Department of Pharmacy, Georai Tanda, Paithan Road, Chh.Sambhajinagar
Leprosy is a neglected infectious disease caused by acid-fast bacillus Mycobacterium leprae. It primarily affects the skin and then progresses to a secondary stage, causing peripheral neuropathy with potential long-term disability along with stigma. Leprosy patients account for a significant proportion of the global disease burden. Previous efforts to improve diagnostic and therapeutic techniques have focused on leprosy in adults, whereas childhood leprosy has been relatively neglected. This review aims to update the diagnostic and therapeutic recommendations for adult and childhood leprosy. This review summarizes the clinical, bacteriological, and immunological approaches used in the diagnosis of leprosy. As strategies for the diagnosis and management of leprosy continue to develop better and more advanced knowledge, control and prevention of leprosy are crucial.
Leprosy, also known as Hansen’s disease, is a chronic slightly contagious disease. Leprosy is likely transmitted via droplets, from the nose and mouth, during close and frequent contact with untreated cases. It is caused by bacillus bacteria called Mycobacterium Leprae. It mainly affects the skin and peripheral nerves, mucosa of the upper respiratory tract and the eyes. Untreated, leprosy can cause progressive and permanent damage to the skin, nerves, limbs and eyes. Involvement of certain peripheral nerves may result in characteristic patterns of disabilities leading to ulceration of skin and deformity of some joints.
Leprosy is curable and treatment in the early stages can prevent disability. Deep-rooted stigmatization has prevented many patients from seeking treatment early, leading to visible deformities and disabilities.
In 2018, a total of 14 countries from the Eastern Mediterranean Region reported new indigenous leprosy cases to WHO with a total of 4356 new cases of leprosy detected, and the registered prevalence was 5.096 cases.
Multidrug therapy (MDT) treatment has been made available through WHO free of charge to all patients worldwide since 1995. MDT provides a highly effective cure for all types of leprosy. Elimination of leprosy as public health problem (defined as a registered prevalence of less than 1 case per 10 000 persons) was achieved globally in 2000. More than 16 million leprosy patients have been treated with MDT over the past 20 years.
In the neglected tropical diseases draft roadmap "Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030", leprosy is targeted for elimination (interruption of transmission) which is defined as zero indigenous new cases.(1)
Leprosy is a chronic infectious disease caused by the bacillus Mycobacterium leprae. While the organism is readily transmitted from person to person, it does not usually produce the clinical disease because of intrinsic human resistance to the infectious agent in the majority of people.
The disease affects mostly the skin and peripheral nerves. Its spectrum of manifestations varies from tuberculoid to lepromatous, depending on the cellular immune status of the patient.
Diagnosis is based on the clinical features, along with the lepromin test to determine the type of disease. Early detection, prompt and adequate treatment, and rehabilitation of any residual deformities, are all essential components of the management of leprosy and to ensure the patient is reintegrated into society fully.
The disfigurement and disability associated with this condition, with the absence of any effective treatment, are largely responsible for the fear and deep revulsion this condition has caused through most of human history. (13)
SYMPTOMS AND CAUSES
Symptoms of leprosy (Hansen’s disease)
Symptoms of leprosy include:
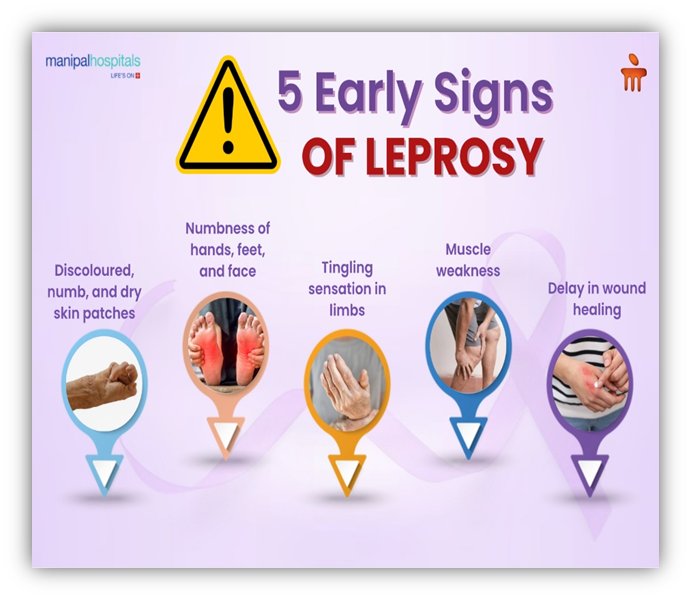
Fig- Early Signs of Leprosy
CAUSES LEPROSY
Leprosy is caused by a slow-growing type of bacteria called Mycobacterium leprae (M. leprae). Leprosy is also known as Hansen's disease, after the scientist who discovered M. leprae in 1873.
Is leprosy contagious?
It's not clear exactly how leprosy is transmitted. When a person with the disease coughs or sneezes, they may spread droplets containing the M. leprae bacteria that another person breathes in. It takes close physical contact with an infected person to transmit leprosy. It's not spread by casual contact like shaking hands, hugging, or sitting next to someone on a bus or at a table during a meal.
Pregnant mothers with leprosy can’t pass it to their babies. It’s not spread by sexual contact, either. (3)
Leprosy affects mainly the skin and peripheral nerves. Nerve involvement causes numbness and weakness in areas controlled by the affected nerves.
Symptoms of leprosy usually do not begin until > 1 year after infection (average 5 to 7 years). Once symptoms begin, they progress slowly.
TYPES OF LEPROSY
Skin lesions consist of one or a few hypaesthesic, centrally hypopigmented macules with sharp, raised borders. The rash, as in all forms of leprosy, is nonpruritic. Areas affected by this rash are numb because of damage to the underlying peripheral nerves, which may be palpably enlarged.
Much of the skin and many areas of the body, including the kidneys, nose, and testes, may be affected. Patients have skin macules, papules, nodules, or plaques, which are often symmetric. Peripheral neuropathy is more severe than in tuberculoid leprosy, with more areas of numbness; certain muscle groups may be weak. Patients may develop gynecomastia or lose eyelashes and eyebrows.
Features of both tuberculoid and lepromatous leprosy are present. Without treatment, borderline leprosy may become less severe and more like the tuberculoid form, or it may worsen and become more like the lepromatous form.
COMPLICATIONS OF LEPROSY
The most severe complications result from the peripheral neuropathy, which causes deterioration of the sense of touch and a corresponding inability to feel pain and temperature. Patients may unknowingly burn, cut, or otherwise harm themselves. Repeated damage may lead to loss of digits. Muscle weakness can result in deformities (e.g., clawing of the 4th and 5th fingers caused by ulnar nerve involvement, foot drop caused by peroneal nerve involvement) (5)
Other areas of the body may be affected:
Humans are the main natural reservoir for M. leprae. Armadillos are the only confirmed source other than humans, although other animal and environmental sources may exist.
Leprosy is thought to be spread by passage from person to person through nasal droplets and secretions. Casual contact (e.g., simply touching someone with the infection) and short-term contact does not seem to spread it. About half of people with leprosy probably contracted it through close, long-term contact with an infected person. Even after contact with the bacteria, most people do not develop leprosy; health care workers often work for many years with people who have leprosy without contracting it. Most immunocompetent people who are infected with M. leprae do not develop leprosy because of effective immunity. People who do develop leprosy probably have a poorly defined genetic predisposition.
M. leprae grow slowly (doubling in 2 weeks). The usual incubation period ranges from 6 months to 10 years. Once infection develops, hematogenous dissemination can occur.
Classification of leprosy
Leprosy is classified by type and number of skin areas affected:
Leprosy also is classified by cellular response and clinical findings:
People with tuberculoid leprosy typically have a strong cell-mediated response, which limits disease to a few skin lesions (paucibacillary), and the disease is milder, less common, and less contagious.
People with lepromatous or borderline leprosy typically have poor cell-mediated immunity to M. leprae and have more severe, systemic infection with widespread bacterial infiltration of skin, nerves, and other organs (e.g., nose, testes, kidneys). They have more skin lesions (multibacillary), and the disease is more contagious.
In both classifications, the type of leprosy dictates
LEPROSY EPIDEMIOLOGY
The highest rates of leprosy are in tropical countries, especially in Asia and Africa. Underdeveloped nations are at the greatest risk and, even today, 105 countries qualify as endemic for the disease. These countries are mostly in Southeast Asia, North and South America, Africa, and the eastern seaboard of the Pacific Ocean and the Western Mediterranean coast. India alone accounts for 64 percent of all new cases in the world.
The current prevalence of leprosy is approximately 0.34 per 10,000.
Over 200 000 new cases of leprosy have been reported annually in recent years. The primary source is lepromatous patients who are not being treated. The microbe persists in fomites and other sources outside the patient’s body when conditions are right however, most people in endemic areas have developed resistance to the mycobacterium.
The highest number of cases in the world is still found in India, with Brazil ranking second. The most useful indicators used in epidemiology include the new case detection rate, the new case rate in children below 15 years, and the number of cases with grade 2 or more disability.
Leprosy incidence in children under 15 years of age is one of the primary monitoring indices of endemicity because leprosy in this age group is a result of recent transmission from an active case, with high endemicity in that area. All these traits reveal a lack of adequate healthcare in the region affected. Contact tracing is important in detecting the source of infection.
Confounding factors which may interfere with the gathering of epidemiological data from developing nations include:
Factors which contribute to late diagnosis include lack of general information about the early signs and curability of leprosy, and lack of accessible and specific treatment for the disease.
Thus, the quality of health care can also be assessed by the extent of physical disability due to leprosy.
When a large number of cases of permanent serious disability are found in a region, it is important to consider the possibility of a reservoir of hidden leprosy, untapped by case detection or leprosy programs, and thus serving as a source of infection to the community.
Early detection, contact tracing, detection of cases from this population, and chemoprophylaxis or immune prophylaxis for healthy household contacts, with supervised MDT for proven cases, are essential parts of any program to eliminate or control leprosy in any endemic region. (13)

Fig- Leprosy Epidomology
CLINICAL FEATURES OF LEPROSY
Detecting the clinical features of leprosy in a patient requires a meticulous approach. The presentation is subtle in many patients, especially in the indeterminate and tuberculoid portions of the spectrum. The patient should be fully exposed and observed under adequate lighting to detect the clinical signs of leprosy.
According to the Eighth Report of the WHO Expert Committee on Leprosy, leprosy should be suspected in people with any of the following symptoms and signs
Leprosy is a disease with myriad different presentations, largely due to the broad immune response towards the M. leprae strain.
Ridley-Jopling classification system covers the entire depth of the clinical feature. From an intense immune response with a small number of tuberculoid organisms to a minor response with an elevated number of multibacillary cells. Overall, this classification is applied using a cutaneous, biopsy, and neurologic outcomes from the body. This gives medical professionals a reasonable estimate of the immune response to be produced. The previously mentioned findings are also related to the acid-fast bacilli that exist in the dermis.
This includes:
Clinical Types of Leprosy
Skin lesions that are commonly seen in leprosy can be categorized in the following subsections:
DIAGNOSIS OF LEPROSY
The guidelines recommend no additional tests in addition to standard methods for diagnosis of leprosy: the diagnosis of leprosy remains based on the presence of at least one of three cardinal signs: definite loss of sensation in a pale (hypopigmented) or reddish skin patch; thickened or enlarged peripheral nerve with loss of sensation and/or weakness of the muscles supplied by that nerve; or (iii) presence of acid-fast bacilli in a slit-skin smear.
The clinical diagnosis of early leprosy and PB leprosy can be a challenge. Therefore, a number of serological and other laboratory assays have been developed to supplement clinical diagnostic methods. However, enzyme-linked immunosorbent assays (ELISA) and lateral flow assays are associated with low diagnostic accuracy for PB leprosy.
Although some polymerase chain reaction (PCR)-based assays are associated with higher diagnostic accuracy, they lack standardization, are not commercially available, and would be difficult to perform in most primary health-care settings. The guidelines also do not recommend any test for the diagnosis of leprosy in asymptomatic contacts. The predictive accuracy of diagnostic tests for identifying persons who will develop leprosy is low, with poor positive predictive values.
TREATMENT OF LEPROSY
The guidelines recommend a 3-drug regimen of rifampicin, dapsone and clofazimine for all leprosy patients, with a duration of treatment of 6 months for PB leprosy and 12 months for MB leprosy. This represents a change from the current standard treatment for PB leprosy, which is rifampicin and dapsone for 6 months, due to some evidence indicating better clinical outcomes with a 3-drug, 6-month regimen over a 2-drug, 6-month regimen. A potential advantage of using the same three drugs for PB and MB leprosy is simplification of treatment (i.e. the same blister pack could be used for treating both types of leprosy) and reduced impact of misclassification of MB leprosy as PB leprosy, since all patients will receive a 3-drug regimen. For MB leprosy, the current standard treatment is a 3-drug regimen for 12 months.
Evidence on the potential benefits and harms of a shorter (6-month) 3-drug regimen was limited and inconclusive, with a potential increase in the risk of relapse. Therefore, the GDG determined that there was not enough evidence of equivalent outcomes to support a recommendation to shorten the treatment duration for MB leprosy. For rifampicin-resistant leprosy, the guidelines recommend treatment with at least two second-line drugs (clarithromycin, minocycline or a quinolone) plus clofazimine daily for 6 months, followed by clofazimine plus one of these drugs for an additional 18 months.
When ofloxacin resistance is also present, a fluoroquinolone should not be used as part of second-line treatment. The regimen of choice in such cases shall consist of 6 months of clarithromycin, minocycline and clofazimine followed by clarithromycin or minocycline plus clofazimine for an additional 18 months. Resistance has been reported from several countries, although the number of patients is small. Evidence on the potential benefits and harms of alternative regimens for drug-resistant leprosy was not available. Therefore, recommendations for second-line regimens are based on expert opinion and the known activity of alternative drugs, including the likelihood of cross-resistance. Prevention of leprosy through chemoprophylaxis the guidelines recommend the use of single-dose rifampicin (SDR) as preventive treatment for adult and child (2 years of age and above) contacts of leprosy patients, after excluding leprosy and tuberculosis (TB) disease and in the absence of other contraindications. The COLEP2 randomized controlled trial (RCT) found SDR in leprosy contacts associated with a 57% reduction in the risk of leprosy after 2 years and 30% after 5–6 years; SDR also appears highly cost–effective, with an incremental cost–effectiveness ratio of US$ 158 per additional prevented leprosy case.
The ability of programmes to adequately identify and manage contacts of persons with leprosy is a prerequisite for successful implementation of the recommendation. Because leprosy is highly stigmatized, caution must be exercised when implementing SDR, particularly for contacts outside the patient’s family. Programmes must respect the wish of patients to disclose or not disclose their diagnosis. When patients do not authorize disclosure, the GDG does not recommend identification or screening of contacts, which is a prerequisite for prescribing preventive treatment. In hyperendemic settings, a blanket approach (i.e. treatment of all community members without identifying contacts) might be more feasible and reduce potential harms related to disclosure of a leprosy diagnosis. (11,12)
CONCLUSION
In conclusion, leprosy is a contagious disease caused by the bacteria Mycobacterium leprae. It is transmitted through prolonged and close contact with an infected person and is not highly infectious.
REFERENCES

Akanksha Surwase, Kajal Jethliya, Argade Shivani, Gadakh Paurnima, Amol Wadhave, A Review on Leprosy: Epidemiology, Pathophysiology and Treatment, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1267-1275. https://doi.org/10.5281/zenodo.16812571
 10.5281/zenodo.16812571
10.5281/zenodo.16812571
