Mangaldeep Institute of Pharmacy, DBATU University Maharashtra
Pancreatic ductal adenocarcinoma (PDAC) stands as one of the most lethal forms of cancer, characterized by a dismal prognosis and a marked resistance to conventional chemotherapeutic interventions, particularly gemcitabine. Despite advances in targeted therapies and immune modulation, the survival rate for PDAC remains under 10% due to late-stage diagnosis, dense desmoplastic stroma, and immunosuppressive tumor microenvironment. Recent insights into the role of microorganisms, both endogenous and engineered—have opened new avenues in understanding and potentially reversing chemoresistance. Microbes, including certain classes of intratumoral bacteria such as Gammaproteobacteria, have been shown to enzymatically degrade chemotherapeutic drugs, reducing their efficacy. Conversely, the exploitation of these microbial communities offers novel therapeutic approaches: genetically modified bacteria and oncolytic viruses are capable of selectively targeting tumors, modulating immune responses, and enhancing drug bioavailability. Furthermore, strategies such as fecal microbiota transplantation (FMT), probiotic therapy, and microbial metabolite supplementation are being explored to improve patient responses and restore immune competence. This review explores the complex and dualistic relationship between the microbiome and PDAC, detailing the mechanisms of microbial-mediated chemoresistance, the therapeutic potential of microbial engineering, and the challenges inherent in clinical translation. Through a synthesis of recent literature and clinical studies, we propose a future in which microbiome-targeted therapies play a pivotal role in combating pancreatic cancer and improving patient outcomes.
Pancreatic ductal adenocarcinoma (PDAC) is among the most aggressive and lethal malignancies, ranking as the seventh leading cause of cancer-related deaths globally. Despite medical advances, PDAC remains a clinical challenge due to its asymptomatic early stages, late diagnosis, and rapid disease progression. With a five-year survival rate of less than 10%, the prognosis for patients remains bleak, especially in low- and middle-income countries where healthcare access is limited [1]. The mainstay chemotherapeutic agent for PDAC is gemcitabine, a nucleoside analog that inhibits DNA synthesis. However, clinical resistance to gemcitabine is nearly universal, with most patients experiencing relapse and poor overall survival even after initially responding to treatment [2]. Multiple factors contribute to this resistance, including tumor-intrinsic mechanisms (such as altered drug transporters and enhanced DNA repair), and tumor-extrinsic mechanisms, notably the tumor microenvironment (TME)—which includes dense stroma, hypoxia, poor vascularization, and immune suppression [3].
In recent years, a new dimension has been added to our understanding of PDAC pathophysiology: the tumor-associated microbiome. Traditionally regarded as opportunistic or contaminant flora, microbes residing within tumors are now recognized for their active role in modulating cancer biology. Landmark studies have identified bacterial DNA signatures and even viable bacteria within pancreatic tumors, indicating a possible biological interaction between host, tumor, and microbes [4,5]. One of the most striking discoveries came from Geller et al. (2017), who found that Gammaproteobacteria—a class of bacteria present within PDAC tissues—can express cytidine deaminase long isoform (CDDL), an enzyme capable of inactivating gemcitabine, thereby rendering the drug ineffective [6]. This represents a direct microbial mechanism of chemoresistance and has spurred interest in characterizing the microbial signatures within tumors as potential predictors of treatment response. Beyond drug metabolism, microbes shape cancer outcomes through immune modulation. Tumor-resident and gut-derived bacteria can stimulate regulatory T-cells, suppress cytotoxic T-cell responses, and activate chronic inflammatory pathways such as NF-κB and STAT3, all of which contribute to cancer progression and reduced chemotherapy sensitivity [7].
However, this microbial influence is not entirely detrimental. The same bacteria and viruses that contribute to resistance may also be repurposed as therapeutic agents. Genetically engineered bacteria (e.g., Salmonella typhimurium, Clostridium novyi-NT) and oncolytic viruses (e.g., herpes simplex virus, reovirus) have shown promise as targeted drug delivery systems and immune stimulants [8,9]. These microbes are designed to colonize hypoxic tumor regions, release immunostimulatory cytokines, or express enzymes that convert prodrugs into active cytotoxic compounds. Such strategies offer specificity, immune activation, and minimal systemic toxicity.

Figure 1: Dual role of microorganisms in pancreatic cancer chemotherapy—enhancing or hindering treatment by altering drug sensitivity, immune response, tumor progression, and resistance. Treatment outcomes by modulating drug sensitivity, immune responses, tumor progression, and chemotherapy resistance.
The gut microbiome also plays an indirect yet crucial role. Dysbiosis—an imbalance in gut microbial composition—has been associated with increased inflammation, impaired drug metabolism, and systemic immune dysregulation. Conversely, probiotics, microbial metabolites (e.g., short-chain fatty acids), and fecal microbiota transplantation (FMT) are being explored for their potential to restore homeostasis, improve chemotherapy tolerance, and sensitize tumors to treatment [10,11]. The overarching goal of this review is to synthesize current knowledge regarding the dual role of microorganisms in pancreatic cancer: both as drivers of chemoresistance and as tools for innovative treatment strategies. We will explore:
Given the growing body of evidence, integrating microbiome science with oncology could unlock new paradigms in cancer therapy. With advances in synthetic biology, metagenomics, and immune engineering, microbial therapeutics are poised to become central to precision oncology approaches for pancreatic cancer.
2. Mechanisms of Chemoresistance in Pancreatic Cancer
Pancreatic ductal adenocarcinoma (PDAC) is well known for its resistance to conventional chemotherapies, particularly gemcitabine, which is the frontline chemotherapeutic agent. This resistance is driven by a complex combination of tumor-intrinsic adaptations and extrinsic features of the tumor microenvironment (TME). Understanding these mechanisms is essential for designing more effective therapeutic strategies.
2.1 Tumor Microenvironment (TME)
The TME in PDAC is uniquely desmoplastic, composed of abundant extracellular matrix (ECM), cancer-associated fibroblasts (CAFs), immune cells, and endothelial cells. This fibrotic stroma forms a physical barrier that impairs the penetration of chemotherapeutic agents [12]. Unlike other tumors, PDAC’s TME is highly hypovascular, meaning it has poor blood supply, leading to low oxygen tension (hypoxia) and poor drug distribution [13]. The dense matrix, enriched with collagen and hyaluronic acid, increases interstitial pressure within tumors, further limiting the uptake of drugs like gemcitabine [14]. Additionally, stromal cells and ECM components actively communicate with tumor cells, promoting growth and survival. CAFs secrete transforming growth factor-beta (TGF-β), hepatocyte growth factor (HGF), and interleukin-6 (IL-6), which enhance epithelial-to-mesenchymal transition (EMT), invasiveness, and resistance to apoptosis [15].
2.2 Molecular Mechanisms of Intrinsic Resistance
On a cellular level, PDAC exhibits numerous molecular strategies that render it insensitive to chemotherapy. One of the most critical mechanisms involves ATP-binding cassette (ABC) transporters, such as P-glycoprotein (ABCB1) and multidrug resistance-associated proteins (MRPs), which actively expel chemotherapeutic agents from the cytoplasm, lowering their intracellular concentrations [16]. Furthermore, PDAC cells are proficient in DNA repair. The upregulation of DNA repair genes, including BRCA1/2 and PARP, allows these cells to recover from DNA-damaging agents. Inhibitors of these pathways (e.g., PARP inhibitors) have shown promise but are limited by resistance mutations [17]. Anti-apoptotic proteins such as Bcl-2 and survivin are also frequently overexpressed in PDAC, preventing programmed cell death despite cytotoxic insult [18]. Genetically, PDAC is driven by mutations in key oncogenes and tumor suppressor genes. Over 90% of PDACs harbor KRAS mutations, which activate downstream pathways like PI3K/AKT and MAPK, promoting proliferation and survival [19]. Co-occurring mutations in TP53, CDKN2A, and SMAD4 further contribute to resistance by deregulating cell cycle checkpoints and apoptosis.
2.3 Cancer Stem Cells (CSCs)
CSCs are a subpopulation within tumors that possess the ability to self-renew and differentiate. In PDAC, CSCs are marked by surface markers such as CD44, CD24, ESA (EpCAM), and ALDH1. These cells are inherently resistant to chemotherapy due to multiple factors: reduced proliferation rate, enhanced drug efflux via ABC transporters, robust DNA repair, and high expression of detoxifying enzymes [20]. CSCs are believed to play a critical role in tumor recurrence and metastasis following initial treatment success. Their resistance to therapy underscores the importance of targeting this subpopulation in future therapeutic strategies.
2.4 Immune Suppression and Evasion
The immune landscape of PDAC is predominantly immunosuppressive. Unlike “hot” tumors such as melanoma or non-small cell lung cancer, PDAC exhibits minimal infiltration of cytotoxic T cells. Instead, it is infiltrated by regulatory T cells (Tregs), myeloid-derived suppressor cells (MDSCs), and M2-type tumor-associated macrophages (TAMs), all of which secrete immunosuppressive cytokines like IL-10 and TGF-β, further inhibiting anti-tumor immunity [21]. In addition, PDAC tumors often downregulate MHC class I molecules, impairing antigen presentation and making them less visible to cytotoxic T cells. They also overexpress immune checkpoint proteins such as PD-L1, leading to T-cell exhaustion. This immune evasion directly contributes to chemoresistance, as a robust immune response is often necessary to support the effects of cytotoxic drugs [22].
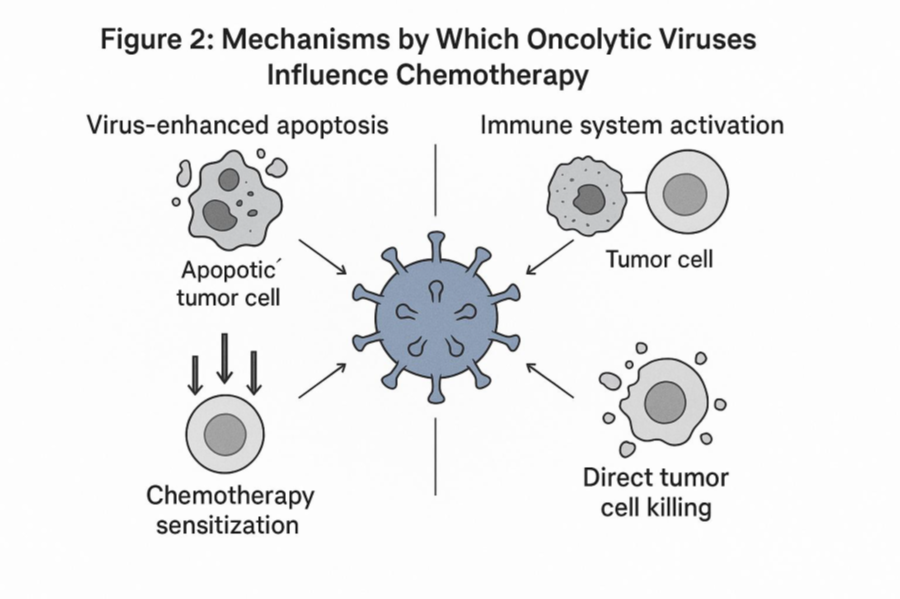
Figure 2: Mechanisms by Which Oncolytic Viruses Influence Chemotherapy
2.5 Clinical Relevance and Therapeutic Limitations
Clinically, these biological characteristics result in therapeutic failure. Gemcitabine monotherapy yields response rates of only 10–20%, and median survival remains less than six months in metastatic PDAC [23]. Combination regimens such as FOLFIRINOX or gemcitabine plus nab-paclitaxel have improved outcomes slightly, but at the cost of high toxicity, and resistance remains inevitable [24]. Notably, many current therapeutic agents fail to penetrate the dense stromal matrix, and tumor cells rapidly adapt by activating compensatory pathways. Attempts to target the stroma directly using hyaluronidase or Hedgehog pathway inhibitors have shown mixed results, as disrupting the stroma too extensively can lead to increased tumor aggression [25].
2.6 Implications for Microbial-Based Strategies
The TME’s structure and immunosuppressive tone make PDAC a hostile environment for conventional therapies—but may be exploited by microbial therapies. For instance, anaerobic bacteria and oncolytic viruses can preferentially target hypoxic tumor cores, which are resistant to drugs but accessible to certain microbes. Moreover, microbial agents may modulate the immune landscape, turning an immunologically “cold” tumor into a “hot” one, thus synergizing with immune checkpoint inhibitors and chemotherapy. Understanding these mechanisms not only highlights why PDAC is so resistant to current treatments, but also provides the rationale for novel therapeutic approaches—especially those involving the tumor microbiome, which will be explored in the next section.
3. Microbial Influence on Chemoresistance
The interaction between the microbiome and cancer chemotherapy has become a compelling area of research, shedding light on how microbial communities influence drug efficacy and resistance. Chemoresistance—the ability of cancer cells to evade the cytotoxic effects of chemotherapy—is a major hurdle in effective cancer treatment, particularly in aggressive cancers like pancreatic ductal adenocarcinoma (PDAC). Increasing evidence demonstrates that microorganisms within the tumor microenvironment and gut microbiota significantly modulate chemoresistance via multiple biological mechanisms [25].
3.1 Microbial Metabolism of Chemotherapeutic Agents
One of the most direct ways microbes influences chemoresistance is through enzymatic modification of chemotherapeutic drugs, altering their bioavailability and toxicity. Certain bacteria express enzymes capable of metabolizing or inactivating chemotherapeutic agents, effectively reducing their cytotoxic potential against tumor cells. For example, Gammaproteobacteria present in PDAC tumors can express cytidine deaminase, which metabolizes gemcitabine—a frontline chemotherapeutic agent—into its inactive form, leading to decreased drug efficacy and resistance [26]. This bacterial enzymatic inactivation not only limits drug action locally but may also alter systemic drug metabolism when gut microbiota is involved [27].
3.2 Modulation of the Tumor Microenvironment
Microbes within the tumor microenvironment can influence chemoresistance by altering immune responses and stromal components. Tumor-associated microbiota can promote an immunosuppressive microenvironment by inducing regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), which dampen antitumor immunity and promote tumor survival despite chemotherapy [28]. Additionally, bacterial products such as lipopolysaccharides (LPS) and peptidoglycans trigger chronic inflammation via toll-like receptor (TLR) signaling pathways, leading to increased secretion of pro-survival cytokines like IL-6 and TNF-α. This inflammatory milieu enhances cancer cell resistance to apoptosis induced by chemotherapy [29]. Furthermore, microbial modulation of stromal cells like cancer-associated fibroblasts (CAFs) promotes extracellular matrix remodeling and desmoplasia, limiting drug penetration and fostering chemoresistance [30]. The dense fibrotic stroma in pancreatic tumors acts as a physical barrier that prevents adequate drug delivery, a process influenced by microbial-driven inflammation.
3.3 Microbial Influence on Cancer Cell Signaling Pathways
Microbes can affect key cellular signaling pathways involved in chemoresistance. For instance, bacterial components activate signaling cascades such as NF-κB, STAT3, and MAPK pathways in tumor cells, enhancing the expression of drug efflux pumps like P-glycoprotein and anti-apoptotic proteins (Bcl-2 family), which protect cancer cells from chemotherapeutic damage [31]. The activation of these pathways results in decreased intracellular accumulation of drugs and inhibition of apoptosis, both of which are hallmarks of chemoresistant phenotypes. Moreover, microbial metabolites such as short-chain fatty acids (SCFAs) and secondary bile acids can epigenetically regulate gene expression in cancer cells, further influencing resistance mechanisms [32]. For example, butyrate, an SCFA, can modulate histone acetylation affecting genes involved in cell cycle regulation and drug response.
3.4 Microbial-Induced Epithelial-Mesenchymal Transition (EMT)
The process of epithelial-mesenchymal transition (EMT) is a key driver of chemoresistance, promoting cancer cell plasticity, invasiveness, and survival under stress. Microbial infections and their secreted factors can induce EMT in cancer cells, enhancing resistance to chemotherapy [33]. Studies have shown that bacterial toxins and inflammatory mediators activate EMT-related transcription factors such as Snail, Twist, and Zeb1, which downregulate epithelial markers (e.g., E-cadherin) and upregulate mesenchymal markers (e.g., vimentin) [34]. This phenotypic switch not only supports metastasis but also confers resistance to drugs by increasing cellular efflux mechanisms and DNA repair capacity.
3.5 Microbiome and Immune Checkpoints Modulation
Emerging research highlights the role of the microbiome in modulating immune checkpoint pathways that contribute to chemoresistance. Certain bacterial taxa promote the expression of immune checkpoint molecules like PD-L1 on tumor and immune cells, thereby attenuating cytotoxic T cell activity during chemotherapy [35]. This immune evasion mechanism supports tumor cell survival despite chemotherapy-induced stress. Additionally, the microbiota can influence the efficacy of combined chemo-immunotherapy approaches by shaping host immune responses [36].
3.6 Gut Microbiota and Systemic Chemoresistance
The gut microbiota plays a crucial role in systemic modulation of chemoresistance by influencing drug pharmacokinetics, host metabolism, and immune function. Dysbiosis—an imbalance in microbial composition—can alter the metabolism of chemotherapeutic drugs, reduce drug absorption, and modulate systemic inflammation that affects tumor response [37]. For example, some gut bacteria activate hepatic enzymes that metabolize chemotherapy agents, altering drug plasma levels and therapeutic outcomes [38]. Moreover, microbial metabolites produced in the gut can reach the tumor site through circulation, impacting local tumor biology and chemoresistance pathways. The gut microbiota also educates systemic immune responses, which are critical in determining the success of chemotherapy [39].
4. Strategies to Overcome Microbial-Induced Chemoresistance
Given the significant role of the microbiome in mediating chemoresistance, innovative therapeutic strategies targeting microbial components represent a promising avenue to improve chemotherapy efficacy, especially in pancreatic cancer. This section explores current and emerging strategies designed to overcome microbial-induced chemoresistance, highlighting their mechanisms, challenges, and potential clinical applications.
4.1 Antibiotics and Targeted Microbial Depletion
One of the most direct approaches to counter microbial-induced chemoresistance is the use of antibiotics to selectively deplete bacterial populations that inactivate chemotherapeutic drugs or promote tumor survival. For instance, studies have demonstrated that treating pancreatic cancer models with antibiotics that target Gammaproteobacteria—bacteria known to metabolize gemcitabine into its inactive form—restores drug sensitivity and reduces tumor growth [41]. Similarly, antibiotic administration can reduce the tumor-associated bacterial load, diminishing immunosuppressive signaling and inflammation that contribute to chemoresistance [42]. However, the use of broad-spectrum antibiotics may also disrupt beneficial microbiota and impair immune responses, leading to unintended side effects and potentially reducing overall treatment efficacy [43]. Therefore, research is focusing on developing narrow-spectrum or targeted antimicrobial agents that selectively eradicate detrimental microbes without compromising the overall microbiome diversity [44].
4.2 Probiotics and Prebiotics to Restore Healthy Microbiota Balance
Restoring or maintaining a healthy microbiome balance through the use of probiotics (live beneficial bacteria) and prebiotics (non-digestible food components that promote beneficial bacteria growth) is another promising strategy to combat chemoresistance. Probiotics have been shown to modulate immune responses, reduce inflammation, and enhance epithelial barrier function, potentially improving chemotherapy outcomes [45]. For example, Lactobacillus and Bifidobacterium species have demonstrated protective roles by enhancing antitumor immunity and reducing treatment-related toxicity [46]. Prebiotics, such as dietary fibers, can selectively stimulate the growth of beneficial microbes that produce anti-inflammatory metabolites like short-chain fatty acids (SCFAs), which can sensitize tumor cells to chemotherapy [47]. Combining probiotics and prebiotics (synbiotics) could synergistically optimize the microbiome environment to overcome resistance [48]. Nonetheless, further clinical studies are needed to define optimal strains, doses, and treatment regimens for effective microbiome modulation in cancer patients [49].
4.3 Microbiome Engineering and Phage Therapy
Advancements in synthetic biology and microbiome research have paved the way for microbiome engineering approaches to overcome chemoresistance. These techniques involve genetically modifying bacteria to enhance their antitumor activity or reduce their ability to induce drug resistance. Engineered bacteria can be designed to deliver therapeutic molecules directly into the tumor microenvironment or to degrade chemoresistance-promoting factors [50]. Phage therapy—the use of bacteriophages to selectively target and kill specific bacterial species—is gaining traction as a precise method to eliminate drug-inactivating or immunosuppressive bacteria within tumors [51]. Phages can penetrate dense tumor matrices and specifically target problematic bacteria without disturbing beneficial microbes, overcoming a major limitation of traditional antibiotics [52]. Early studies indicate that phage therapy combined with chemotherapy could synergistically improve treatment outcomes by reversing microbial-mediated resistance [53].
4.4 Combining Chemotherapy with Microbiome-Modulating Agents
An integrative therapeutic approach involves combining standard chemotherapy with agents that modulate the microbiome or its effects. This can include immunomodulators, anti-inflammatory drugs, or microbial metabolites that enhance drug sensitivity. For example, the use of TLR agonists or antagonists can reprogram tumor-associated immune cells, reversing the immunosuppressive microenvironment fostered by bacteria [54]. Additionally, fecal microbiota transplantation (FMT) from healthy donors or responders has shown promise in restoring microbiome diversity and improving chemotherapy responsiveness in preclinical models [55]. By shifting the microbial composition towards a more favorable state, these combined therapies may enhance drug efficacy and reduce resistance. Such combination therapies require careful consideration of timing, dosing, and patient-specific microbiome profiles to maximize benefit and minimize adverse effects [56].
4.5 Personalized Microbiome Profiling to Guide Therapy
Given the heterogeneity of the microbiome across patients, personalized microbiome profiling has emerged as a crucial strategy to tailor interventions for overcoming chemoresistance. High-throughput sequencing and metagenomic analyses allow for detailed characterization of tumor-associated and gut microbiota, identifying microbial signatures associated with resistance or sensitivity to chemotherapy [57]. Using this information, clinicians can stratify patients likely to benefit from microbiome-targeted therapies, select appropriate antibiotics or probiotics, and monitor microbial shifts during treatment to adapt therapeutic regimens dynamically [58]. Personalized microbiome interventions have the potential to transform cancer care by improving precision and reducing unnecessary toxicity [59].
5. Clinical Implications and Future Perspectives
Understanding the role of microbes in chemoresistance opens new avenues for improving pancreatic cancer treatment, but translating these findings from bench to bedside presents significant challenges and opportunities. This section discusses the clinical applications, current trials, future directions, and ethical considerations involved in microbiome-targeted cancer therapies.
5.1 Current Clinical Trials Targeting Microbiota in Pancreatic Cancer
Several clinical trials are underway exploring microbiome modulation to improve chemotherapeutic efficacy in pancreatic cancer. These include trials using antibiotics to reduce drug-inactivating bacteria, probiotics to restore microbiome balance, and fecal microbiota transplantation (FMT) to enhance immune responses [61]. For example, a phase II clinical trial is investigating the combination of gemcitabine with antibiotic therapy targeting Gammaproteobacteria to overcome gemcitabine resistance [62]. Additionally, trials combining immunotherapy with microbiome modulators are ongoing, aiming to leverage microbial influence on immune checkpoint blockade efficacy [63]. These efforts highlight the clinical potential of microbiome-targeted interventions to enhance standard treatments but also underscore the need for robust biomarkers and patient stratification strategies.
5.2 Challenges in Implementing Microbiome-Based Therapies
Despite promising preclinical data, several challenges hinder the clinical implementation of microbiome-based therapies. First, the complex and dynamic nature of the microbiome makes it difficult to identify causative microbial species and predict patient responses [64]. Interindividual variability, influenced by genetics, diet, lifestyle, and environment, complicates standardized treatment protocols [65]. Moreover, the risk of off-target effects and unintended consequences of microbiome modulation, such as opportunistic infections or dysbiosis, requires careful monitoring [66]. Regulatory hurdles and the lack of standardized methods for microbiome analysis and manipulation further slow clinical translation [67]. Addressing these challenges necessitates multidisciplinary collaboration and technological advances.
5.3 Microbiome-Derived Biomarkers for Predicting Treatment Response
Microbiome profiling has the potential to identify biomarkers that predict chemotherapy response and guide personalized therapy. Specific microbial signatures have been associated with favorable or poor outcomes in cancer patients receiving chemotherapy or immunotherapy [68]. For instance, the presence of Akkermansia muciniphila and certain Bifidobacterium species correlates with better responses to immune checkpoint inhibitors [69]. Developing reliable, non-invasive microbiome-based biomarkers using stool, blood, or tumor samples could facilitate early identification of patients at risk of chemoresistance and enable timely intervention [70]. Integrating microbiome data with other omics (genomics, metabolomics) can further refine predictive models for personalized treatment strategies.
5.4 Future Research Directions: Integrative Multi-Omics and Personalized Medicine
Future research must adopt integrative multi-omics approaches combining microbiomics, genomics, transcriptomics, proteomics, and metabolomics to unravel the complex host-microbe interactions driving chemoresistance [71]. Such holistic analyses can identify novel therapeutic targets and mechanisms. Personalized medicine approaches leveraging detailed patient-specific microbiome data will enable tailored interventions to modulate the microbiome effectively and safely. Machine learning and artificial intelligence can assist in analyzing large datasets and predicting optimal treatment regimens based on microbial and host profiles [72]. Furthermore, longitudinal studies tracking microbiome changes during treatment will provide insights into temporal dynamics influencing therapy response and resistance development [73].
5.5 Ethical and Safety Considerations in Microbiome Manipulation
Manipulating the microbiome for cancer therapy raises important ethical and safety concerns. Risks include the potential transfer of antibiotic resistance genes, disruption of beneficial microbes, and unpredictable immune reactions [74]. Ensuring patient safety requires rigorous preclinical testing, informed consent, and post-treatment monitoring.
Ethical considerations also involve equitable access to emerging therapies and addressing disparities in microbiome research, which often underrepresents diverse populations [75]. Transparency in research and clinical applications is essential to build trust and responsibly integrate microbiome-based treatments into oncology care.
SUMMARY
Recent research has uncovered the profound impact of the microbiome on chemoresistance in pancreatic cancer, revealing that both tumor-associated and gut microbes can significantly influence treatment outcomes. Microbial species can enzymatically inactivate chemotherapeutic agents like gemcitabine, alter the tumor microenvironment to promote immunosuppression and inflammation, and modulate systemic metabolism, thereby reducing drug efficacy and contributing to therapeutic failure. This intricate host-microbe interplay highlights the microbiome as a critical factor in drug resistance, underscoring the need to integrate microbial considerations into cancer treatment strategies. Therapeutically, approaches such as targeted antibiotics, probiotics, phage therapy, and engineered microbial interventions show great promise in reversing or preventing chemoresistance. However, challenges including interpatient variability in microbiome composition, potential disruption of beneficial microbes, and associated safety concerns necessitate careful development and clinical validation of these interventions. Personalized microbiome modulation using narrow-spectrum agents and biomarker-driven treatment plans may mitigate these risks and optimize efficacy. Incorporating microbiome profiling into pancreatic cancer management is essential to advance precision medicine. Microbial signatures can serve as predictive biomarkers for chemotherapy response, enabling tailored therapeutic decisions and dynamic monitoring of treatment effectiveness. Collaborative efforts across oncology, microbiology, and bioinformatics are vital to translate these insights into practical clinical applications. Future directions involve leveraging multi-omics technologies and machine learning to develop personalized, microbiome-informed therapies. Longitudinal monitoring of microbial dynamics during treatment will allow adaptive strategies to counteract emerging resistance. Ethical, regulatory, and safety considerations must be prioritized to ensure responsible clinical translation. Overall, harnessing the microbiome’s influence offers a transformative opportunity to improve chemotherapy outcomes, reduce resistance, and enhance survival and quality of life for pancreatic cancer patients, marking a promising frontier in oncology research and patient care.
CONCLUSION
In conclusion, the growing body of evidence firmly establishes the microbiome as a pivotal player in pancreatic cancer chemoresistance, influencing treatment outcomes through diverse and complex mechanisms. Understanding the microbial contribution to drug inactivation, immune modulation, and tumor microenvironment alteration provides a new dimension to tackling one of the deadliest cancers. While promising therapeutic strategies targeting microbiomes such as selective antibiotics, probiotics, and phage therapies—are emerging, they must overcome significant challenges related to microbial diversity, safety, and patient-specific variability. Integrating microbiome analysis into clinical practice represents a crucial step toward precision oncology, enabling personalized treatment plans informed by microbial biomarkers that predict and monitor therapy response. The future of pancreatic cancer treatment lies in multi-disciplinary collaboration, leveraging cutting-edge technologies like multi-omics and artificial intelligence to design adaptive, individualized microbiome-based interventions. Equally important are the ethical and regulatory frameworks that will ensure patient safety and equitable access as these novel therapies advance from research to clinical application. Ultimately, harnessing the microbiome’s full therapeutic potential offers hope for overcoming chemoresistance, improving patient survival rates, and enhancing quality of life. This paradigm shift underscores the necessity of viewing pancreatic cancer through a holistic lens that embraces the dynamic interplay between host, tumor, and microbiota, setting the stage for more effective and durable cancer therapies in the future.
REFERENCES

Niranjan Giri, Quadri Mohammed Soheb, Nikita Bodkhe, Mayur Katode, A Review on Microbial Strategies to Combat Chemoresistance in Pancreatic Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2010-2024. https://doi.org/10.5281/zenodo.15633160
 10.5281/zenodo.15633160
10.5281/zenodo.15633160
