Department of Pharmaceutics, Loknete Dr. J. D. Pawar College of Pharmacy, Manur, Kalwan-423501 (Nashik) Maharashtra.
Mucoadhesive buccal tablets are a novel and patient-friendly drug delivery technology that adheres to the buccal mucosa, prolongs extended residence duration, and regulates drug release. The principles, advantages, challenges, and most recent developments in the field of mucoadhesive buccal medication administration are highlighted in this study. It discusses the anatomy and physiology of the buccal cavity, mechanisms of mucoadhesion and various natural and synthetic polymers employed to enhance adhesion and drug permeation.
Over the past two decades, mucoadhesion research has experienced significant growth, driven by its potential to improve targeted and systemic drug delivery. Although oral administration is often preferred, it has drawbacks, including liver metabolism and enzyme degradation, which limit the oral delivery of peptide and protein-based medications.1 Transmucosal delivery of drug offers advantages over oral administration. Mucoadhesion uses bioadhesive polymers to target drugs to specific body regions for extended periods.2 Transmucosal drug delivery can occur through various mucosal linings, with oral mucosa being a convenient and preferred route.3 Buccal mucosa, lining the inner cheek, is utilized for both systemic and local medication delivery. The buccal route serves as suitable for oligonucleotides, proteins and conventional small molecules. Bioadhesive formulations increase drug concentration, improving bioavailability, and reducing dose requirements and side effects.4 Drugs with partition coefficients (40-20,000) and pKa values (2-10) are optimal for buccal delivery.5
Structure of the Oral Cavity: 7,8,9,10,11,12
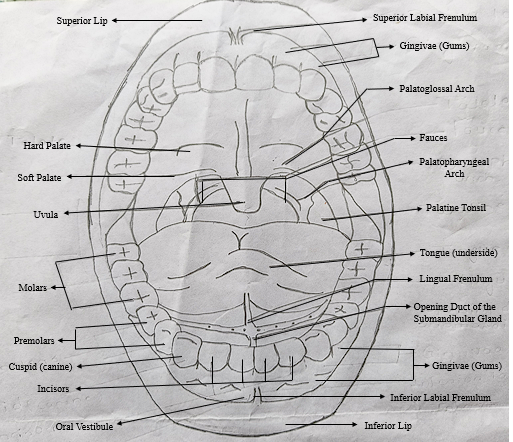
Fig. 1 Structure of the Oral Cavity 6
The Buccal Cavity: The buccal cavity is made up of the tonsils, floor of the oral cavity, both soft and hard palates, cheeks and the lips that enclose to the vestibule outside the mouth. A multilayered, highly vascularized mucous membrane that is rather thick and dense lines the oral cavity. Drugs are entering the systemic circulation through a network of capillaries and arties underneath the mucosal membrane. The phrase "buccal drug delivery" describes the release of a medication that can happen when the form of dosage is positioned within the external vestibule situated between the gingival and buccal mucosa, which is the membrane covering the cheeks.
Summary of Oral Mucosa: The buccal mucosa consists of dual layers: connective, basement membrane and epithelium tissue.
The Mucosal Layer: Mucus is a clear, thick, and sticky liquid that adheres to the mucosal epithelial surface and resembles a delicate, continuous gel coating. In humans, this layer's thickness varies between 50 and 450 µm. Goblet cells in the epithelial lining, or specialized exocrine glands, produce and secrete mucus. Although the exact nature of the mucus layer's composition differs significantly across species, locations, and health conditions, it generally consists of the following typical components:
|
Water |
95% |
|
Lipids and Glycoproteins |
0.5 to 5% |
|
Mineral salts |
0.5 to 1% |
|
Free Proteins |
0.5 to 1% |
Physiological factors influencing Buccal absorption
Table 1: Oral epithelium characteristics 13
|
Tissue |
Structure |
Epithelial Thickness (µm) |
Permeability |
Residence Time |
Blood (ml/min/cm2) |
|
Buccal |
Non keratinized |
500-600 |
Intermediate |
Intermediate |
2.4 |
|
Sublingual |
Non keratinized |
100-200 |
Very good |
Poor |
0.97 |
|
Gingival |
Keratinized |
200 |
Poor |
Intermediate |
1.47 |
|
Palatal |
Keratinized |
250 |
Poor |
Very good |
0.89 |
Introduction to the Oral Mucosal Tissue 14,15,16

Fig.2: Anatomy of Buccal Mucosa
A stratified squamous epithelial layer forms the outer surface of the oral mucosa, coated by mucous, which provides mechanical protection to underlying tissues. Beneath this layer lies the lamina propria and submucosa. The oral mucosa has varying degrees of keratinization, with non-keratinized regions (e.g., buccal mucosa) being more permeable than keratinized areas (e.g., gingiva and hard palate). The oral mucosa's structure and composition enable it to serve as a primary site for absorption of the drug in the oral cavity.
Mucoadhesion
"Fixing" of surfaces that are attached to one another is the simplest definition of adhesion.17 In a biological context, bioadhesion is the adherence of an organic or synthetic polymers to a biological substrate; if this adhesion takes place on mucosal membranes or a mucus layer, it is referred to as mucoadhesion. Mucoadhesive drug delivery systems take advantage of the sticky properties of specific polymers to target specific areas of the body, enhancing drug delivery and prolonging release. While oral administration is common, some medications are susceptible to acidic stomach conditions and first-pass metabolism, reducing bioavailability. To overcome these limitations, mucoadhesive systems are being developed for non-oral routes, such as buccal, nasal, and vaginal delivery. Research is ongoing, and mucoadhesive systems are being used to develop various medications, including those for hypertension, angina, inflammation, pain, ophthalmic conditions, and hormonal therapies.18
Mechanism of Mucoadhesion
The exact mechanism of bioadhesion between macromolecules and mucosal tissue remains unclear. For effective mucoadhesion, The adhesive should be capable of spreading across the entire surface area, facilitating intimate contact and promoting chain diffusion within the mucus. This process involves a balance of attractive and repulsive forces, with the attractive forces needing to dominate for successful mucoadhesion.19 Hence, the mucoadhesion mechanism is separated into two stages: contact and consolidation (Fig. 3).
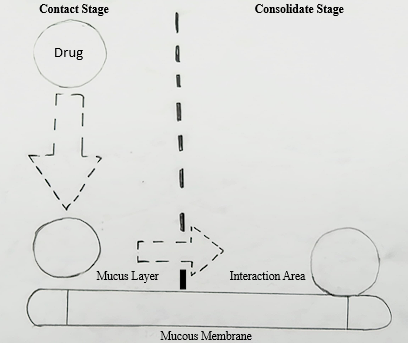
Fig.3: Phases of the Mucoadhesion Mechanism 20
Stage 1: The initial stage of mucoadhesion begins with contact between the mucoadhesive and the mucous membrane, followed by spreading and expansion to form a close bond with the mucus layer. The contact is mechanically facilitated in vaginal or ocular formulations, while nasal delivery relies on aerodynamic forces for deposition. In the gastrointestinal tract, direct adhesion is challenging, but peristaltic motion and oesophageal adhesion can aid in establishing contact.21
Stage 2: The consolidation stage is the second condition, where mucoadhesive molecules are activated by moisture, allowing them to relax and form bonds through weakened hydrogen and van der Waals interactions. There are two ideas that explain this phase: dehydration theory and diffusion theory. Diffusion theories implies mucoadhesive compounds and mucus glycoproteins engage by entangling their chains as well as forming supplementary bonds, creating a mixture that prolongs time of contact with the mucousal membrane. In contrast, theory of dehydration is less relevant for formulations that are solid or extremely hydrated.22
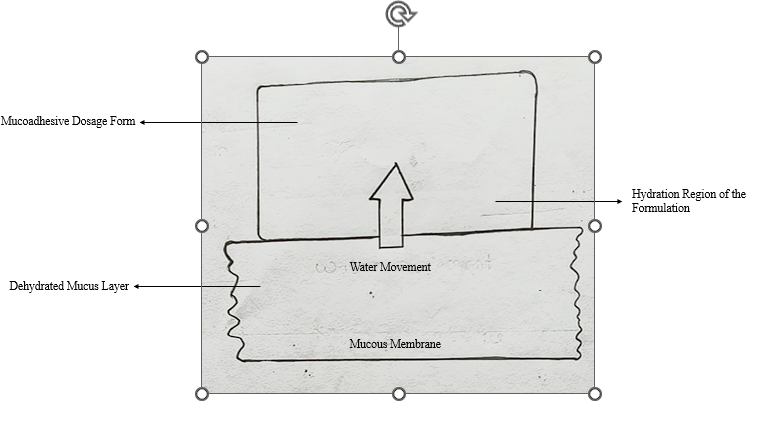
Fig. 4: Theory of Mucoadhesion for Dehydration 23
Theories of Mucoadhesion: 24,25,26
SAB = γB- γA - γAB
The adhesion work (WA), which represents the energy needed to separate two phases, increases as the interfacial energy exceeds the individual surface energies.
WA = γA + γB - γAB
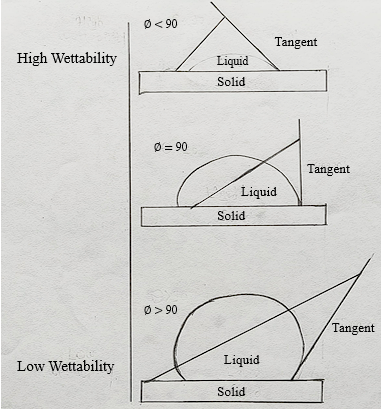
Fig.5: Schematic Representation showing effect of contact angle on Bioadhesion. 27
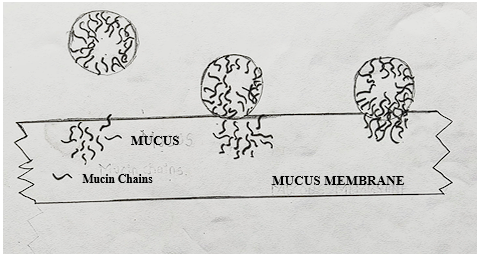
Fig.6: Secondary interactions resulting from inter-diffusion of polymer chains of bioadhesive device and of mucus. 28
Fracture theory: This widely accepted explanation, supported by mechanical measurements, describes the relationship between the forces required to detach polymers from mucus and the resilience of their adhesive bonds. Research shows that a decrease in cross-linking degree or an increase in network strand length results in a higher work of fracture, indicating stronger mucoadhesion.
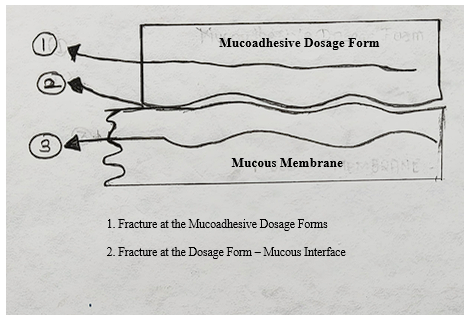
Fig.7: Possible sites of Mucoadhesive bond failure 29
Buccal drug delivery system: 30
Drug delivery through buccal cavity membranes may be categorized as follows:
1. Buccal Drug Delivery
Delivery by the buccal mucosa (inner lining of the cheek)
2. Sublingual Drug Delivery
Delivery through the mucous membrane under the tongue.
3. Transmucosal Drug Delivery
Delivery through other mucous membranes in the mouth, such as the gums or palate.
Advantages of Oral Cavity Drug Delivery: 31
Limitations of Buccal Drug Delivery: 32
CONCLUSION
Buccal Mucoadhesive drug delivery is a promising research arena, offering a gentle route for the systemic delivery of poorly absorbed oral drug and potent peptide/protein molecules. Advancing buccal drug delivery requires the development of safe and effective permeation enhancers. To optimize treatment outcomes, predicting, monitoring, and controlling delivery rates, biodegradation, and site-specific targeting are essential. The buccal mucosa provides a viable alternative route for delivering drugs vulnerable to gastric pH, intestinal enzymes, or hepatic first-pass effect. As new pharmaceuticals emerge, mucoadhesive systems will likely play a crucial role in innovative drug delivery solutions.
REFERENCES


Lalit Gangurde*, Dr. Rajendra Surawase, Rakesh Wagh, Akshay Aher, Darshan Khairnar, A Review on Mucoadhesive Buccal Tablets, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 4050-4059. https://doi.org/10.5281/zenodo.16601840
 10.5281/zenodo.16601840
10.5281/zenodo.16601840
