Department of Pharmaceutics, Sankaralingam Bhuvaneswari College of Pharmacy, The Tamil Nadu Dr. M.G.R. Medical University, Sivakasi - 626130, Tamil Nadu, India
The transdermal route of drug administration using films is one of the promising approaches for delivering therapeutic agents, which has benefits like the longer-lasting release, fewer systemic side effects, and increased patient compliance. To maximize the safety and efficacy of transdermal film formulations, it is mandatory to understand and resolve various issues associated with this drug delivery system. Overcoming the skin's barrier properties to enable drug penetration, guaranteeing drug stability in the film, reducing skin irritation and sensitization, attaining consistent drug release, delivering precise dosage, improving patient acceptance and adherence are major challenges. Strategies developed to address these issues includes, the use of barrier coatings and stabilizers to protect drug stability; formulation of medications with skin-compatible excipients to reduce irritation; use of nano-emulsions, micro-needles, and vesicular carriers to enhance drug permeation; use of precise manufacturing techniques to achieve precise dosage and consistent medication distribution; etc., Patient acceptance and adherence can be enhanced by patient-centric strategies like the development of thin, flexible and discrete films as well as the provision of clear instructions and educating materials. Hence, in the presence of an existing knowledge bank and well-designed strategies, various issues encountering can be resolved and therapeutics can be delivered more efficiently through transdermal route using patches.
Transdermal drug delivery systems (TDDS) are dosage forms designed to deliver a therapeutically effective amount of drug across a patient’s skin. The skin is the largest organ in the human body by mass (15% of total weight), with an area between 1.5 and 2.0 m2 in adults. Drugs have been applied to the skin to treat superficial disorders, for the transdermal administration of therapeutics to manage systemic ailments, and as cosmetics for make-up, perfume, deodorant and grooming aids[1-2]. Transdermal drug delivery is a non-invasive or minimally invasive method that allows a certain amount of drug to pass through the epidermal layer of the skin by free diffusion or other means and continues to enter the systemic blood circulation at a controlled rate[3]. The transdermal route is currently the most promising drug delivery method because it reduces the pulsed entry of the drug into the systemic circulation, controls or sustains the release of the drug and avoids drug toxicity, increases bioavailability by avoiding first-pass metabolism and permits constant input of the drug with a short biological half-life[4]. Various formulations like ointment, creams, sprays, gels or patches are suitable to deliver the drugs through the skin for local and systemic therapeutic effects. Owing to various factors limited number of drugs only can be delivered through this route. A transdermal patch is a medicated patch that can be applied topically to provide medication at a specified rate directly into the bloodstream via the layers of the skin and is the easiest way to provide medication[5]. By avoiding the digestive system and liver metabolism, transdermal patches provide a more efficient and controlled way of delivering the active pharmaceutical ingredients, ultimately improving patient outcomes and treatment efficacy. Recent advancements in transdermal patches have resulted in smart patches having an ability to sense and release drugs accurately, higher loading, enhanced penetration, better drug release, degradable, dimensional (3D)-printed patches, etc. Various properties like release of the medicament from the vehicle, penetration through the skin barrier and activation of the pharmacological response influence transdermal delivery of drugs[6-10]. In Table 1, advantages, disadvantages and limitations of delivering drugs through the skin are presented [11-15].
Table 1: Advantages, disadvantages and limitations of transdermal drug delivery

This present review offers a comprehensive analysis of the basic components used in transdermal products, types, laboratory preparation of transdermal patches, testing methods for quality assessment and highlights the scale-up from R&D to large scale, commercial manufacturing, regulatory compliance and market status. The contents presented in this review serve as a valuable bridge for extending the research activities in the domain area of transdermal patches by understanding the challenges encountered in development to deliver drug candidates more safely and effectively.
COMPONENTS OF TRANSDERMAL DRUG DELIVERY SYSTEM
The basic components of a transdermal drug delivery system (TDDS) include a polymer matrix, plasticizer, membrane, pressure-sensitive adhesives, backing laminates, release liner and permeation enhancers etc., not all components need to be present in every transdermal patch. All Transdermal patches have the same backing film, medication reservoir, and release liner[16-18].
Polymer matrix:
The core of TDDS is polymers, which regulate drug release in both in-vivo or in-vitro conditions. Drugs can be dispersed in liquid or solid-state synthetic polymer bases to prepare a drug-polymer matrix. The polymers utilized in TDDS ought to exhibit both chemical and biocompatibility with the drug and additional system constituents like pressure-sensitive adhesives (PSAs) and penetration enhancers used. The polymer used should also be safe and deliver a drug consistently and effectively for the duration of the product's intended shelf life. Examples of polymer that controls the release of the drug from the device are given in Table 2.
Table 2: Polymers control the release of the drug from the device

Active pharmaceutical ingredient or drug molecule:
For successfully developing a transdermal drug delivery system, the physicochemical properties of the drugs need to be taken into consideration. A transdermal drug delivery system is ideal for drugs with a high initial pass metabolism, restricted time frame for therapy, a short half-life that leads to frequent dosing, non-patient compliance, lower dose per day, low molecular weight of less than 1000 daltons, sufficient solubility both in water and oil with log P between 1-3, minimal melting point of below 200°C and not induce any irritation or allergic responses.
Pressure-sensitive adhesives (PSAs):
These adhesives can be used to adhere any transdermal device to the skin. They can be placed on the device's face or in the back and extended outward. The first strategy is the creation of novel polymers, such as polyurethanes and hydrogel hydrophilic polymers. Another strategy involves altering the chemistry of the PSAs that are currently in use, such as acrylates, silicones, and polyisobutylene, either physically or chemically. Physical modification is the process of creating base adhesives with special additives that work in concert with the drug and excipients in the system formulation to improve skin adhesion and enhance drug delivery. Chemical modification is adding functional monomers chemically or grafting them onto conventional PSA polymers to improve drug delivery rates[19-21].
Backing membrane:
Printing needs to be acceptable by backing membranes. They should be more flexible and offer a strong bond to the drug reservoir. They also stop the drug from escaping the dosage form through the top. The product is protected from the skin during use by an impermeable substance, such as metallic plastic laminate, plastic backing with an absorbent pad, an occlusive base plate made of aluminium foil, an adhesive foam pad made of flexible polyurethane with an occlusive base plate made of aluminium foil discs, etc.
Drug release membrane:
The membrane regulates the drug's release from multilayer patches and the reservoir. It contributes to the control of the diffusion rate of the drug into the skin. When choosing the transdermal membranes, one should consider the material composition and thickness. Drug release from the dosage form is regulated by rate-controlling membranes found in transdermal devices. Rate-regulating membranes derived from naturally occurring polymeric materials, like chitosan, have a lot of potential applications. When bent or stretched, it should have enough flexibility to avoid breaking or cracking. Polyethylene sheets, cellulose acetate, and ethylene vinyl acetate co-polymer are a few types of rate-controlling membranes. Lately, transdermal application of composite poly-2-hydroxyethyl methacrylate (PHEMA) membranes has been investigated as a rate-limiting barrier.
Plasticizers:
While adding plasticizers of low molecular weight, the polymer's flexibility and plasticity are promoted. When added right quantity, these modify the polymer's mechanical and physical properties by lowering the glass transition temperature (Tg). More frequently used plasticizers include glycerine, propylene glycol, dibutyl phthalate, triethyl citrate, triacetin and polyethylene glycol.
Release liner:
The release liner is a material that provides a temporary protective layer to adhesive-coated products, preventing them from sticking to each other. The release liners will be coated with an anti-adherent material and its function is to safeguard the system while it is in the packaging; it will be taken out right before its topical application. Release liners are crucial to the patch's affectivity, stability, and safety, hence they should be carefully chosen. An improper release liner can interfere with the active ingredient or other components, making it difficult to release the patch and shortening its shelf life. The two main coating classes are fluro-polymers and silicones. The most frequently utilized types of release liner films are composite, paper, and plastic.
Transdermal permeation and penetration enhancers[22,23]
Transdermal permeation:
Transdermal permeation of drug molecules can take place by different mechanisms, which include:
Penetration enhancers:[24-26]
The transport via the sweat glands and along hair follicles with their associated sebaceous gland, it is necessary to use enhancers. The different layers present in the skin act as a barrier to the flow of penetrating molecules and these enhancers increase the permeation by their specific mechanism. Penetration enhancers are chemical substances that alter the stratum corneum's permeability to raise the drug's therapeutic level. These enhancers interact with the lipids and proteins that make up the stratum corneum's structural elements. They change the stratum corneum's protein and lipid packing, which chemically modifies the barrier's function and increases permeability. Permeation enhancers may be natural or chemical type. Natural penetration enhancers have less toxicity profile and do not produce irritation, ex. Eugenol. Various solvents increase penetration possibly by swallowing the polar pathway and/or by fluidizing lipids which include water alcohols, ex. methanol and ethanol. Other classes of enhancers which include alkyl methyl sulfoxides, ex. dimethyl sulfoxide; alkyl homologs, ex. methyl sulfoxide, dimethyl acetamide; anionic-surfactants, ex. dioctyl-sulphosuccinate, sodium-lauryl sulfate, decodecyl-methylsulphoxide; nonionic-surfactants; bile salts, ex. sodium taurocholate, sodium deoxycholate, sodium tauroglycocholate; binary systems, ex. propylene glycol-oleic acid and 1,4-butane diol-linoleic acid. At a safer level of concentration the chemical enhancers cause reversible damage to the skin layers and increase the drug's permeability to maximize the drug's thermodynamic activity. The ideal characteristics of permeation enhancers include being biocompatible and they should not irritating skin or triggering allergies over time. It shouldn't cause toxicity. Both chemically and physiologically, it should be stable. Body fluids and endogenous materials shouldn't leak out of it (unidirectional flow), and the skin should instantly regain its natural barrier qualities if these items are eliminated. It shouldn’t cause any permanent damage to sin layers and work efficiently with the medication being administered.
TYPES OF TRANSDERMAL PATCHES
Different types of transdermal patches are designed based on how the drug solution deploys during its process of manufacturing. Transdermal solutions can come in a liquid, gel, or crystallized solid form. Choosing a type of transdermal patch revolves around the most efficient skin transmission, delivery requirements of drug solution, the nature of the production set-up and the manufacturing feasibility[27-29].
Adhesive drug system
To create a drug reservoir, this kind of patch is made by combining the medication with an adhesive polymer. Subsequently, an impermeable backing layer was applied using either solvent casting or melting techniques. An unmediated adhesive polymer layer shields the reservoir's top. Drug-in-adhesive can be further divided into single-layer and multi-layer varieties. Numerous medications are suitable to work well with this system. Additionally, the system is capable of delivering multiple drugs in a single patch. It helps to influence patient preference by providing benefits like decreased size and thickness as well as better conformability to the application site. The single-layer drug in adhesive patches comprises the combination of drug and adhesive. The backing membrane and release liner are applied up and down the side of the adhesive layer. A single-layer patch is applied to the skin, where it sticks and deploys the drug. Multilayer drugs in adhesive patches are similar to the single-layer system in that adhesive layers release the drug, except additional adhesive layers containing drugs are present (more than one). Typically, multilayer transdermal adhesives deploy solutions over a longer period because the width of the layers determines how quickly the drug reaches the skin. In multiple layers, one can be for controlled release and the other for immediate drug release. The single and multiple drug-in-adhesive patches are presented in Figure 1.
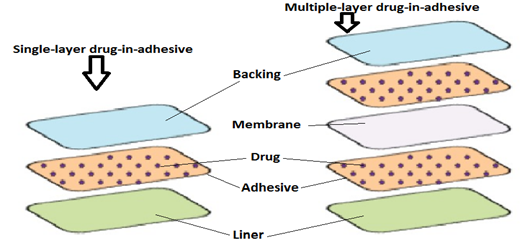
Figure 1: Adhesive Transdermal Drug Delivery System
Reservoir and matrix-dispersion system
Transdermal reservoirs are liquid layers containing the drugs which are gradually delivered to the skin through a rate-controlling membrane. These reservoir patches allow for more controlled delivery rates, but the initial drug release can come in a slight burst. In addition, if the membrane is damaged, there is a risk of sudden release in the skin. This system embeds the drug reservoir between a rate-controlling membrane and an impermeable backing layer. Only the rate-regulating membrane, which may or may not be microporous allows the drug to be released. The drug may be in the form of a gel, suspension, or solution, or dispersed throughout a solid polymer matrix within the drug reservoir compartment. A drug-compatible outer surface polymeric membrane made of hypoallergenic adhesive polymer. A transdermal matrix patch includes an adhesive polymer matrix containing the drug, which is gradually released into the skin. Unlike the rate-controlling membrane in a reservoir patch, the formulation of its drug and polymer matrix dictates the rate of drug delivery. The active ingredient is distributed evenly throughout the patch, so there is less risk of accidental release. The medication is uniformly distributed within a hydrophilic or lipophilic polymer matrix. After that, it is changed into a medicated disc with a distinct thickness and form. This medication-containing polymer disk is installed in a compartment made of a drug-impermeable backing layer, fixed to an occlusive base plate. To create an adhesive rim strip, the adhesive is not applied on the drug reservoir's face; rather, it is spread around its circumference. In Figure 2, components of reservoir (a) and matrix type (b) transdermal patches are presented.


Iontophoresis and Microneedle patches
Iontophoresis patches are medical devices that use small electrical currents to deliver charged substances to the skin. Iontophoresis relies on electro-migration to drive charged drugs under a direct electric field. As such, a stable power source is indispensable for the operation. An external power supply places a physiological and psychological load on patients. Thus, wearable or skin-mountable iontophoresis that incorporates lightweight and safe power sources is highly desirable for patient comfort. The intensively explored energy harvesting strategy currently offers new options for self-powered iontophoresis devices, yet with limitations. Microneedle patches are transdermal patches with microscopic needles that penetrate the epidermis deep enough to help drugs enter the bloodstream. One-layer medication in an adhesive in this kind, the drug is contained in the adhesive layer. In addition to holding the different layers together, the adhesive layer delivers the medication to the skin. A backing and a temporary liner encircle the adhesive layer. The 20 ?m thickness of the patch permits the passage of biomolecules up to 20 ?m in size through the gap of 100–1000 ?m tips in a tiny needles patch. Two kinds of needles are used: those dissolved in water syringes composed of soluble polysaccharides or sugars and water-insoluble needles made of metal, ceramic or polymer[30,31]. In Figure 3(a) and Figure 3(b), components of iontophoresis and microneedle-type transdermal patches are presented.


Vapour patches and other advanced types
In addition to holding the different surfaces together, the adhesive layer-containing patch also acts as a vent for the vapor. Vapor patches are frequently used to release essential oils (ex. Eucalyptus oil, Peppermint oil) for up to 6 hours during decongestion. There are numerous other kinds of vapor patches on the market that are intended to lessen the conditions associated with cigarette smoking and enhance the quality of sleep. Recently many advances in transdermal patches, which include the development of smart, dissolving/biodegradable, high-loading/release and 3D-printed patches, etc.[32,33]
LABORATORY PREPARATION STAGES AND METHODS OF SKIN PATCHES
The general steps involved in the preparation of transdermal patches in the laboratory include the below[34].
Formulation preparation:
Accurately weigh and dispense the active ingredient/s, excipients and adhesive materials in a suitable container. To achieve a uniform dispersion, mix the ingredients using the proper tools, such as mixers and homogenizers using controlled temperature and stirring. Conduct compatibility studies to make sure the formulation is stable and effective.
Putting on a coat or layer:
Using coating or lamination machines, apply the drug-containing formulation onto a backing material. To guarantee dependable medication delivery, regulate the coating's thickness and homogeneity. Use different coating techniques, such as knife coating, roller coating, or hot melt coating, depending on the formulation characteristics.
Desiccation:
To get the correct consistency and get rid of solvents, dry the coated or laminated material. To avoid overheating or uneven drying, use ovens or drying chambers with controlled temperature and airflow.
Die-cutting:
Use die-cutting machines to cut the dried material into individual patches of the required size. The size of the patch should accommodate the necessary therapeutic active drug of claimed quantity and shape of market acceptable. To create patches with constant drug content, make sure to cut precisely and consistently.
Quality assurance:
To guarantee the patches' quality, potency, and uniformity, conduct quality control tests at different phases of the manufacturing process. Stability studies, adhesive strength, thickness measurement, drug release kinetics, and content homogeneity are a few examples of test types. For quality control, use analytical tools like spectrophotometers, thickness gauges, peel testers, tensile strength testing devices and dissolution testers.
Packaging:
Using packaging tools like pouch sealers, blister packaging machines, and cartoners, pack each patch into a pouch, blister or pouch pack in a carton. Assure correct labeling and packaging in compliance with legal specifications. Put precautions in place to shield the patches from contamination, light, and moisture during packing.
Sterilization, if necessary:
Use techniques like ethylene oxide sterilization or gamma irradiation to sterilize the patches, depending on the drug's characteristics, application types and regulatory requirements. To preserve the integrity and security of the patches, make sure the sterilization equipment and procedure are properly validated.
Final exam and discharge:
Verify that the packaged patches comply with all legal and quality standards by performing a final inspection. After ensuring that the batches have passed quality control tests and meet all requirements, release them for distribution.
Below are some of the methods adopted for the manufacturing of transdermal patches in the laboratory [35-37].
Asymmetric TPX membrane method
These are fabricated by using the dry/wet inversion process. TPX (4-methyl-1-pentene) is dissolved in a mixture of solvent (cyclohexane) and nonsolvent additives at 60°C to form a polymer solution. The polymer solution is kept at 40°C for 24 hrs and cast on a glass plate to a pre-determined thickness with a Gardner knife. After that the casting film is evaporated at 50°C for 30 sec, then the glass plate is to be immersed immediately in a coagulation bath (maintained the temperature at 25°C). After 10 minutes of immersion, the membrane can be removed, air dry in a circulation oven at 50°C for 12 hrs.
Circular-Teflon mold method
Solutions containing polymers in various ratios are used in an organic solvent. The calculated amount of the drug is dissolved in half the quantity of the same organic solvent. Enhancers in different concentrations are dissolved in the other half of the organic solvent and then added. Di-N-butyl phthalate is added as a plasticizer into a drug-polymer solution. The total contents are to be stirred for 12 hrs and then poured into a circular teflon mold. The molds are to be placed on a leveled surface and covered with an inverted funnel to control solvent vaporization in a laminar flow hood model with an air speed of 0.5 m/s. The solvent is allowed to evaporate for 24 hrs. The dried films are to be stored for another 24 hrs at 25±0.5°C in a desiccator containing silica gel before evaluation to eliminate aging effects. The dried film is kept in silica gel-filled desiccators to prevent the effects of aging. This kind of film can be evaluated a week after it is produced.
Mercury substrate method
This procedure involves dissolving the medication and plasticizer in the polymer solution. After agitating it for 10 to 15 minutes to form a homogeneous dispersion, it was transferred onto a level mercury surface and covered with an inverted funnel to regulate the evaporation of the solvent.
IPM membranes method
This approach involves dispersing the medication in a solution of water and propylene glycol that contains carbomer 940 polymers, then stirring the mixture with a magnetic stirrer for 12 hours. The addition of triethanolamine is intended to neutralize the dispersion and increase its viscosity. If the drug is very poorly soluble in aqueous solution, buffer pH 7.4 can be used to obtain solution gel. The gel that has developed will be integrated into the IPM membrane.
EVAC membranes method
Polyethylene (PE) and ethylene vinyl acetate copolymer (EVAC) membranes, as well as 1?rbopol reservoir gel, can be utilized as rate control membranes to set up the target transdermal therapeutic system. Propylene glycol is used to prepare gel if the medication is not soluble in water. The medication is dissolved in propylene glycol, and then carbopol resin is added. The mixture is then neutralized with a 5% w/w sodium hydroxide solution. A sheet of backing layer covering the designated region is covered with the medicine (in gel form). The gel will be covered with a rate-regulating membrane, and the edges will be heated to seal the device and prevent leaks.
Aluminium-backed adhesive film method
When transdermal methods produce unstable matrices and if the loading doses are more than 10 mg, the adhesive film supported by aluminium is used. This process makes use of chloroform as a choice of solvent because most of the drugs as well as adhesives are soluble in chloroform. The drug is dissolved in chloroform and adhesive material will be added to the drug solution and dissolved. An aluminium former that is custom-made is lined with aluminium foil and the split ends are sealed off with cork blocks that fit tightly.
Proliposomes method
The Proliposomes are prepared by carrier method using the film deposition technique. The medicament and lecithin in the established ratio (about 0.1:2) can be used. For the preparation, the required quantity of mannitol powder is taken in a round bottom flask which is kept at 60-70°C temperature and the flask is rotated at 80-90 rpm and dried the mannitol at vacuum. After drying, the temperature of the water bath is adjusted to 20-30°C. Drug and lecithin are dissolved in a suitable organic solvent mixture in the established ratio (about 0.1:2), and a 0.5ml aliquot of the organic solution is introduced into the round-bottomed flask at 37°C after complete drying second aliquots (0.5ml) of the solution is to be added. After the last loading, the flask containing proliposomes are connected in a lyophilizer and subsequently drug loaded mannitol powders (proliposomes) are placed in a desiccator over night and then sieved through 100 mesh. The collected powder is transferred into a glass bottle and stored at the freeze temperature until characterization and formulation into TDDS.
Free film method
Free film of cellulose acetate is prepared by casting it on a mercury surface. A polymer solution of 2% w/w is to be prepared by using chloroform. Plasticizers are to be incorporated at a concentration of 40% w/w of polymer weight. Five ml of polymer solution was poured in a glass ring which was placed over the mercury surface in a glass petridish. The rate of evaporation of the solvent is controlled by placing an inverted funnel over the petridish. The film formation is noted by observing the mercury surface after complete evaporation of the solvent. The dry film will be separated out and stored between the sheets of wax paper in a desiccator until use. Free films of different thickness can be prepared by changing the volume of the polymer solution.
SCALE UP FROM R&D TO COMMERCIAL
Product development is considered successful if the laboratory-developed formula and process need to be executed without any issues at a higher scale during commercial for market sale. Also, it is mandatory to make the robust method of manufacturing to obtain the expected yield with quality products consistently to upsurge the profit.
Quality by Design (QbD)
A more seamless transition to commercial production is made possible by applying QbD principles during the R&D stage. Designing reliable and consistent processes and comprehending how process parameters affect product quality are key components. During transdermal product development, the QbD tools include risk assessment, design of experiments, control strategy, and product life cycle monitoring. Before initiating the laboratory trials the QbD elements like QTPP (Quality target product profile) and CQAs (critical quality attributes) that include process parameters and material attributes need to be in place for making the design space and control strategy. Continual improvement will be a part of development at all stages of developing the film formulation.
Technology Transfer
It's critical to transfer the transdermal technology from R&D to manufacturing facilities in an efficient manner. This entails the transfer of procedures, documentation, and knowledge while maintaining uniformity and regulatory compliance. Before scaling up, a thorough understanding of the R&D process is necessary. Process optimization and understanding are inevitable for determining the crucial process variables, comprehending how they affect the caliber of the final product, and scalability-maximizing the process. Selection of the right machinery or equipment for commercial production of transdermal batches and validation is crucial. Larger volumes should be handled by the equipment while keeping process parameters intact. Equipment validation guarantees dependable and consistent operation of the machinery. While scaling up the transdermal formulations the personnel requirements like qualification, experience and training; space requirements for administration and office, testing area; equipment floor; storage area of approved and unapproved raw materials, packing materials, in-process and finished dosage forms; quarantine area; review of the formula; raw materials; equipment; rate of manufacturing; manufacturing process evaluation; master manufacturing procedure; product stability; and standard testing procedures are necessary to be considered[38-39].
Critical properties
The fundamental features of patch adhesion are described by tack, shear adhesion and peel adhesion. ‘Tack’ relates to the ability of an adhesive to form the initial bond with an unlike substrate on brief contact and under light pressure. ‘Shear adhesion’ or ‘holding power’ defines the resistance of the matrix to flow. ‘Peel adhesion’ refers to the force required to peel away the patch from an adherent[40-42]. The patch needs to be carefully applied onto the skin and, therefore, low-tack PSAs are required. The shear adhesion property has to guarantee that the PSA will remain attached to the skin for a specific period despite tangential stresses caused by both body movements and cloth frictions. The peeling-off procedure should be easy and painless, without leaving patch residues and causing skin damage. These features depend on both the critical surface energy and the viscoelastic properties of PSAs. By separating PSA adhesion in bonding and debonding steps, two mechanisms are involved: the former is due to the viscous flow proceeding by biased diffusion via free volume and the latter is caused by the elastic distortion, which stores free energy. Knowledge on these three properties are important during the development and scaling.
Tack:
In addition to being influenced by rheological characteristics at low frequencies, the initial bonding of a PSA onto an adherend usually happens in a fraction of a second and is the result of molecular interactions at the adhesive/adherend interface. The PSA performance is primarily determined by the visco-elastic properties of the adhesive material, or the rate of wetting, in particular when the PSA's surface energy is significantly lower than the adherend. On the other hand, for low-energy surfaces, the substrate's wetting is dependent on the PSA critical surface tension, which is typically in the 28–32 dyne/cm range. Wetting and tack are negatively correlated with the adherend's critical surface value. The skin surface energy is correlated with its hydro-lipidic balance; values documented in the literature varied from approximately 25 dyne/cm for dry skin to 56 dyne/cm when the skin's temperature and relative humidity increased. Therefore, in addition to physio-pathological conditions, gender and age have a significant impact on PSA tack performances. On the other hand, a patch needs low tack values when it is precisely applied to the skin. The tack methods measure the force of debonding following a brief contact time and light pressure application because it is challenging to determine the time required to achieve optimal adhesion. The bond-making and bond-breaking processes are combined in the rolling ball tack tests.
Shear adhesion or holding power:
Shear adhesion indicates a PSA's ability to withstand tangential stresses and, consequently, the matrix's cohesiveness. The shear adhesion techniques calculate the force needed to remove a standard patch area from an adherent plate, a standard flat surface, in a direction perpendicular to the surface it is attached to. By measuring the amount of time needed to remove a standard area of the patch from the adherend plate under a standard load, these static tests indirectly quantify the force needed to skid the patch on the adherend plate. The adhesive should fail cohesively in the holding power tests, leaving an adhesive layer on the backing layer or adherend plate. The outcomes can only be regarded as an accurate indicator of the adhesive's internal strength if this mode of failure materializes. The number of shearing layers increases with adhesive thickness, resulting in a decrease in matrix cohesion. Thus, there exists an exponential relationship between the holding power and the matrix thickness of patches.
Peel adhesion:
One of the most important characteristics of patches is their ability to peel off; the more firmly a peel adheres, the more painfully a patch can be removed. Since peel resistance is not always correlated with intrinsic adhesiveness, it should not be taken for granted that it expresses the strength of the adhesive bond. The backing layer and the patch matrix must be bent and extended before the detachment can occur, which is a difficult procedure. Because of this, the total force needed to remove a patch from the adherend is far greater than the force needed to keep it in place. The various ways that patches from a rigid surface fail can be viewed as a measure of the adhesion and cohesiveness of the matrix and the adhesion to the backing layer. Prediction of patch in-vivo adhesive performances. The percentage of the dosage form that remained adhered to the skin for the duration of the application is typically used to assess the in vivo adhesive performances of a patch during clinical studies; this is known as the "patch survival rate." More appropriately, a scoring system has been proposed based on the users'/patients' subjective considerations and observations about the patch's permanence and behaviour during detachment.
COMMERCIAL MANUFACTURING PROCESS OF PATCHES
The commercial production of transdermal patches is a continuous process and consists of three stages. Custom-made equipment is installed as per user requirements. Designing of user requirements based on product type and volume of proposed manufacturing quantity.
Stage 1. Mixing:
It represents the beginning of the manufacturing process and its objective is to achieve the integration of the active and non-active ingredients that make up the formulation. The first step is to fraction and weight each of the materials that will be part of the mixture, according to what is established in the production methodology. API (Active Pharmaceutical Ingredient) and functional and non-functional excipients are involved in this process. The semi-finished product resulting from this phase is the mix according to the formulation. At this stage it is important to control the correct dissolution and dispersion of the components to guarantee the homogeneity of the adhesive mixture necessary to ensure the correct dosage and that all the units produced are effective and safe because of the controlled release of the active ingredient.
Stage 2. Coating, Drying and Laminating:
Once the mixture is obtained, the remaining process consists of three sub-stages: first is the coating, which is a continuous process where the mixture is uniformly dispensed on the release liner. Subsequently, both components go through various drying stations to evaporate the volatile components of the mixture to obtain the “adhesive mixture”. Finally, both components are joined at the exit of the drying stations with the backing film, thus obtaining the multilayer system that forms the transdermal system (backing film-adhesive matrix-release liner). Typically, the raw materials for this phase are: the mixture (semi-finished resulting from the previous stage), the release liner and the backing film. Obtaining the resulting semi-finished product: one or more laminate rolls. At this stage, it is important to control the weight of the adhesive matrix dispensed per unit area and the adhesive properties of the matrix. In this way, a correct adhesion of the patch at the place of application and a correct dosage of the drug is guaranteed, and consequently the safety, efficiency and quality of the drug.
Stage 3. Die-cutting and packaging:
In this last stage, the shape of the patch itself is obtained with the surface established according to the dose. This process is carried out by die cutting the layers obtained in the previous process where several cuts are generally made, one of them being the cut for easy detachment, therefore allowing the patient to open the patch and then apply it on the safer and more practical area of the skin. The raw materials that feed this process, in chronological order of their use, are the following: the laminate obtained in the previous stage, release liner, foil for making envelopes and other necessary packaging material. In this process, the appearance of the patches is controlled to ensure that the cuts are made correctly, as well as any other aesthetic abnormality of the patch that puts the quality of the units produced at risk. Additionally, quality control is carried out on the heat-sealed envelopes, thus guaranteeing the hermetic protection of the patches, ensuring their quality throughout their useful life.
EVALUATION TESTS OF TRANSDERMAL PATCHES
Transdermal patches can be subjected to preliminary screening followed by evaluating their physicochemical properties, in-vitro dissolution, in-vitro permeation, skin irritation and stability studies[43-45].
Preliminary screening
The microscopic pictures of transdermal patches is observed using an electronic microscope with a digital camera to determine the surface of the films formed and the uniform dispersion of drug and polymer. The effect of various polymers used in the process can be checked.
Physicochemical properties
Thickness of the patch:
The thickness of the drug-loaded patch is measured at different points (>5) by using a digital micrometer and determines the average thickness and standard deviation for the same.
Weight uniformity:
The prepared patches are to be dried at 60°C for 4 hrs before testing. A specified area of the patch is to be cut into different parts of the patch and weighed in a digital balance. The average weight and standard deviation values are to be calculated from the individual weights.
Folding endurance:
A strip of a specific area is to be cut evenly and repeatedly folded at the same place till it breaks. The number of times the film could be folded at the same place without breaking is to be noted as folding endurance.
Percentage moisture loss:
The prepared films are to be weighed individually and kept in a desiccator containing fused calcium chloride at room temperature for 24 hrs. After 24 hrs the films are to be reweighed and determine the percentage moisture content from the below-mentioned formula.
Percentage moisture loss = Initial weight - Final weight x 100
Final weight
Percentage moisture uptake:
The weighed films are to be kept in a desiccator at room temperature for 24 hrs containing a saturated solution of potassium chloride to maintain 84% RH. After 24 hrs the films are to be reweighed and determine the percentage moisture uptake from the below-mentioned formula.
Percentage moisture uptake = Final weight- Initial weight x 100
Initial weight
Water vapor permeability test:
Water vapor permeability can be determined with the foam dressing method the air-forced oven is replaced by a natural air circulation oven. This can be determined by the following formula
Water vapor permeability (gm/m2 per 24hrs) = W/A
W = amount of vapor permeated through the patch and
A = surface area of the exposure samples (in m2).
Drug content:
A specified quantity of patch is to be dissolved in a suitable solvent and sonicate for complete extraction of drug from the patch and made up to the mark with same. The resulting solution was allowed to settle for about an hour, and the supernatant was suitably diluted to give the desired concentration with a suitable solvent. The solution was filtered using 0.2 micrometer membrane filter and analyzed by a suitable analytical technique (UV or HPLC) and the drug content is estimated.
Uniformity of dosage unit test:
10 patches are selected and content is determined for individual patches. If 9 out of 10 patches have content between 85% to 115% of the specified value and one has content not less than 75% to 125% of the specified value, then transdermal patches pass the test of content uniformity. But if more than one patch has content in the range of 75% to 125%, then an additional 20 patches are tested for drug content. If these 20 patches range from 85% to 115%, then the transdermal patches pass the test.
Morphology examination:
This test is to be performed to examine the drug crystals from the patch by polariscope. A specific surface area of the piece is to be kept on the object slide and observe for the drug crystals to distinguish whether the drug is present in crystalline form or amorphous form in the patch.
Shear adhesion test:
This test is to be performed for the measurement of the cohesive strength of an adhesive polymer. It can be influenced by the molecular weight, the degree of crosslinking and the composition of polymer, type and the amount of tackifier added. An adhesive-coated tape is applied onto a stainless steel plate; a specified weight is hung from the tape, to affect it pulling in a direction parallel to the plate. Shear adhesion strength is determined by measuring the time it takes to pull the tape off the plate. The longer the time takes for removal, the greater is the shear strength
Peel adhesion test:
In this test, the force required to remove an adhesive coating from a test substrate is referred to as peel adhesion. The molecular weight of the adhesive polymer, and the type and amount of additives are the variables that determine the peel adhesion properties. A single tape is applied to a stainless steel plate or a backing membrane of choice and then the tape is pulled from the substrate at a 180º angle, and the force required for tape removal is measured.
Thumb tack test:
It is a qualitative test applied for tack property determination of adhesive. The thumb is simply pressed on the adhesive and the relative tack property is detected.
Flatness test:
Three longitudinal strips are to be cut from each film at different portions like one from the center, the other one from the left side, and another one from the right side. The length of each strip was measured and the variation in length because of non-uniformity in flatness was measured by determining percent constriction, with 0% constriction equivalent to 100% flatness.
Percentage elongation break test:
The percentage elongation break is to be determined by noting the length just before the break point, the percentage elongation can be determined from the below-mentioned formula.
Elongation percentage = L1-L2 x 100
L2
Where, L1 - final length of each strip, L2 - initial length of each strip.
Rolling ball tack test:
This test measures the softness of a polymer that relates to talk. In this test, a stainless steel ball of 7/16 inches in diameter is released on an inclined track so that it rolls down and comes into contact with horizontal, upward-facing adhesive. The distance the ball travels along the adhesive provides the measurement of tack, which is expressed in inches.
Quick stick (peel-tack) test:
In this test, the tape is pulled away from the substrate at 90ºC at a speed of 12 inches/min. The peel force required to break the bond between adhesive and substrate is measured and recorded as tack value, which is expressed in ounces or grams per inch width.
Probe tack test:
In this test, the tip of a clean probe with defined surface roughness is brought into contact with the adhesive, and when a bond is formed between the probe and the adhesive. The subsequent removal of the probe mechanically breaks it. The force required to pull the probe away from the adhesive at a fixed rate is recorded as tack and it is expressed in grams.
In vitro drug release studies
The paddle-over disc method (USP apparatus V) can be employed for the assessment of the release of the drug from the prepared patches. Dry films of known thickness are to be cut into definite shapes, weighed, and fixed over a glass plate with an adhesive. The glass plate was then placed in a 500-mL of the dissolution medium or phosphate buffer (pH 7.4), and the apparatus was equilibrated to 32± 0.5°C. The paddle was then set at a distance of 2.5 cm from the glass plate and operated at a speed of 50 rpm. Samples (5- mL aliquots) can be withdrawn at appropriate time intervals up to 24 h and analyzed by UV spectrophotometer or HPLC. The experiment is to be performed in triplicate and the mean value can be calculated.
In vitro skin permeation studies
An in vitro permeation study can be carried out by using a Franz diffusion cell apparatus. Phosphate buffer solution (pH 7.4) was filled in the receptor compartment up to 12 mL or necessary volume. The temperature of the cell was maintained at 32 ± 0.5°C using a thermostatically controlled heater. The donor compartment was placed over the receptor compartment and both compartments were kept in position with the help of the stainless steel clamp. To avoid evaporation, the junction of the two compartments was wrapped with adhesive tape. The whole assembly was kept on a magnetic stirrer and the receptor fluid was kept stirring continuously during the test by using magnetic bars at specified rpm. The isolated rat or rabbit skin piece is to be mounted between the compartments of the diffusion cell, with the epidermis facing upward into the donor compartment. A sample volume of definite volume is to be removed from the receptor compartment at regular intervals, and an equal volume of fresh medium is to be replaced. Samples are to be filtered through a filtering medium and can be analyzed spectrophotometrically or HPLC. The cumulative amount of the drug permeated for the patch formulations has been calculated. Flux can be determined directly as the slope of the curve between the steady-state values of the amount of drug permeated (mg/cm2) vs. time in hours and permeability coefficients were deduced by dividing the flux by the initial drug load (mg/cm2).
Skin irritation study
Skin irritation and sensitization testing can be performed on healthy rabbits (average weight 1.2 to 1.5 kg). The dorsal surface (50cm2) of the rabbit is to be cleaned and remove the hair from the clean dorsal surface by shaving and cleaning the surface by using rectified spirit and the representative formulations can be applied over the skin. The patch is to be removed after 24 hr. and the skin is to be observed and classified into 5 grades based on the severity of skin injury.
Stability studies
Stability studies are to be conducted according to the ICH guidelines by storing the TDDS samples at 40±0.5°C and 75±5% RH for 6 months. The samples were withdrawn at 0, 30, 60, 90 and 180 days and analyzed for the drug content.
REGULATORY STRATEGY AND FUTURE OF TRANSDERMAL THERAPY
Standard irritation and sensitization studies should be performed with the patch itself in animals/humans for investigational and new submissions for transdermal patches. Negotiate the timing and implementation of the toxicology requirements. The dermatology division at the FDA should review dermal aspects of the IND and new drug Application (NDA). The primary review should occur at the division that handles the indication under study. Dose-ranging studies are required in Phase 2. A single Phase 3 study could be negotiated. U.S. Food and Drug Administration classifies transdermal patches as a combination product, consisting of a medical device combined with a drug or biological product that the device is designed to deliver. Prior to sale in the US, any transdermal patch product must apply for and receive approval from the FDA, demonstrating safety and efficacy for its intended use[46-48]. The market size of transdermal skin patches is estimated at USD 8.92 billion in 2024, and is expected to reach USD 11.33 billion by 2029, growing at a CAGR of 4.87% during the forecast period (2024-2029). The nicotine patch revolutionized smoking cessation; patients were being treated with nitroglycerin for angina, clonidine for hypertension, scopolamine for motion sickness, and estradiol for estrogen deficiency, all through patches. At that time, biotech medicine was still being developed. During the past decade, the number of drugs formulated in the patches has hardly increased, and there has been little change in the composition of the patch systems. Modifications have been mostly limited to refinements of the materials used. The reason is that only a limited number of drugs fit the molecular weight and potency requirements for transdermal absorption. In Table 3, examples of well-known market-available products which are used for the treatment of various ailments are shown.
Table 3: Examples of marketed transdermal film formulations.

CONCLUSION
Transdermal drug delivery offers significant benefits such as reduced side effects, improved in-vivo bioavailability, patient convenience and simplified dosing regimens. Many advances in transdermal technology continue to enhance the effectiveness and applicability of transdermal patches, making it a promising option in modern pharmaceutical therapy. Transdermal patches have the potential to provide an effective means of drug delivery for a variety of ailments, but some challenges lie ahead, such as the possibility of self-inflicted toxicity due to improper dosing, poor adhesion, low drug penetration, a potential trigger for skin irritation, or patch failure. Careful consideration of drug properties and formulation components is essential to overcome the limitations associated with the development and commercial manufacturing of patches. All of this warrants further research and development to optimize the safety and efficacy of this delivery system. Novel approaches in formulation development, process or manufacturing technology and regulatory strategies are constantly being explored to overcome the issues associated with these routes of delivering drugs. This review will serve as a connecting bridge between the current knowledge and future conducting R&D work on transdermal delivery for treating patients suffering from many ailments using existing and new chemical entities in a variety of therapeutic areas.
REFERENCES


Mahesh Kumar T , Vetrivel Rajan M , Gowsalya K, A Comprehensive Review On Complexities And Directions Of Drug Delivery Using Transdermal Patches, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 9, 533-552. https://doi.org/10.5281/zenodo.13737874
 10.5281/zenodo.13737874
10.5281/zenodo.13737874
