Department of Pharmacology, Sankaralingam Bhuvanswari College of Pharmacy, Anaikuttam, Sivakasi – 626130.
Anasarca, which is often referred to as global edema, is a severe and extensive buildup of fluid in the bodily cavities and interstitial tissue. This case study examines the effects of anasarca therapy on patients who have previously experienced a cerebrovascular accident (CVA), also referred to as a stroke. Clinicians face particular difficulties in controlling anasarca in patients who have had a cerebrovascular accident (CCA). The clinical presentation, diagnostic process, and treatment strategy for a 40-year-old female patient with severe anasarca are described in this case study. The patient's medical history, physical examination findings, and test results indicated a complex etiology that included scanty micturition, anemia, dyspnea, chronic portal vein thrombosis, and type 2 diabetes. To treat the underlying causes and reduce symptoms, an extensive and multidisciplinary strategy is necessary for the care of anasarca. We aim to show the difficulties in identifying and treating anasarca through this case study and to discuss the value of individualized therapy in enhancing patient outcomes.
Severe widespread fluid collection in the interstitial space is known as anasarca. The causes of this generalized edema include capillary filtration exceeding the fluid removed by lymphatic drainage, an increase in intravascular hydrostatic pressure, an increase in endothelial barrier permeability, a decrease in oncotic pressure within the capillary, or a change in oncotic pressure from low protein states. Anasarca is characterized by widespread, enormous swelling as opposed to the localized swelling of peripheral edema. Anasarca can be brought on by a number of clinical disorders, such as lymphatic system impairment, liver failure, heart failure, or renal failure. Patients may present with anasarca in many ways, but when the interstitial volume is greater than 2.5 to 3L, it usually becomes clinically visible. [1] [2][3] The primary trait is a considerable buildup of fluid in the interstitial
spaces, which causes obvious swelling in the face, arms, legs, belly, and other parts of the body. Anasarca is a symptom of an underlying medical issue that is primarily diagnosed by clinical evaluation rather than a distinct disease. The main goal of diagnostic testing is to determine the underlying cause, while they can also help in determining the degree and locations of edema. Diuretics are usually used in conjunction with treating the underlying cause as part of treatment. Consequently, it's critical to identify and address the underlying illness as soon as possible [4]. A cerebrovascular accident (CVA) happens when there is cerebral ischemia or hemorrhage that leads to the death of brain cells. Loss or impairment occurs to functions that were regulated by the damaged part of the brain, such as movement, sensation, or emotions [5]. The Indian Stroke Association [ISA] declares. From 1970–1979 to 2000–2008, the incidence of stroke increased by more than 100% in low- and middle-income nations, including India [6].
Case Report:
In 4 days, a 40-year-old female patient complained of dyspnea, abdominal distension, and scanty micturition. She was admitted to the government headquarters hospital in Virudhunagar, Tamil Nadu. They gave us an ethical certificate for performing this study, with reference number R. No. 110/HS/GHQH-VNR/SEP 2019. The patient's medical history is without vomiting, fever, loose stools, hematuria, dysuria, or expectoration in the cough. The patient already has a history of chronic portal vein thrombosis, left side hemiplegia, previous CVA, and type 2 diabetes. The patient's past prescription history includes T. amlodipine (2–3 mg), T. atovastatin (10 mg), T. propanalol, T. aspirin, and T. nicoumalone. The patient's pulse (106 beats per minute) is abnormal. A systemic review of CVS indicates that S1S2 is within normal limits. In the RS examination, BAE is normal. The examination reveals a distended abdomen from a fluid buildup. The right side of the CNS examination is normal, while the left side's upper and lower limb tones are faint. B/L of the CNS Neurological Pupil Index (NPI) is regarded as normal in the examination (range -3.0 mm). The patient presents with generalized anasarca, bilateral pedal edema, and pallor. Based on this diagnosis, we can see that the patient suffers from severe anemia, left-sided hemiplegia, chronic portal vein thrombosis, and type 2 diabetes mellitus.
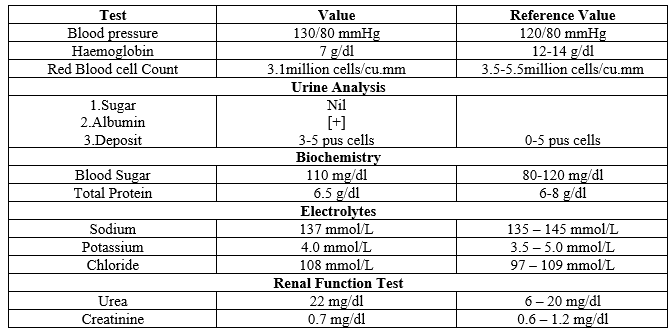
Table 1: Clinical Laboratory Investigation Report
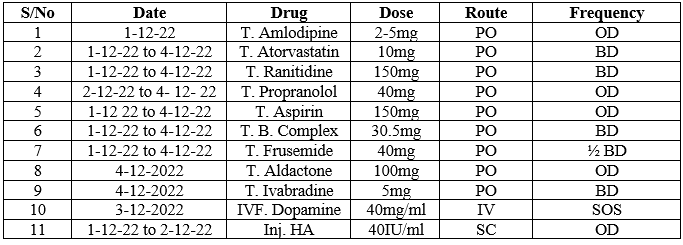
Table 2: Treatment Chart
Patient Counseling For Drugs:
The patient was advised to take T. amlodipine 2–5 mg have to be taken in the morning, and T. atorvastatin 10 mg of 2 tablets have to be taken at night. T. Ranitidine 150 mg tablets have to be taken in the morning and night. T. Propanalol 40 mg; half of the tablets have to be taken in the morning and night. T. Aspirin 150 mg has to be taken in the afternoon.. T. frusemide 40 mg; half of the tablets have to be taken in the morning and afternoon. T.BCT needs to be taken both at night and in the morning. Give the patient ionotropes such as dopamine if their blood pressure is less than 80 mmHg.
DISCUSSION:
A systemic edema, or an extensive buildup of fluid in the bodily cavities and interstitial tissue, is known as an anasarca. The causes of this generalized edema include capillary filtration exceeding the fluid removed by lymphatic drainage, an increase in intravascular hydrostatic pressure, an increase in endothelial barrier permeability, a decrease in oncotic pressure within the capillary, or a change in oncotic pressure from low protein states. Anasarca is frequently caused by congestive heart failure.Because of a lower preload, a higher afterload, and a reduced ejection fraction. Vascular fluid leaks into the interstitium as a result of this condition [7]. Reduced capillary oncotic pressure can occur from necessary protein loss brought on by renal disorders (glomerulonephritis) [8] [9]. Generalized nonpitting edema can be brought on by fluid retention from certain endocrinological illnesses (certain gastrointestinal ailments, such as celiac disease, cause intestinal protein loss, resulting in vascular fluid; hypothyroidism is one such condition) [10]. Anasarca can be brought on by a number of inflammatory diseases, such as rheumatoid arthritis, systemic lupus erythematosus, and dermatomyositis, because of increased vascular wall permeability [11]. The patient's medical, surgical, and pharmacological histories should all be included in the whole history. Edema can be brought on by comorbidities, postsurgical problems, and certain drugs (like amlodipine) [12]. This 40-year-old female patient was taken to the Virudhunagar government headquarters hospital in Tamil Nadu after complaining of abdominal distension and pain within four days. In order to treat a documented case of cerebrovascular accident, the patient is currently on medication. Anasarca examination is primarily concerned with determining the underlying reason and ruling out alternative diagnoses. Because many organ systems (e.g., urinary, cardiovascular, and respiratory) are impacted simultaneously, clinicians from various specialties (e.g., cardiology, nephrology, gastroenterology, and oncology) often need to work together to pinpoint the primary etiology [13]. The main method of diagnosing anasarca is via physical examination, when distinctive findings are made. Vital symptoms (e.g., tachycardia, tachypnea, reduced oxygen saturation) may be indicative of secondary disorders resulting from fluid overload [14]. Diuretic therapy may not be beneficial in patients with localized edema caused by malignant ascites, venous or lymphatic blockage, or both, as it can cause volume depletion. However, it is advised that a loop diuretic, such as furosemide or bumetanide, be used as the first line of treatment in cases of severe generalized edematous conditions, such as congestive heart failure [15]. Since primary care physicians are frequently the first to see patients and are able to recognize anasarca at an earlier stage of sickness, they are essential in the early diagnosis of the underlying disease. While physical and occupational therapists work with individuals whose mobility and lifestyle have been impaired by anesthesia, pharmacists make sure that drugs are prescribed safely.
CONCLUSION:
This case illustrates the complexity of managing anasarca in a patient with a history of CVA and multiple comorbidities. A multidisciplinary approach is essential for successful treatment, focusing on the underlying causes and symptomatic relief. Regular monitoring and adjustments in treatment plans are crucial to addressing the dynamic nature of the patient’s condition.
REFERENCE


Dr. Vigneswaran R.*, Natarajan P., Saravana Kumar R., Jeniba E., Kaviya V., Pasupathy P., A Case Report On Anasarca – The Whole Body Swelling, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 8, 3415-3419. https://doi.org/10.5281/zenodo.13337899
 10.5281/zenodo.13337899
10.5281/zenodo.13337899
