School of pharmacy Rai University Ahmedabad.
Pyria, also called pyorrhea alveolaris or periodontitis, is a long-lasting disease that affects the tissues supporting the teeth, such as the gums, the ligament around the teeth, and the jawbone. It is mainly caused by bacterial infection due to poor oral hygiene and the buildup of plaque. Over time, the disease causes gum inflammation, pus, and eventually, the teeth can become loose or fall out if not treated. Factors like smoking, diabetes, hormonal changes, and not getting enough nutrients can make the disease worse. Catching pyria early by checking the mouth and using X-rays is important for proper treatment. Treatment includes professional dental cleaning, using medicines to control bacteria, and, in serious cases, surgery. Good oral hygiene, regular dental visits, and a healthy diet help prevent pyria. This review explains what causes pyria, how it develops, its symptoms, and how to manage it, highlighting the importance of prevention and awareness for good oral health.
Pyria, also called Pyorrhea Alveolaris or Periodontitis, is a long-lasting inflammatory and infectious disease that affects the tissues supporting the teeth, such as the gums, periodontal ligament, cementum, and jawbone. It is one of the most common oral health problems around the world and a main cause of tooth loss in adults. The main reason pyria happens is because bacteria from dental plaque and tartar collect along the gum line, which leads to inflammation and damage of the tissues around the teeth (Newman et al., 2022; Pihlstrom et al., 2005).
Risk factors that make the disease get worse include poor oral hygiene, smoking, not getting enough nutrients (especially vitamin C), hormonal changes, and health conditions like diabetes (Löe, 1967; Slots, 2017). In the early stage, pyria appears as gingivitis, showing redness, swelling, and bleeding of the gums. If not treated, it can develop into periodontitis, which causes pockets to form around the teeth, loss of jawbone, and teeth becoming loose (Armitage, 1999).
Besides its effects in the mouth, pyria has also been linked to other health problems like heart disease, lung infections, pregnancy issues, and poor blood sugar control in people with diabetes (Tonetti & Van Dyke, 2013; Kinane et al., 2017). This makes it important to understand what causes pyria, how it develops, and how to manage it, for both oral and overall health. Preventing pyria and catching it early with regular dental visits, good oral hygiene, and health education can greatly reduce the number of cases and complications (AlJehani, 2014).
This review gives a summary of pyria, including its causes, how it works in the body, its symptoms, how it’s diagnosed, and management options, while highlighting the importance of taking care of your teeth and gums to prevent it.
Etiology (Causes)
Pyria, or periodontitis, is caused by a mix of different factors, including bacteria, behavior, nutrition, and other health conditions. The main causes are:
Bacterial Infection:
The main cause of pyria is infection from harmful bacteria, especially Porphyromonas gingivalis, which lives under the gums and causes inflammation that destroys tissue and bone (Socransky & Haffajee, 1992; Hajishengallis & Lamont, 2012).
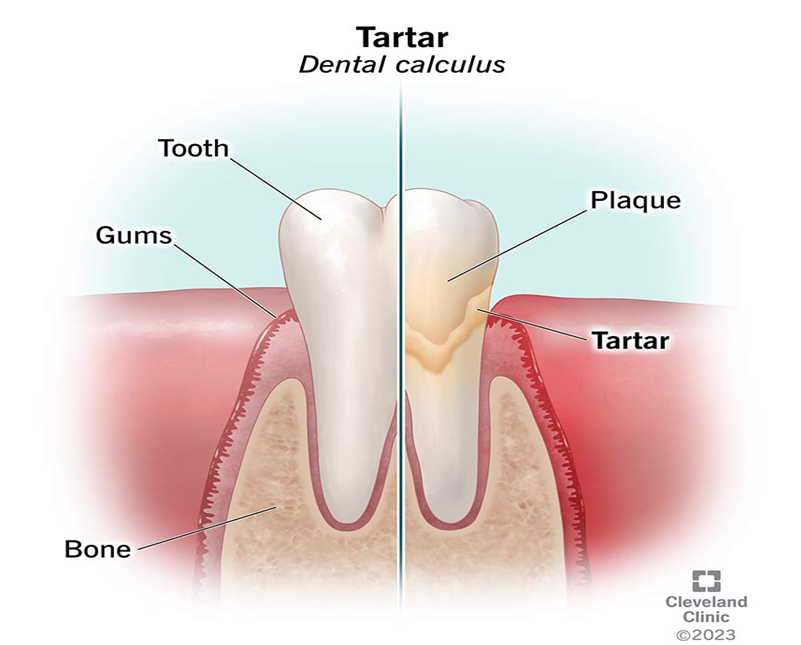
Plaque and Tartar Accumulation:
Dental plaque is a sticky film of germs on the teeth that starts periodontal disease. If it isn’t cleaned off regularly, it hardens into tartar, which keeps bacteria in place and continues to cause inflammation (Lindhe et al., 2015
Poor Oral Hygiene:
Not brushing, flossing, or visiting the dentist enough leads to plaque buildup, which causes gingivitis and can develop into periodontitis (Preshaw & Bissett, 2010).

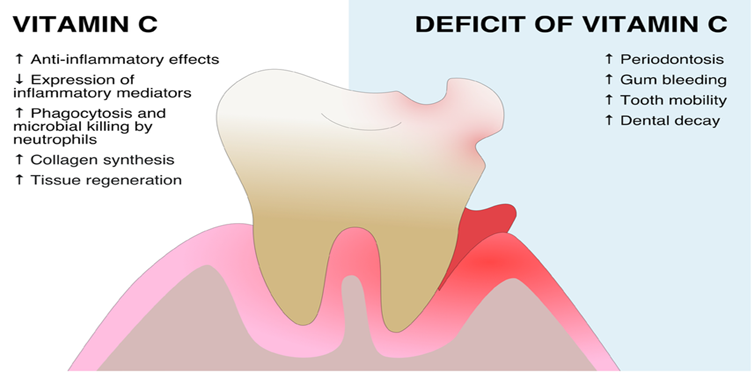
Nutritional Deficiency (Vitamin C):
Not getting enough vitamin C weakens the gums and makes them more likely to bleed and get infected (Nishida et al., 2000).
Tobacco Use:
Smoking and using tobacco reduces blood flow to the gums, weakens immune response, and speeds up gum disease (Bergström, 2004).

Diabetes Mellitus:
High blood sugar in diabetes affects the immune system and healing in the gums, increasing the risk and severity of gum disease (Preshaw et al., 2012).
Hormonal Imbalance:
Changes in hormones during puberty, periods, pregnancy, or menopause make gums more sensitive and likely to become inflamed, raising the risk of periodontitis (Mariotti, 1994).
In summary, pyria develops because of a combination of bacteria, local conditions in the mouth, and overall health factors. This is why both good dental care and looking after your general health are important for prevention and treatment.
Pathophysiology
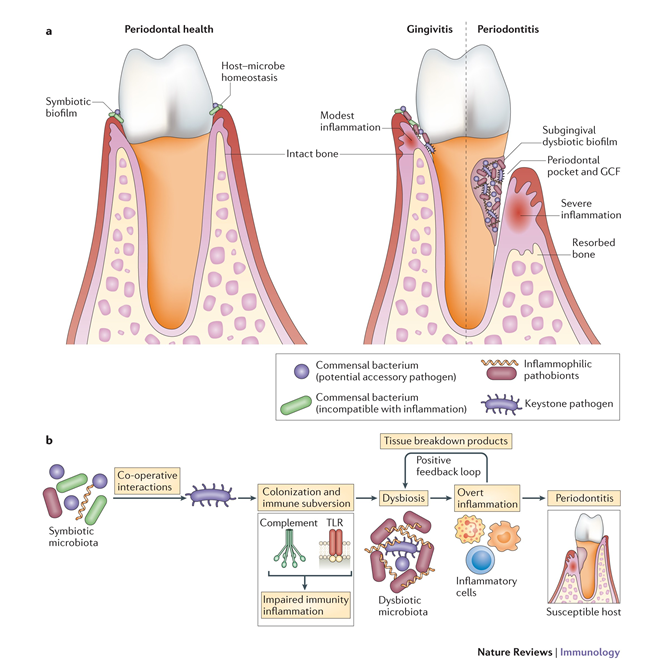
Pyria is a long-lasting inflammatory disease of the tissues supporting the teeth. It develops through a complex process involving harmful bacteria and the body’s immune response. The disease usually starts when dental plaque—a sticky film with bacteria—builds up along the gum line. Key bacteria, such as Porphyromonas gingivalis, Tannerella forsythia, and Aggregatibacter actinomycetemcomitans, play major roles in starting gum inflammation (Socransky & Haffajee, 1992; Hajishengallis & Lamont, 2012).
When the body detects these bacteria, it activates immune cells like neutrophils, macrophages, and lymphocytes. These cells release pro-inflammatory chemicals such as interleukin-1β (IL-1β), tumor necrosis factor-alpha (TNF-α), and prostaglandins (Kornman, 2008). While these chemicals are meant to fight infection, they also cause damage to gum tissue. Ongoing inflammation breaks down the periodontal ligament, causes the jawbone to be resorbed, and leads to loss of the tissue that keeps teeth in place—creating deep pockets around the teeth (Page & Kornman, 1997).
As pyria gets worse, the bacteria in the mouth shift from mostly gram-positive (less harmful) to gram-negative (more harmful) types, which further drive inflammation and tissue destruction. Both the body’s cells and the bacteria release substances like matrix metalloproteinases (MMPs), which speed up the breakdown of collagen and bone (Graves & Cochran, 2003).
Other health factors, such as diabetes, smoking, and hormone changes, can make the body’s inflammatory response stronger and slow down healing, making pyria more severe (Preshaw et al., 2012). In the mouth, this disease process leads to bleeding gums, gum recession, deep pockets, loose teeth, and eventually tooth loss.
Understanding how pyria develops is important for creating effective treatments, like professional cleaning, antibiotics, and therapies that target the body’s immune response to control inflammation and prevent further damage.
Clinical Symptoms
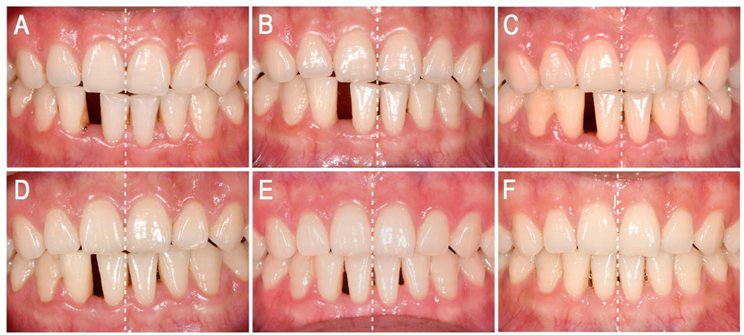
Pyria usually starts as gingivitis and can develop into periodontitis, showing symptoms that match the damage happening in the gums and other supporting tissues. Main symptoms include:
Gingival Inflammation and Redness
In the early stage, the gums become swollen, tender, and red because of inflammation caused by plaque buildup (Armitage, 1995; Newman et al., 2022).

Bleeding Gums
Bleeding often happens during brushing, flossing, or sometimes even without touching the gums. This is a key sign of gum inflammation (Newman et al., 2022)

Gum Recession
As the disease gets worse, the gums pull away from the teeth, exposing the tooth roots, which can make teeth more sensitive (Lindhe et al., 2015).

Periodontal Pocket Formation
When the ligament and bone around the teeth are destroyed, deep pockets form between the teeth and gums. These pockets trap bacteria and make the disease worse (Page & Kornman, 1997).

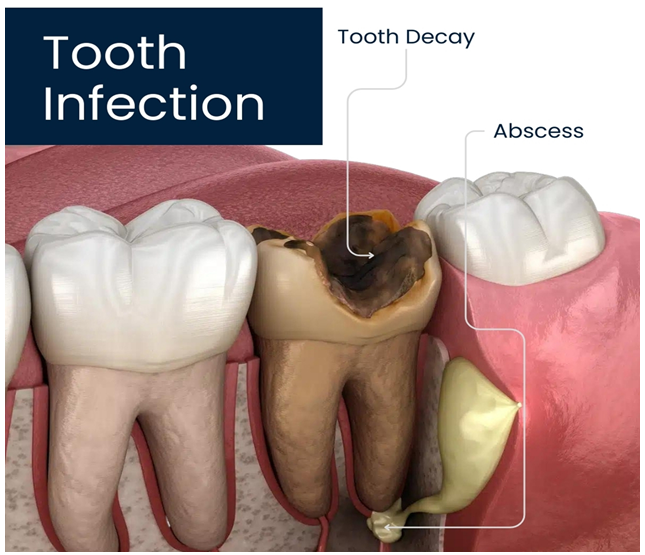
Pus Discharge (Suppuration)
Sometimes, pus may come out of these pockets, showing an active infection and tissue breakdown (Socransky & Haffajee, 1991)
Tooth Mobility and Migration
As the support for the teeth is lost, teeth can become loose and may even shift out of place (Lindhe et al., 2015).
Halitosis (Bad Breath)
Constant bad breath is common, caused by bacteria and the breakdown of tissue in the mouth (Kinane et al., 2017).
Pain or Discomfort While Chewing
While often mild, chewing can become uncomfortable or even painful, especially if the disease is advanced (Page & Kornman, 1997).
Recognizing these symptoms early is important for diagnosis and treatment to prevent permanent damage to gums and teeth.
Diagnosis
Diagnosing pyria (periodontitis) requires a detailed check-up using clinical exams, X-rays, and sometimes lab tests to see how much damage has been done to the gums and supporting tissues. Catching it early is important to prevent tooth loss and help with treatment.
Clinical Examination:
The dentist first looks inside the mouth to check the color, shape, and feel of the gums, and to see if there is bleeding, swelling, or gum recession. They also look for plaque, tartar, and loose teeth—all signs that the gums are affected (Newman et al., 2022; Lindhe et al., 2015).
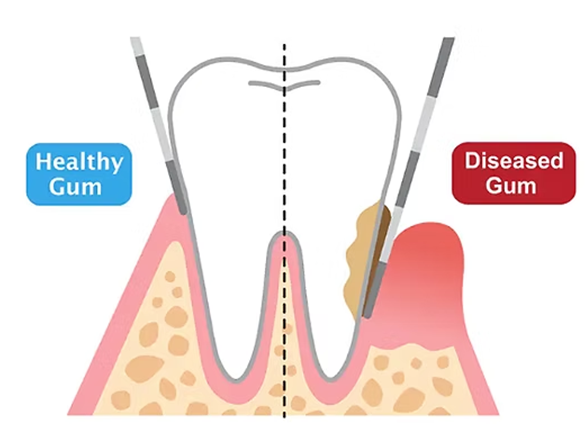
Periodontal Probing:
A special tool called a periodontal probe is used to measure the depth of the spaces (pockets) between the teeth and gums. If these pockets are deeper than 3 mm and bleed when probed, it means there is tissue loss and ongoing inflammation (Armitage, 1999).
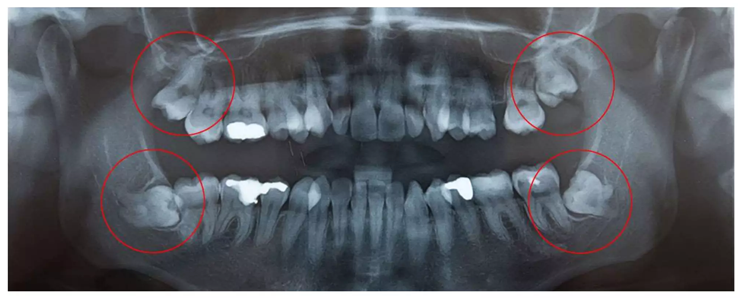
Radiographic Assessment:
Dental X-rays (like periapical or bitewing) help the dentist see bone loss around the teeth. Signs such as horizontal or vertical bone loss, widening of the space around the tooth root, and loss of bone lining show periodontitis (Jeffcoat, 1992; Hausmann, 2000).
Mobility and Furcation Involvement Tests:
The dentist checks if any teeth are loose (graded with Miller’s index) or, in the case of back teeth with more than one root, if the spaces between roots are affected (using Nabers probe). These tests help show how severe the disease is (Miller, 1950).

Microbiological and Biochemical Tests:
Lab tests can detect specific bacteria (like Porphyromonas gingivalis, Tannerella forsythia, and Aggregatibacter actinomycetemcomitans) that cause pyria. Biomarkers in the fluid from the gums, such as IL-1β, TNF-α, and MMPs, can also show if the disease is active (Socransky & Haffajee, 1991; Kinane et al., 2017).

Systemic Health Evaluation:
It’s important to check for other health conditions, such as diabetes or hormonal changes, because these can make pyria worse or harder to treat (Lindhe et al., 2015).
By combining these exams and tests, the dentist can accurately diagnose pyria and plan the right treatment for each patient
Treatment and Management
The main goals in treating pyria (periodontitis) are to get rid of infection, stop the disease from getting worse, and restore gum health. Treatment usually includes both non-surgical (medical) and surgical (dental) methods, along with patient education and regular maintenance.
1. Non-Surgical / Medical Management
a. Mechanical Plaque Control
The most important step is removing plaque and tartar through professional cleaning, known as scaling and root planing (SRP). This helps remove bacteria and smooth the tooth roots to promote healing (Newman et al., 2022; Lindhe et al., 2015).
b. Antimicrobial Therapy
Mouthwashes like chlorhexidine (0.12–0.2%) help control plaque. In tougher cases, antibiotics such as amoxicillin and metronidazole may be used. Medicines like doxycycline gel or minocycline microspheres can be placed directly in gum pockets to target infection (Herrera et al., 2002; Slots & Ting, 2002).
c. Anti-inflammatory and Supportive Therapy
Medicines like NSAIDs can help reduce gum swelling. Eating a healthy diet with enough vitamin C and antioxidants also helps with healing and boosts the immune system (Chapple & Matthews, 2007).
d. Patient Education and Oral Hygiene
Teaching patients how to brush, floss, and use dental aids is key for keeping gums healthy. Stopping smoking is also very important (Lindhe et al., 2015; Preshaw et al., 2012).
2. Surgical / Dental Management
a. Flap Surgery (Periodontal Surgery)
If deep pockets remain after non-surgical care, surgery may be needed. Flap surgery lifts the gums so the dentist can clean deep areas and remove infected tissue (Ramfjord & Nissle, 1974).
b. Regenerative Procedures
When there is a lot of bone loss, treatments like bone grafts, guided tissue regeneration (GTR), or special growth factors can help rebuild lost gum and bone (Reynolds et al., 2015).
c. Gingivectomy and Gingivoplasty
These surgeries remove diseased gum tissue and reshape the gums for better health and appearance (Newman et al., 2022).
d. Maintenance Therapy
After treatment, patients need regular check-ups and cleanings every 3–6 months to keep the disease from coming back (Axelsson & Lindhe, 1981).
3. Home Remedies and Herbal Support (Adjunctive Care)
Some herbal remedies, like neem, clove oil, green tea extract, and aloe vera, have antibacterial and anti-inflammatory properties. They can be used along with professional care, but should not replace it (Grover et al., 2011).
Prevention
Preventing pyria (periodontitis) mainly involves keeping good oral hygiene and reducing risk factors that lead to gum disease. Since pyria is mostly preventable, regular personal dental care and professional check-ups are very important.
Maintain Good Oral Hygiene
Brush your teeth twice a day with fluoride toothpaste, using the right brushing technique (like the modified Bass method) to remove plaque and prevent gum problems (Lindhe et al., 2015). Use dental floss, interdental brushes, or a water flosser to clean between teeth where a toothbrush can’t reach (Newman et al., 2022).
Regular Dental Visits and Professional Cleaning
Go to the dentist every six months for check-ups and professional cleaning. The dentist can spot early gum problems and remove plaque and tartar that brushing alone can’t get rid of (Axelsson & Lindhe, 1978).
Balanced Diet and Nutrition
Eat a healthy diet rich in vitamins (especially C and D), minerals (like calcium and phosphorus), and antioxidants to support healthy gums and tissue repair. Drink enough water to keep your mouth clean and your saliva flowing (Nishida et al., 2000; Chapple, 1997).
Avoid Tobacco and Limit Alcohol
Smoking and tobacco are major risk factors for gum disease, weakening your immune system and slowing healing. Quitting tobacco and cutting back on alcohol are important for keeping your gums healthy (Johnson & Hill, 2004).
Manage Systemic Diseases
Keep conditions like diabetes and hormone imbalances under control, as they increase your risk of gum infections. Regularly check your blood sugar if you have diabetes, and look after your overall health (Preshaw et al., 2012).
Manage Stress and Maintain a Healthy Lifestyle
Chronic stress can weaken your immune system and make you more likely to get infections, including gum disease. Managing stress with activities like yoga, meditation, and getting enough sleep helps protect your gums (Genco et al., 1999).
Education and Public Awareness
Community oral health programs, school dental check-ups, and awareness campaigns are important for teaching people about good oral hygiene and preventing gum disease at a community level (Petersen & Ogawa, 2005).
CONCLUSION
Pyria, also known as periodontitis, is a long-lasting infection and inflammation that slowly destroys the tissues supporting the teeth, eventually causing tooth loss if not treated. The main cause is the buildup of bacterial plaque, but the disease can get worse due to factors like diabetes, poor nutrition, hormonal changes, smoking, and not taking care of your teeth.
Catching pyria early and managing it properly is very important to stop the disease and prevent lasting damage. The first step in treatment is usually non-surgical, such as professional cleaning (scaling and root planing). For more serious cases, surgery and procedures to rebuild gum and bone may be needed. Using antimicrobial products and teaching patients about good oral hygiene helps improve results.
Preventing pyria depends on keeping up with daily oral hygiene, visiting the dentist regularly, and living a healthy lifestyle. Public education and community dental health programs are also important to lower the number of cases. Focusing on prevention not only keeps your mouth healthy but also supports general health, since gum disease is linked to heart disease, diabetes, and other chronic problems.
In summary, pyria can be prevented. Education, early action, and a lifelong commitment to oral hygiene are key to having healthy gums and teeth.
REFERENCES

Pratyush Kumar Brahma*, Almash Shekh, A Comprehensive Review on Pyria (Pyorrhea Alveolaris) Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 3121-3135 https://doi.org/10.5281/zenodo.17661175
 10.5281/zenodo.17661175
10.5281/zenodo.17661175
