Dr. K. V. Subba Reddy Institute of Pharmacy, Dupadu, Pharm D VI Year.
Decompensated Chronic Liver Disease (DCLD) signifies the advanced stage of cirrhosis, characterized by the emergence of critical complications such as ascites, hepatic encephalopathy, variceal bleeding, and hepatorenal syndrome (HRS). This review aims to provide an in-depth overview of DCLD, including its epidemiology, underlying pathophysiology, diagnostic approaches, risk factors, and current management strategies. Cirrhosis results from persistent liver injury that leads to fibrosis and irreversible architectural damage. It is a global health concern, with increasing prevalence in developing countries like India, largely due to rising rates of alcohol use, obesity, and viral hepatitis. The transition from compensated to decompensated cirrhosis marks a significant decline in survival outcomes. The main causes include alcohol-related liver disease, viral hepatitis (B and C), NAFLD, and various autoimmune and genetic disorders. Diagnosis is based on clinical features, lab investigations, imaging studies, and prognostic scoring systems such as Child-Pugh and MELD. Management is multidisciplinary and includes interventions for complications such as portal hypertension, ascites, encephalopathy, and renal failure. Liver transplantation remains the definitive treatment. Early detection and targeted therapy can substantially improve clinical outcomes and reduce disease burden.
Cirrhosis is a progressive liver condition where healthy hepatic tissue is replaced by fibrotic scar tissue, ultimately impairing liver function. The liver loses its ability to perform vital roles such as metabolism, detoxification, and protein synthesis. Persistent liver injury from alcohol, viruses, or metabolic disorders leads to structural remodeling and irreversible damage.
Key Features of Cirrhosis
Fibrosis and Scarring: Chronic damage results in fibrous tissue accumulation.
Loss of Function: Normal liver processes are disrupted, including bile production and ammonia clearance.
Progressive Nature: Complications arise as liver function declines.
Stages if Cirrhosis
Compensated Stage: Patients remain asymptomatic without signs such as ascites, encephalopathy, or jaundice.
Decompensated Stage: Characterized by clinical manifestations including ascites, variceal bleeding, and encephalopathy. The onset of decompensation is associated with a significant decrease in survival.
Epidemiology
Cirrhosis represents a major global health challenge. Its prevalence ranges from 4.5% to 9.5% in the general population. In 2017, it accounted for over 1.3 million deaths worldwide. In countries like India, increasing alcohol use, viral hepatitis, and obesity have contributed to the rising incidence of cirrhosis.
Etiologies Of Cirrhosis
The primary causes of cirrhosis include:
Alcoholic Liver Disease
Non-Alcoholic Fatty Liver Disease (NAFLD)
Hepatitis B and C Infections
Autoimmune Liver Disorders
Metabolic and Genetic Disorders (e.g., Wilson’s disease, hemochromatosis)
Iatrogenic and Toxic Injuries (e.g., certain medications, arsenic)
Other categories:
Viral: HBV, HCV, HDV
Autoimmune: Autoimmune hepatitis, primary biliary cholangitis
Metabolic: NAFLD, NASH, alpha-1 antitrypsin deficiency
Vascular: Budd-Chiari syndrome
Genetic: Cystic fibrosis
Toxic: Alcohol, drugs
Pathophysiology
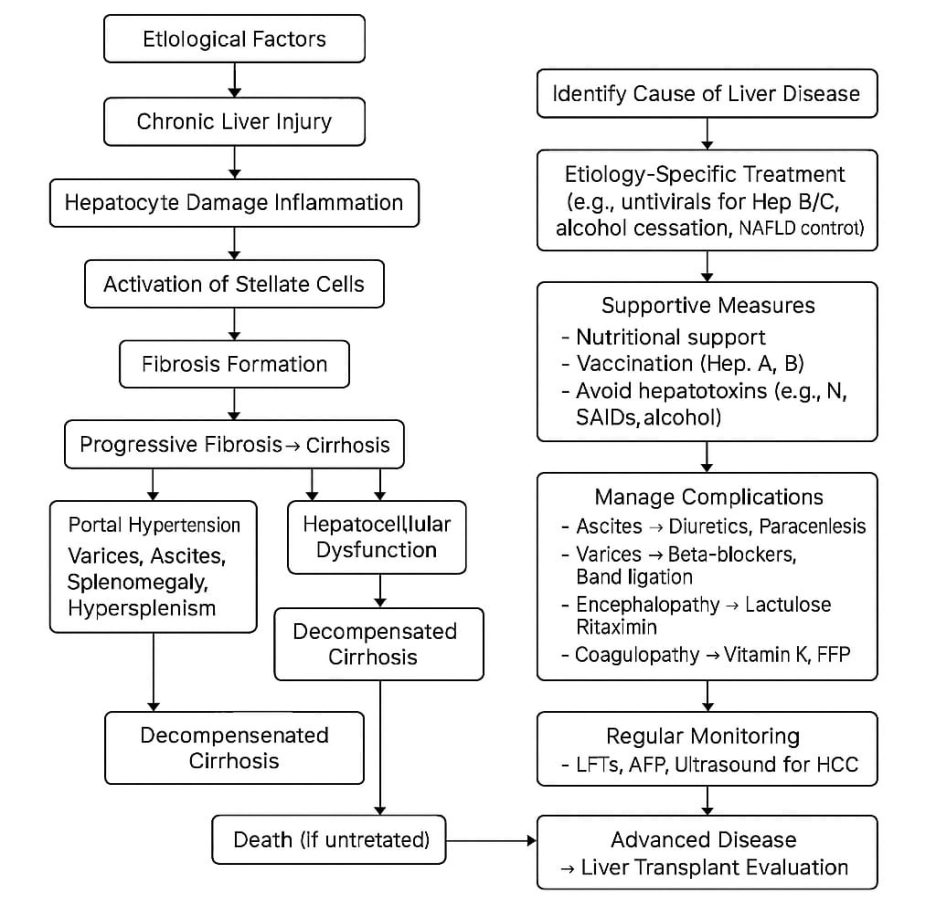
The development of cirrhosis involves persistent hepatic inflammation, regeneration of hepatocytes, and fibrotic remodeling. As intrahepatic resistance rises, portal hypertension develops. This leads to splanchnic vasodilation, systemic circulatory changes, and multi-organ dysfunction in advanced stages.
Risk Factors
DIAGNOSIS OF DCLD
Clinical Evaluation
History: Focuses on alcohol use, hepatitis exposure, comorbidities
Physical Examination: Includes assessment for jaundice, ascites, mental status changes
Laboratory Tests
LFTs: Bilirubin, albumin, PT/INR
CBC: To detect thrombocytopenia
Electrolytes: Monitoring for hyponatremia
Imaging
Ultrasound/CT/MRI: Evaluate liver morphology and ascites
Elastography (FibroScan): Assesses liver stiffness
Scoring Systems
Child-Pugh Score: Classifies severity based on labs and clinical features
MELD/MELD-Na Score: Predicts mortality using bilirubin, INR, creatinine, and sodium
Management Strategies
Portal Hypertension
Assessed via HVPG; treatment includes NSBBs (e.g., propranolol, carvedilol), somatostatin analogues, and vasopressin to reduce portal flow.
Esophageal Varices
Ascites
Hepatic Encephalopathy
Hepatorenal Syndrome
CONCLUSION
Decompensated Chronic Liver Disease represents a critical stage in the progression of cirrhosis, marked by life-threatening complications. Its onset significantly worsens prognosis and increases healthcare burden globally. Early identification and prompt management of complications like ascites, variceal bleeding, encephalopathy, and hepatorenal syndrome are crucial for improving patient outcomes. A multidisciplinary approach combining medical therapy, nutritional support, and consideration for liver transplantation is essential. Preventive strategies targeting alcohol use, obesity, and hepatitis can reduce disease incidence. Prognostic scoring systems such as MELD and Child-Pugh aid in risk stratification and treatment planning. Despite advancements, DCLD remains a major cause of mortality, especially in developing countries. Public health initiatives and patient education are vital for early intervention. Continued research is needed to refine therapeutic strategies and optimize transplant allocation. Ultimately, improving awareness, access, and early care can significantly reduce the burden of advanced liver disease.
REFERENCES

Shaik Irshad Nufshrun*, Dr. M. Sri Ramachandra, G. Kavya, Shaik Khalid, A Comprehensive Review on The Complications of Decompensated Liver Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1021-1025. https://doi.org/10.5281/zenodo.16793526
 10.5281/zenodo.16793526
10.5281/zenodo.16793526
