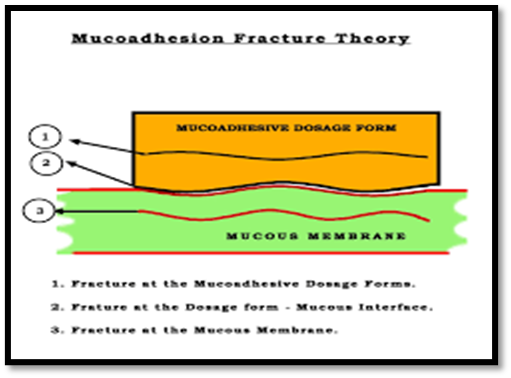
Fracture theory:
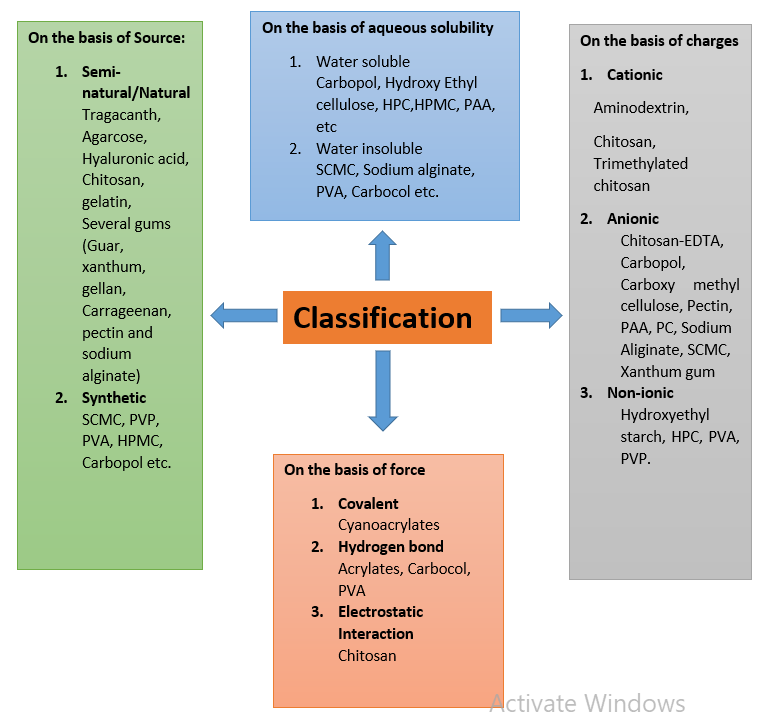
This theory is among the most widely applied approaches for evaluating the mechanical aspects of mucoadhesion. It focuses on measuring the force needed to detach two surfaces once adhesion has been established. In this context, the detachment stress(Sm) is commonly determined during rupture resistance tests by dividing the maximum detachment force (Fm) by the total contact area (A0) involved in the adhesive interaction.
Sm=FmA0
Since fracture theory only considers the force necessary to separate the surfaces, it does not account for polymer chain interpenetration or diffusion. Therefore, it is mainly applicable for evaluating rigid or semi-rigid bioadhesive systems where polymer chains lack penetration into the mucus layer [19].
Figure 5: Fracture Theory
Basic Components For A Mucoadhesive Drug Delivery System:
Active constituents:
The ideal features for choosing an API for MDDS should be selected on the basis of its [20].
Physicochemical properties
Solubility: Moderate to high solubility in mucosal fluids.
Stability: Chemically and physically stable in formulation and at mucosal pH.
Partition coefficient (log P): Appropriate for mucosal diffusion (hydrophilic/lipophilic balance).
Molecular Weight: Low to moderate (ideally less than 500 Dalton) for improved absorption.
Pharmacokinetic Properties:
High potency: because of its small absorption area, it performs effectively at low doses.
Short half-life: The mucoadhesive mechanism facilitates sustained release.
Good permeability: Able to effectively pass through the mucosal barrier.
Pharmacodynamic Properties:
Rapid onset or sustained action depending on therapeutic need.
Minimal local irritation to the mucosa.
Compatibility with Mucoadhesive Polymers:
No chemical interaction with polymers (like chitosan, HPMC, carbopol).
Maintains API activity in the presence of excipients.
Safety Considerations:
Non-toxic, non-irritant to mucosal tissues.
Pleasant taste (for oral/buccal MDDS) or odorless.
Formulation Flexibility:
Compatible with different dosage forms: gels, films, tablets, patches, microspheres.
Can withstand processing conditions (compression, drying, heat).
Bioavailability & Absorption:
It shows enhanced absorption via the mucosal route compared to the conventional oral route.
Avoids first-pass metabolism if systemic delivery is intended.
Selection of drugs according to route of administration [21]:
1) Oral/Buccal MDDS:
Drug / API Therapeutic
Class
Notes
Nitroglycerin
Antianginal
Rapid absorption through buccal mucosa; avoids first-pass metabolism
Propranolol
Beta-blocker
Used in buccal tablets or films
Fentanyl
Analgesic
For fast acting buccal films/lozenges
Clotrimazole
Antifungal
Oral candidiasis; buccal tablets/films
Acyclovir
Antiviral
Buccal tablets for herpes simplex lesions
Diazepam
Anxiolytic
Buccal fast-dissolving films
Sumatriptan
Anti-migraine
Rapid buccal absorption for fast onset
2) Sublingual MDDS:
Drug / API Therapeutic
Class
Notes
Nitroglycerin
Antianginal
Sublingual tablets for rapid effect
Buprenorphine
Opioid analgesic
Sublingual films for controlled absorption
Zolpidem
Hypnotic
Fast onset via sublingual route
3) Nasal MDDS:
Drug / API Therapeutic
Class
Notes
Sumatriptan
Anti-migraine
Nasal spray for rapid absorption
Desmopressin
Hormone
Nasal delivery to avoid first-pass metabolism
Oxytocin
Hormone
Rapid absorption via nasal mucosa
4) Vaginal/Rectal MDDS:
Drug / API Therapeutic
Class
Notes
Metronidazole
Antibacterial
Vaginal gels/tablets for local infection
Clotrimazole
Antifungal
Vaginal mucoadhesive formulations
Progesterone
Hormone
Vaginal or rectal sustained-release gels
5) Ophthalmic MDDS:
Drug / API Therapeutic
Class
Notes
Timolol
Beta-blocker
Eye gels with mucoadhesive polymers
Ciprofloxacin
Antibiotic
Mucoadhesive eye drops for sustained release
Bioadhesive polymers:
The selection of a bioadhesive polymer influences several key parameters, including mucoadhesive strength, thickness, in vitro drug release, and the residence time of the delivery system. Polymers with high molecular weight are generally preferred due to their effective control over drug release rates. An ideal polymer should possess the following characteristics to achieve optimal performance [22]:
It should be chemically inert.
It must be compatible with both the drug and the biological environment.
It should adhere rapidly to the mucosal surface and maintain long-lasting adhesion for the desired duration [23].
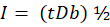
Classification of bioadhesive polymer into the following categories:
Features of ideal mucoadhesive polymers[24,25]:
It should adhere to the mucosal membrane rapidly.
Must interact strongly with mucin and epithelial tissues.
Should possess excellent spreading, wetting, swelling, solubility, and biodegradability.
Should not significantly alter the nature of the drug release.
Remain unaffected by variations in hydrodynamic conditions, food intake, or pH.
Be easy to incorporate into different drug formulations.
Exhibit peel, tensile, and shear strengths within the bioadhesive range.
Display mucoadhesive properties in both dry and hydrated states.
Have the ability to inhibit local enzymatic activity and enhance drug penetration.
Provide satisfactory stability and shelf life.
Contain adhesively active functional groups.
It possesses an optimum molecular weight.
Maintain the required spatial conformation for adhesion.
Be adequately cross-linked without suppressing bond-forming groups.
Exhibit good viscoelasticity while avoiding mucosal damage.
Backing membrane:
The backing membrane in mucoadhesive formulations should be impermeable to both the drug and mucus, preventing unwanted drug loss from the sides of the device. Materials selected for backing membranes must be inert, insoluble, or exhibit very low water solubility. Commonly used substances include ethyl cellulose, carbopol, sodium alginate, HPMC, and polycarbophil [26].
Plasticizers:
Plasticizers are added to make the drug delivery device more flexible and durable, so it doesn’t break easily when folded. This also makes the dosage form more comfortable for patients to use. Common examples include PEG-400, PEG-600, dibutyl phthalate, and propylene glycol [27].
Permeation enhancers:
Permeation enhancers are chemicals or liquids added to improve the movement of a drug from the delivery device into the mucosal membrane. They act through different mechanisms, such as:
Reducing the viscosity of mucus.
Making the membrane of the lipid bilayer more fluid.
Overcoming enzymatic barriers.
Enhancing the thermodynamic activity of the drug [28].
Factors Affecting Mucoadhesion:
Polymer-related factors:
Molecular Weight: The mucoadhesive strength of a polymer largely depends on its molecular weight and structural linearity. For linear polymers like polyethylene glycol (PEG), higher molecular weight generally leads to stronger adhesion—for example, PEG-200,000 exhibits greater mucoadhesive strength than PEG-20,000. However, in nonlinear polymers, mucoadhesive strength may not correlate with molecular weight because the helical or coiled structures can shield some adhesive groups, which are essential for adhesion [29].
Concentration of Polymer: The mucoadhesive strength of a polymer depends significantly on its concentration. There is an optimal concentration at which mucoadhesion is maximum. If the polymer concentration exceeds this optimum, the strength decreases because the polymer molecules exceed the capacity of the liquid medium, preventing proper chain formation and leaving polymer particles separated from the medium. Conversely, if the polymer concentration is too low, there are too few polymer chains per unit volume, resulting in weak mucoadhesion [30].
Flexibility of Polymer Chains: Higher flexibility of mucoadhesive polymer chains allows better diffusion into the mucus network of the buccal cavity, leading to stronger mucoadhesion. However, polymer chain flexibility decreases as polymer concentration increases. For effective bioadhesion, polymer chains must diffuse efficiently into the mucus layer. The flexibility of a polymer chain is influenced by its viscosity and diffusion coefficient [31].
Spatial Conformation: The mucoadhesive strength of a polymer also depends on its spatial arrangement or conformation, such as linear or helical. Linear polymers generally exhibit stronger mucoadhesion compared to helical polymers, because the helical structure can shield some of the active groups responsible for adhesion, reducing the polymers` overall mucoadhesive strength [32].
Swelling or Hydration: Proper hydration of a mucoadhesive polymer is essential to achieve the desired adhesion. As hydration increases, the pore size of the polymer expands, which enhances mobility and allows better interpenetration with the mucus, resulting in stronger mucoadhesion [33].
Hydrogen Bonding Capacity: Hydrogen bonding plays a crucial role in the mucoadhesion of polymers. Polymers must possess functional groups, such as –COOH or –OH, that can form hydrogen bonds with the mucus. The flexibility of the polymer enhances its hydrogen bonding potential. Polymers like polyvinyl alcohol, hydroxylated methacrylate, poly (methacrylic acid), and their copolymers exhibit strong hydrogen bonding capacity [34].
Cross-Linking Density: The cross-linking density of a polymer affects its molecular weight and pore size. Higher cross-linking density reduces the pore size, limiting water diffusion into the polymer network. This reduced diffusion decreases the polymer’s ability to penetrate the mucus, ultimately lowering its mucoadhesive strength (35].
Charge: Ionic polymers generally exhibit higher bioadhesive properties than non-ionic polymers. In neutral or slightly alkaline conditions, cationic polymers show superior mucoadhesion. For example, high molecular weight cationic polymers like chitosan are known to have strong bioadhesive properties [36].
Environment-related factors:
pH of Polymer–Substrate Interface: The pH at the polymer–mucin interface should be as closely matched as possible. Significant differences in pH between the polymer and the mucosal surface can lead to charge transfer across the interface, which may adversely affect mucoadhesive strength [37].
Applied Strength: When placing a buccal mucoadhesive device, enough pressure should be applied to ensure it sticks well to the mucosa. Even if the polymer and mucus do not naturally attract each other, applying pressure for a sufficient time can help the polymer adhere [38].
Initial Contact Time: Longer initial contact between the mucoadhesive polymer and the mucus layer allows more swelling and interpenetration of the polymer chains, which increases the mucoadhesive strength [39].
Moistening: Moistening helps the mucoadhesive polymer spread over the surface. It forms a network with pores that allow interpenetration of polymer and mucin molecules, increasing the mobility of polymer chains and promoting proper diffusion into the mucin layer [40].
Physiological factors:
Mucin Turnover: High mucin turnover negatively affects mucoadhesion. It reduces the residence time of the polymer because the polymer may detach from the mucosal layer. Additionally, soluble mucin molecules may interact with the polymer before it adheres to the mucus, leading to insufficient mucoadhesion [41].
Disease State: In certain conditions, such as Dry Mouth Syndrome or at an older age, mucus secretion is reduced. This results in insufficient mucus at the site of polymer attachment, leading to poor moistening and swelling of the polymer and, consequently, reduced mucoadhesive strength [42].
Rate of Renewal of Mucosal Cells: The renewal rate of mucosal cells varies between different types of mucosa and can limit the residence time of bioadhesive systems on the mucosal surface [43].
Concomitant Diseases: Certain diseases can change the properties or amount of mucus, such as hypo- or hypersecretion of gastric juice, fever, ulcers, colitis, tissue fibrosis, allergic rhinitis, infections, or inflammation, which can affect mucoadhesion [44].
Tissue Movement: Movements such as swallowing, speaking, food intake, and gastrointestinal peristalsis can affect the performance of mucoadhesive systems, particularly gastro-retentive dosage forms [45].
Evaluation Parameter Of Mucoadhesive Drug Delivery System:
The standard evaluation tests for mucoadhesive drug delivery devices include tensile strength, film endurance, hydroscopicity, weight variation, thickness variation, friability, hardness, content uniformity, and in vitro dissolution for tablets. Viscosity and aging effects for films and patches, so for the ointments and gels. Additionally, they should be specifically assessed for their permeability and bioadhesive qualities [46].
Bioadhesion studies:
Bioadhesion studies are generally classified into in vitro and in vivo methods.
In vitro evaluation technique
These are used to determine the dissolution, solubility, and release of the dosage form. It is performed outside biological tissue (e.g., on synthetic membranes or instruments) [47].
Tensile Strength / Detachment Force Method
This is used to measure the force required to detach a bioadhesive formulation from a biological membrane [48].
The formula is used to determine tensile strength:
Force of adhesion (N)= mucoadhesive strength × 9.81/1000
Shear Stress Method
This method is used to measure the force required to slide the adhesive system along the mucosal tissue [49].
Bond strength (N/m2)= force of adhesion (N)/surface area of tablet(m2)
Figure 6: Shear stress method
Colloidal Gold Staining Method:
This is a new method that tests the interaction of polymers with mucin to determine the qualitative interaction indicator [50].
Viscometric Method:
This method is based on the change in viscosity due to bioadhesive polymer and mucin interaction. It simply explains that the higher the viscosity, the greater the bioadhesion [51].
In vivo evaluation technique
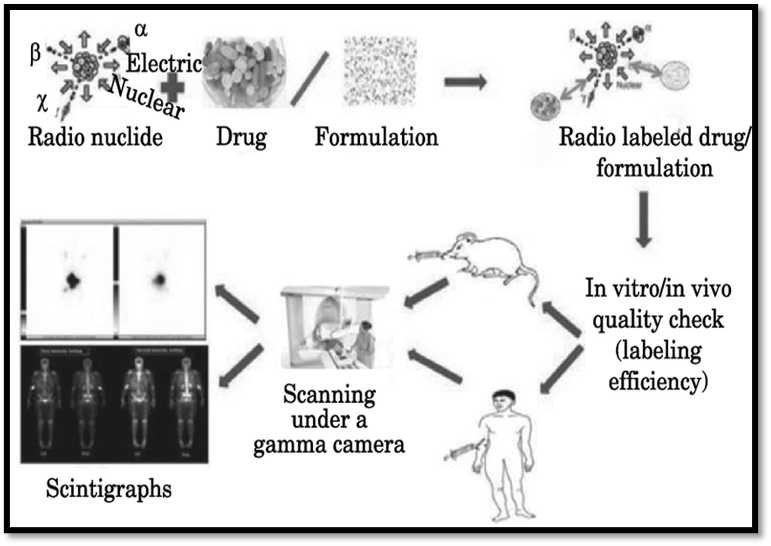
Gamma scintography techniques:
It is a non-invasive technique employed for evaluating pharmaceutical dosage forms. This method provides valuable information about various regions of the gastrointestinal (GI) tract, including the site of drug absorption as well as the location and timing of dosage form disintegration. The technique is also useful for assuming the influence of factors such as disease conditions and food intake on the biopharmaceutical performance of dosage forms. In most cases, it is applied to investigate the distribution and residence time of mucoadhesive tablets [52].
Pharmacokinetic Studies:
In the context of PK studies, it is crucial for understanding how adhesion at the mucosal site influences drug absorption and systemic availability. It leads to enhanced drug absorption, altered plasma concentration-time profile, and possibly improved bioavailability. By studying PK parameters, the effectiveness of bioadhesive systems can be quantitatively assessed [53].
Figure 7: Gamma Scintography Technique
Physical evaluation studies:
Thickness and hardness:
Thickness is a crucial parameter to ensure uniformity in tablet size and can be measured using a Vernier caliper. For evaluation, tablets are randomly selected from each batch, and their hardness is determined by a Monsanto hardness tester. The hardness values are expressed in kg/cm² [54].
Weight variation:
Weigh 20 tablets separately and then together. Calculate the average weight of the tablets and determine the % weight variation using the following formula [55].
Formula
% Wtvariation=Weight of each tablet -Average weight of tablet÷Average weight of tablet×100
Swelling index:
The degree of swelling of the dosage form when it is placed in an aqueous medium
Swelling index (SI)= W2-W1/W1×100%
Surface pH: It is used to determine the effect of the dosage form at acidic or basic pH to know mucosal irritation. It is measured by placing the dosage form in contact with a pH electrode. 6-7 pH for buccal & 4-5 pH for vaginal [56].
Current Scenario:
Mucoadhesive drug delivery systems are witnessing rapid growth worldwide, with continuous research and innovation focusing on novel polymers, nanocarriers, and advanced adhesive technologies. A wide range of formulations are being developed, not only for conventional small-molecule drugs but also for biologics such as peptides, proteins, vaccines, and nucleic acids. Recently marketed or under clinical development mucoadhesive products include Striant® (testosterone buccal system), Onsolis® (fentanyl buccal soluble film), Zuplenz® (ondansetron oral soluble film), Belbuca® (buccal buprenorphine film), and various nasal sprays such as Narcan® (naloxone). Mucoadhesive gels and patches for local delivery in periodontal, vaginal, and ocular applications are also entering the market. Although the number of commercially available formulations is still relatively limited compared to oral dosage forms, the demand for patient-friendly, non-invasive, and controlled-release systems is driving strong growth. With increasing global interest, the future is expected to bring a surge of next-generation mucoadhesive products integrating nanotechnology, smart polymers, and personalized drug delivery approaches [57].
ACKNOWLEDGEMENT:
The authors sincerely express their gratitude to Miss. A.B. Udar for their valuable guidance, encouragement, and continuous support throughout the preparation of this review article onA Review on: Mucoadhesive Drug Delivery Systems. Her insightful suggestions and expert supervision have been instrumental in shaping the quality and depth of this work. The author also extend their appreciation to their institution and colleagues for providing the necessary resources and academic environment that facilitated this study.
Conflict Of Interest:
The author declared no conflict of interest with respect to the authorship and publication of this article.
Availability Of Data and Material:
All the data used in our article are available from publically accessible sources such as PubMed, Elsevier, Wikipedia, etc.
Funding:
The authors received no financial support for the authorship and for publication of this article.
REFERENCES
Senthil KM. Mucoadhesive buccal drug delivery system—an overview. Int J PharmTech Res. 2012;4:3951-3969.
Ahmed TA, Bawazir AO, Alharbi WS, Safo MK. Enhancement of simvastatin ex vivo permeation from mucoadhesive buccal films loaded with dual drug release carriers. Int J Nanomedicine. 2020;15:4001-4020. doi:10.2147/IJN.S256925.
Kumar K, Dhawan N, et al. Bioadhesive polymers: novel tool for drug delivery. Artif Cells Nanomed Biotechnol. 2014;42:274-283.
Shinkar DM, Dhake AS, Setty CM. Drug delivery from the oral cavity: a focus on mucoadhesive buccal drug delivery systems. PDA J Pharm Sci Technol. 2012;66(5):466-500. doi:10.5731/pdajpst.2012.00877.
Khanna R, Agarwal SP, Alka A. Mucoadhesive buccal drug delivery: a potential alternative to conventional therapy. Indian J Pharm Sci. 1998;60(1):1-11.
Miller NS, Chittchang M, Johnston TP. The use of mucoadhesive polymers in buccal drug delivery. Adv Drug Deliv Rev. 2005;57(11):1666-1691.
Vyas SP, Khar RK. Controlled drug delivery—concepts and advances. 1st ed. New Delhi: Vallabh Prakashan; 2002.
Smart JD. The basics and underlying mechanisms of mucoadhesion. Adv Drug Deliv Rev. 2005;57:1556-1568.
Kaul M. An overview of buccal drug delivery system. Int J Pharm Res. 2021;13(1):1303-1321. doi:10.31838/ijpr/2021.13.01.556.
Gandhi PA. A review article on mucoadhesive buccal delivery system. Int J Pharm Res Dev. 2011;3(0974):159-173.
Boddupalli BM, Mohammed ZNK, Nath AR, Banji D. Mucoadhesive drug delivery system: an overview. J Adv Pharm Technol Res. 2010;1(4):381-387. doi:10.4103/0110-5558.76436.
Longer MA, Robinson JR. Fundamental aspects of bioadhesion. Pharm Int. 1986;7:114-117.
Dodou P, Breedveld P, Wieringa PA. Mucoadhesives in the gastrointestinal tract: revisiting the literature for novel applications. Eur J Pharm Biopharm. 2005;60(1):1-16.
Derjaguin BV, Smilga VP. The electronic theory of adhesion. In: Adhesion: fundamentals and practice. Nottingham, UK & New York: University of Nottingham and Gordon & Breach; 1996.
Bhowmik D, Niladry C. Mucoadhesive buccal drug delivery system—an overview. J Adv Pharm Educ Res. 2013;3:319-331.
Ramesh B, Saravanakumar K, Nagaveni P, Mohan Kumar A, Jaya Preethi P, Vivek Kumar P. A review on buccal drug delivery system. Int J Res Pharm Sci. 2014;5(3):200-204. doi:10.5958/0975-4377.2017.00019.2.
Varma N, Chattopadhyay P. Polymeric platform for mucoadhesive buccal drug delivery system: a review. Int J Curr Pharm Res. 2011.
Bruschi ML, Jones DS, Panzeri H, Gremião MPD, Freitas O, Lara EH. Semisolid systems containing propolis for the treatment of periodontal disease: in vitro release kinetics, syringeability, rheological, textural, and mucoadhesive properties. J Pharm Sci. 2007;96(8):2074-2089.
Hägerström H, Edsman K, Strømme M. Low-frequency dielectric spectroscopy as a tool for studying compatibility between pharmaceutical gels and mucus tissue. J Pharm Sci. 2003;92:1869-1881.
Steward A. The effect of enhancers on buccal absorption of hybrid alpha interferon. Int J Pharm. 1994;104:145-149.
Patil KH, Mobin SA. Advances in mucoadhesive drug delivery system: enhancing effectiveness of typical and biomolecule drugs. J Drug Deliv Ther. 2024;14(10):105227.
Yajaman S, Bandyopadhyay AK. Buccal bioadhesive drug delivery—a promising option for orally less efficient drugs. J Control Release. 2006;114:15-40.
Edgar WM. Saliva: its secretion, composition and functions. Br Dent J. 1992;172:305-312.
Mahajan P, Kaur A, Aggarwal G, Harikumar SL. Mucoadhesive drug delivery system: a review. Int J Drug Dev Res. 2013;5(1):11-20. doi:10.20959/wjpps20174-8863.
Roy SK, Prabhakar B. Bioadhesive polymeric platforms for transmucosal drug delivery systems—a review. Trop J Pharm Res. 2010;9(1):91-104. doi:10.4314/tjpr.v9i1.52043.
Bhalodia R, Basu B, Mehta K. Bucoadhesive drug delivery system: a review. Int J Pharm Bio Sci. 2010;1(1):1-32.
Ahuja A, Khar RK, Ali J. Mucoadhesive drug delivery systems. Drug Dev Ind Pharm. 1997;23(5):489-515.
Parthasarathy G, Bhaskar K, Jayaveera KN, Prasanth V. Buccal mucosa: a gifted choice for systemic drug delivery. Int J Drug Deliv. 2011;3:586-596.
Tiwari D, Goldman D, Sause R, Madan PL. Evaluation of polyoxyethylene homopolymers for buccal bioadhesive drug delivery device formulations. AAPS PharmSci. 1999;1(3):50-57.
Duchene D, Touchard F, Peppas NA. Pharmaceutical and medical aspects of bioadhesive systems for drug administration. Drug Dev Ind Pharm. 1988;14:283-318.
Gu JM, Robinson JR, Leung SH. Binding of acrylic polymers to mucin/epithelial surfaces: structure–property relationships. Crit Rev Ther Drug Carrier Syst. 1998;5:21-67.
Jimenez-Castellanos MR, Zia H, Rhodes CT. Mucoadhesive drug delivery systems. Drug Dev Ind Pharm. 1993;19:143-194.
Sigurdsson H, Loftsson T, Lehr C. Assessment of mucoadhesion by a resonant mirror biosensor. Int J Pharm. 2006;325(1-2):75-81.
Park K, Robinson JR. Mechanisms of mucoadhesion of poly(acrylic acid) hydrogels. Pharm Res. 1987;4(6):457-464.
Peppas NA, Little MD, Huang Y. Bioadhesive controlled release systems. In: Wise DL, editor. Handbook of pharmaceutical controlled release technology. New York: Marcel Dekker; 2000. p.255-269.
Park H, Amiji M, Park K. Mucoadhesive hydrogels effective at neutral pH. Proc Int Symp Control Release Bioact Mater. 1989;16:217-218.
van Wachem PB, Beugeling T, Feijen J, Bantjes A, Detmers JP, van Aken WG. Interaction of cultured human endothelial cells with polymeric surfaces of different wettabilities. Biomaterials. 1985;6(6):403-408.
Salamat-Miller N, Chittchang M, Johnston TP. The use of mucoadhesive polymers in buccal drug delivery. Adv Drug Deliv Rev. 2005;57(11):1666-1691.
Kamath KR, Park K. Mucosal adhesive preparations. In: Swarbrick J, Boylan JC, editors. Encyclopedia of pharmaceutical technology. New York: Marcel Dekker; 1994. p.133-138.
Shijith KV, Chandran CS. A review on basics behind development of mucoadhesive buccal drug delivery systems. Int J Adv Pharm Bio Chem. 2013;2:310-317.
Lehr CM, Poelma FCG, Junginger HE, Tukker JJ. An estimate of turnover time of intestinal mucus gel layer in the rats, in situ loop. Int J Pharm. 1991;70(1):235-240.
Sharma M. Mucoadhesive polymers for buccal drug delivery system. Asian J Pharm Res Dev. 2021;9(3):1-10.
Shaikh R, Raj Singh TR, Garland MJ, Woolfson AD, Donnelly RF. Mucoadhesive drug delivery systems. J Control Release. 2011;154(2):2-10.
Ugwoke MI, Agu RU, Verbeke N, Kinget R. Nasal mucoadhesive drug delivery: background, applications, trends and future perspectives. Adv Drug Deliv Rev. 2005;57(11):1640-1665.
Dubey R, Bajpai M, Mishra D. Recent advancements in mucoadhesive floating drug delivery systems: a mini-review. Eur J Med Chem. 2016; 111:419-434.
Jug M, Becirevic-Lacan M. Influence of hydroxypropyl-β-cyclodextrin complexation on piroxicam release from buccoadhesive tablets. Eur J Pharm Sci. 2004;21:251-260.
Gupta A, Garg S, Khar RK. Measurement of bioadhesive strengths of mucoadhesive buccal tablets: design of in-vitro assembly. Indian Drugs. 1992;30(4):152-155.
Ivarsson M, Wahlgren M. Comparison of in vitro methods of measuring mucoadhesion: ellipsometry, tensile strength, and rheological measurements. Colloids Surf B Biointerfaces. 2012;92:353-359.
Komati S, Rani S, Reddy M, et al. Mucoadhesive multiparticulate drug delivery systems. J Pharm Pharmacol. 2019;71(6):842-854.
Park K. A new approach to study mucoadhesion: colloidal gold staining. Int J Pharm. 1989;53:209-217.
Hassan EE, Gallo JM. Simple rheological method for the in vitro assessment of mucin-polymer bioadhesive bond strength. Pharm Res. 1990;7:491-498.
Batchelor H. Novel bioadhesive formulations in drug delivery. Drug Deliv Companies Rep. 2004 Autumn/Winter.
Bácskay I, Kósa D, Fenyvesi F, et al. Bioavailability enhancement and formulation strategies of oral mucosal drug delivery systems. Pharmaceutics. 2025;17(1):118.
Sharma D, Singh M, Kumar D, Singh G, Rathore MS. Formulation development and evaluation of fast disintegrating tablets of ambroxol hydrochloride for pediatrics—a novel approach for drug delivery. Indian J Pharm Educ Res. 2014;48(4):40-48. doi:10.5530/ijper.48.4s.6.
Dixit YD, Suruse PB, Shivhare UD. Formulation and evaluation of mucoadhesive buccal tablet of domperidone maleate. Indian J Pharm Educ Res. 2013;24(1):47-55.
Shivanand K, Raju SA, Nizamuddin S, Jayakar B. In vivo bioavailability studies of sumatriptan succinate buccal tablets. DARU J Pharm Sci. 2011;19(3):224-230.
Ghosalkar AR, Shettigar R, Phalak SD. Recent advances in buccal mucoadhesive drug delivery systems: development, applications, and challenges. Int J Novel Res Dev. 2025;10(1):1-11.
Reference
Senthil KM. Mucoadhesive buccal drug delivery system—an overview. Int J PharmTech Res. 2012;4:3951-3969.
Ahmed TA, Bawazir AO, Alharbi WS, Safo MK. Enhancement of simvastatin ex vivo permeation from mucoadhesive buccal films loaded with dual drug release carriers. Int J Nanomedicine. 2020;15:4001-4020. doi:10.2147/IJN.S256925.
Kumar K, Dhawan N, et al. Bioadhesive polymers: novel tool for drug delivery. Artif Cells Nanomed Biotechnol. 2014;42:274-283.
Shinkar DM, Dhake AS, Setty CM. Drug delivery from the oral cavity: a focus on mucoadhesive buccal drug delivery systems. PDA J Pharm Sci Technol. 2012;66(5):466-500. doi:10.5731/pdajpst.2012.00877.
Khanna R, Agarwal SP, Alka A. Mucoadhesive buccal drug delivery: a potential alternative to conventional therapy. Indian J Pharm Sci. 1998;60(1):1-11.
Miller NS, Chittchang M, Johnston TP. The use of mucoadhesive polymers in buccal drug delivery. Adv Drug Deliv Rev. 2005;57(11):1666-1691.
Vyas SP, Khar RK. Controlled drug delivery—concepts and advances. 1st ed. New Delhi: Vallabh Prakashan; 2002.
Smart JD. The basics and underlying mechanisms of mucoadhesion. Adv Drug Deliv Rev. 2005;57:1556-1568.
Kaul M. An overview of buccal drug delivery system. Int J Pharm Res. 2021;13(1):1303-1321. doi:10.31838/ijpr/2021.13.01.556.
Gandhi PA. A review article on mucoadhesive buccal delivery system. Int J Pharm Res Dev. 2011;3(0974):159-173.
Boddupalli BM, Mohammed ZNK, Nath AR, Banji D. Mucoadhesive drug delivery system: an overview. J Adv Pharm Technol Res. 2010;1(4):381-387. doi:10.4103/0110-5558.76436.
Longer MA, Robinson JR. Fundamental aspects of bioadhesion. Pharm Int. 1986;7:114-117.
Dodou P, Breedveld P, Wieringa PA. Mucoadhesives in the gastrointestinal tract: revisiting the literature for novel applications. Eur J Pharm Biopharm. 2005;60(1):1-16.
Derjaguin BV, Smilga VP. The electronic theory of adhesion. In: Adhesion: fundamentals and practice. Nottingham, UK & New York: University of Nottingham and Gordon & Breach; 1996.
Bhowmik D, Niladry C. Mucoadhesive buccal drug delivery system—an overview. J Adv Pharm Educ Res. 2013;3:319-331.
Ramesh B, Saravanakumar K, Nagaveni P, Mohan Kumar A, Jaya Preethi P, Vivek Kumar P. A review on buccal drug delivery system. Int J Res Pharm Sci. 2014;5(3):200-204. doi:10.5958/0975-4377.2017.00019.2.
Varma N, Chattopadhyay P. Polymeric platform for mucoadhesive buccal drug delivery system: a review. Int J Curr Pharm Res. 2011.
Bruschi ML, Jones DS, Panzeri H, Gremião MPD, Freitas O, Lara EH. Semisolid systems containing propolis for the treatment of periodontal disease: in vitro release kinetics, syringeability, rheological, textural, and mucoadhesive properties. J Pharm Sci. 2007;96(8):2074-2089.
Hägerström H, Edsman K, Strømme M. Low-frequency dielectric spectroscopy as a tool for studying compatibility between pharmaceutical gels and mucus tissue. J Pharm Sci. 2003;92:1869-1881.
Steward A. The effect of enhancers on buccal absorption of hybrid alpha interferon. Int J Pharm. 1994;104:145-149.
Patil KH, Mobin SA. Advances in mucoadhesive drug delivery system: enhancing effectiveness of typical and biomolecule drugs. J Drug Deliv Ther. 2024;14(10):105227.
Yajaman S, Bandyopadhyay AK. Buccal bioadhesive drug delivery—a promising option for orally less efficient drugs. J Control Release. 2006;114:15-40.
Edgar WM. Saliva: its secretion, composition and functions. Br Dent J. 1992;172:305-312.
Mahajan P, Kaur A, Aggarwal G, Harikumar SL. Mucoadhesive drug delivery system: a review. Int J Drug Dev Res. 2013;5(1):11-20. doi:10.20959/wjpps20174-8863.
Roy SK, Prabhakar B. Bioadhesive polymeric platforms for transmucosal drug delivery systems—a review. Trop J Pharm Res. 2010;9(1):91-104. doi:10.4314/tjpr.v9i1.52043.
Bhalodia R, Basu B, Mehta K. Bucoadhesive drug delivery system: a review. Int J Pharm Bio Sci. 2010;1(1):1-32.
Ahuja A, Khar RK, Ali J. Mucoadhesive drug delivery systems. Drug Dev Ind Pharm. 1997;23(5):489-515.
Parthasarathy G, Bhaskar K, Jayaveera KN, Prasanth V. Buccal mucosa: a gifted choice for systemic drug delivery. Int J Drug Deliv. 2011;3:586-596.
Tiwari D, Goldman D, Sause R, Madan PL. Evaluation of polyoxyethylene homopolymers for buccal bioadhesive drug delivery device formulations. AAPS PharmSci. 1999;1(3):50-57.
Duchene D, Touchard F, Peppas NA. Pharmaceutical and medical aspects of bioadhesive systems for drug administration. Drug Dev Ind Pharm. 1988;14:283-318.
Gu JM, Robinson JR, Leung SH. Binding of acrylic polymers to mucin/epithelial surfaces: structure–property relationships. Crit Rev Ther Drug Carrier Syst. 1998;5:21-67.
Jimenez-Castellanos MR, Zia H, Rhodes CT. Mucoadhesive drug delivery systems. Drug Dev Ind Pharm. 1993;19:143-194.
Sigurdsson H, Loftsson T, Lehr C. Assessment of mucoadhesion by a resonant mirror biosensor. Int J Pharm. 2006;325(1-2):75-81.
Park K, Robinson JR. Mechanisms of mucoadhesion of poly(acrylic acid) hydrogels. Pharm Res. 1987;4(6):457-464.
Peppas NA, Little MD, Huang Y. Bioadhesive controlled release systems. In: Wise DL, editor. Handbook of pharmaceutical controlled release technology. New York: Marcel Dekker; 2000. p.255-269.
Park H, Amiji M, Park K. Mucoadhesive hydrogels effective at neutral pH. Proc Int Symp Control Release Bioact Mater. 1989;16:217-218.
van Wachem PB, Beugeling T, Feijen J, Bantjes A, Detmers JP, van Aken WG. Interaction of cultured human endothelial cells with polymeric surfaces of different wettabilities. Biomaterials. 1985;6(6):403-408.
Salamat-Miller N, Chittchang M, Johnston TP. The use of mucoadhesive polymers in buccal drug delivery. Adv Drug Deliv Rev. 2005;57(11):1666-1691.
Kamath KR, Park K. Mucosal adhesive preparations. In: Swarbrick J, Boylan JC, editors. Encyclopedia of pharmaceutical technology. New York: Marcel Dekker; 1994. p.133-138.
Shijith KV, Chandran CS. A review on basics behind development of mucoadhesive buccal drug delivery systems. Int J Adv Pharm Bio Chem. 2013;2:310-317.
Lehr CM, Poelma FCG, Junginger HE, Tukker JJ. An estimate of turnover time of intestinal mucus gel layer in the rats, in situ loop. Int J Pharm. 1991;70(1):235-240.
Sharma M. Mucoadhesive polymers for buccal drug delivery system. Asian J Pharm Res Dev. 2021;9(3):1-10.
Shaikh R, Raj Singh TR, Garland MJ, Woolfson AD, Donnelly RF. Mucoadhesive drug delivery systems. J Control Release. 2011;154(2):2-10.
Ugwoke MI, Agu RU, Verbeke N, Kinget R. Nasal mucoadhesive drug delivery: background, applications, trends and future perspectives. Adv Drug Deliv Rev. 2005;57(11):1640-1665.
Dubey R, Bajpai M, Mishra D. Recent advancements in mucoadhesive floating drug delivery systems: a mini-review. Eur J Med Chem. 2016; 111:419-434.
Jug M, Becirevic-Lacan M. Influence of hydroxypropyl-β-cyclodextrin complexation on piroxicam release from buccoadhesive tablets. Eur J Pharm Sci. 2004;21:251-260.
Gupta A, Garg S, Khar RK. Measurement of bioadhesive strengths of mucoadhesive buccal tablets: design of in-vitro assembly. Indian Drugs. 1992;30(4):152-155.
Ivarsson M, Wahlgren M. Comparison of in vitro methods of measuring mucoadhesion: ellipsometry, tensile strength, and rheological measurements. Colloids Surf B Biointerfaces. 2012;92:353-359.
Komati S, Rani S, Reddy M, et al. Mucoadhesive multiparticulate drug delivery systems. J Pharm Pharmacol. 2019;71(6):842-854.
Park K. A new approach to study mucoadhesion: colloidal gold staining. Int J Pharm. 1989;53:209-217.
Hassan EE, Gallo JM. Simple rheological method for the in vitro assessment of mucin-polymer bioadhesive bond strength. Pharm Res. 1990;7:491-498.
Batchelor H. Novel bioadhesive formulations in drug delivery. Drug Deliv Companies Rep. 2004 Autumn/Winter.
Bácskay I, Kósa D, Fenyvesi F, et al. Bioavailability enhancement and formulation strategies of oral mucosal drug delivery systems. Pharmaceutics. 2025;17(1):118.
Sharma D, Singh M, Kumar D, Singh G, Rathore MS. Formulation development and evaluation of fast disintegrating tablets of ambroxol hydrochloride for pediatrics—a novel approach for drug delivery. Indian J Pharm Educ Res. 2014;48(4):40-48. doi:10.5530/ijper.48.4s.6.
Dixit YD, Suruse PB, Shivhare UD. Formulation and evaluation of mucoadhesive buccal tablet of domperidone maleate. Indian J Pharm Educ Res. 2013;24(1):47-55.
Shivanand K, Raju SA, Nizamuddin S, Jayakar B. In vivo bioavailability studies of sumatriptan succinate buccal tablets. DARU J Pharm Sci. 2011;19(3):224-230.
Ghosalkar AR, Shettigar R, Phalak SD. Recent advances in buccal mucoadhesive drug delivery systems: development, applications, and challenges. Int J Novel Res Dev. 2025;10(1):1-11.
A. B. Udar
Corresponding author
Dr. Vitthalrao Vikhe Patil Foundation’s College of Pharmacy, Vadgaongupta (Vilad ghat), Post MIDC, Ahilyanagar.
Dr. Vitthalrao Vikhe Patil Foundation’s College of Pharmacy, Vadgaongupta (Vilad ghat), Post MIDC, Ahilyanagar.
Manoj Rahinj
Co-author
Dr. Vitthalrao Vikhe Patil Foundation’s College of Pharmacy, Vadgaongupta (Vilad ghat), Post MIDC, Ahilyanagar.
A. B. Udar*, Aman Prajapati, Manoj Rahinj, A Review on: Mucoadhesive Drug Delivery Systems, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1123-1140 https://doi.org/10.5281/zenodo.17552140









 10.5281/zenodo.17552140
10.5281/zenodo.17552140